
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is an acknowledged contributor to universal fatality and morbidity. Using biomarkers to pinpoint its phenotypes is crucial, enabling individualized treatment and enhancing prognosis.
Objective
Studying the steadiness of blood eosinophi1s in cases who experienced repeated hospital admissions for acute worsening of COPD during a year and its correlation to the treatment plan.
Methods
A retrospective cohort study includes 270 COPD male patients with acute exacerbations. The patients were divided into three groups: fluctuating (ranges between ≥ 150 cells/ul and < 150 cells/ul), non-EOS (< 150 cells/ul), and Eosinophil (EOS) (≥ 150 cells/ul).
Results
Most patients were in the fluctuating blood EOS group (53.3%). The median length of hospital stay was longer in the fluctuating group (5 days). There was a significant positive correlation between the number of exacerbations and both EOS count and EOS/WBCs. A higher eosinophilic count was associated with an increased risk of eosinophilic exacerbations. Most patients used steroids (higher in the EOS group, 61.6%).
Conclusion
Blood eosinophilic count is promising for investigating acute COPD exacerbations. Peripheral blood eosinophilia is a relevant biomarker for directing the management of COPD exacerbations, including steroids.
Similar content being viewed by others

Background
Chronic obstructive pulmonary disease (COPD) is an acknowledged contributor to universal fatality and morbidity [1, 2]. Due to its significant heterogeneity, the prognosis and responsiveness to treatment will vary among patients with various phenotypes. Hence, it is crucial to use biomarkers to pinpoint particular COPD phenotypes, enabling individualized treatment and thereby enhancing prognosis [3]. Exacerbation of COPD is the primary cause of severity due to deterioration of the patient’s respiratory symptoms [2]. Repeated infective exacerbations in patients with COPD lead to an increasing incidence of morbidity and enhanced mortality [4]. The patients’ complete recovery has far-reaching post-exacerbations, which plays an essential prognostic role in COPD because it indicates gradually rising risk [2]. COPD may be difficult to distinguish in clinical practice with other airway disease, particularly asthma. In addition, some patients may exhibit features of both diseases [5]. In COPD patients, eosinophilic airway inflammation is linked to exacerbations and responsiveness to corticosteroids, proposing possible similar pathways with eosinophilic asthma [6]. Patients may exhibit this inflammatory pattern due to concomitant asthma [7]. However, it is still uncertain how eosinophils contribute to COPD and why only some patients experience eosinophilic airway inflammation [8]. This has piqued researchers’ curiosity as a possible treatment target for inhaled corticosteroid therapy. The Global Initiative for Chronic Obstructive Pu1monary Disease 2023 report suggests using blood eosinophil counts to direct treatment for both new diagnoses classified as GOLD E and those who exacerbate despite bronchodilatation [9]. B1ood eosinophi1s (EOS) have been suggested as a substitute biomarker and therapeutic mentor for determining the kind of airway inflammation due to the restricted accessibility of sputum induction in clinical practice. Nevertheless, blood EOS’s stability is debatable because of all the variables it is susceptible to [8]. Periodic reassessment of COPD patients is crucial to avoid misdiagnosis and overtreatment [5]. So, predicting the prognosis of COPD from a single-blood EOS count appears to be imprecise. On the other hand, over a year, blood EOS in patients with acute exacerbation COPD is considered reasonably constant [10]. Prior findings recommended that the presence of elevated blood eosinophil levels (≥ 2%, corresponding to ≥ 150 cells/l) is an appropriate biomarker for predicting the likelihood of frequent exacerbations and preventing them via the administration of inhaled steroids [3].
Systemic corticosteroids can reduce circulating eosinophils, resulting in a smaller proportion of eosinophils and increasing circulatory neutrophils. Hence, an alteration in patients from the eosinophilic group into the non-eosinophilic group due to prior corticosteroid treatment led to an underestimated detected impact [11].
The aim of our study is to investigate the steadiness of blood eosinophi1s in cases who experienced repeated hospital admissions for acute worsening of COPD during a year and its correlation to the treatment plan.
Subjects and methods
Study design and subject’s enrollment
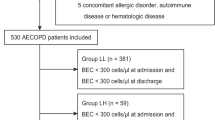
A retrospective cohort study included 270 COPD patients with acute exacerbations previously admitted to the Chest Diseases Department at Port Said University Hospital; all were males. The patients were diagnosed as COPD according to GOLD 2023 criteria [9]. The study was conducted over 1 year, from August 2022 to August 2023. The study protocol was approved by the local institutional review board (IRB) of the Faculty of Medicine, Port Said University (ERN: MED (1/5/2023) S.no (87) CHS_001).
Depending on the EOS blood level, 150 cells/ul was utilized as a checkpoint, and our patients were divided into three groups as follows:
-
▪ EOS group: (≥ 150 cells/ul), which included 86 patients.
-
▪ 40 individuals were included in the non-EOS group (< 150 cells/ul).
-
▪ 144 individuals were included in the fluctuating group, which had a range of ≥ 150 to < 150 cells/ul.
We picked a cut-off value of 150 cells/ul, which is among the published normal range and was utilized as the defined threshold in most research. Moreover, it is sensitive to predicting eosinophilic airway inflammation and exacerbations [12, 13].
Inclusion and exclusion criteria
The study included adult patients (older than 18 years) with COPD who fulfill the criteria for a diagnosis of chronic obstructive pulmonary disease acute flare-ups (minimally two exacerbations/year) [9]. Exacerbations were attributed to either infectious causes (bacterial or viral), or environmental causes (air pollution or smoking). At the same time, patients with bronchial asthma associated with elevated EOS, allergenic illness, parasitic infection, or additional conditions that may enhance blood EOS level (Addison’s disease, skin disorders (eczema, pemphigus), autoimmune disorders (SLE, sarcoidosis), tumors (leukemia, Hodgkin lymphoma)) were excluded. Moreover, patients with severe cardiac diseases associated with severe hepatic and renal problems or patients using maintenance treatment of systemic corticosteroids for more than 30 days were ruled out (part of patients used ICS before admission but the other remaining part did not).
Data collection
The data collected from the enrolled patients involved medical history (including smoking history, hospita1ization, rate of exacerbations/year, use of corticosteroids, and concurrent disorders), and anthropometric measures, including weight, height, and calculated body mass index (BMI); the outcome was noted.
Laboratory results for CBC (using Mindray BC 3200 device) were recorded. The 1oad of EOS in the peripheral b1ood was investigated within 24 h after admission and on the second exacerbation within the same year.
Data analysis
Data analysis was performed by Statistical Package for the Social Sciences (SPSS version 25; SPSS, Inc., Chicago, IL, USA) statistical software. Numbers and percentages were used to describe the qualitative data. For non-normally distributed data, the median (lowest and maximum) and mean ± were used to characterize the quantitative data. Standard deviation for data is regularly distributed following the Kolmogrov-Smirnov test for normalcy. The acquired results were deemed significant at the ≤ 0.05 level. When necessary, Monte Carlo, Fisher exact, and Chi-square tests were performed to compare qualitative data between groups. Mann–Whitney U and Kruskal–Wallis tests were used to compare two groups and more than two groups for non-normally distributed data.
-
Student t-test was used to compare two independent groups for normally distributed data.
-
One-way ANOVA test compared more than two independent groups with the post hoc Tukey test to detect pair-wise comparison.
-
Spearman’s rank-order correlation determined the strength and direction of a linear link between two continuous variables with non-normal distribution or ordinal variables.
Results
The study included 270 adult COPD patients, all were males, with acute exacerbations recruited retrospectively. When categorized according to blood eosinophil (EOS) level, the majority of the patients were in the fluctuating blood EOS group (53.3%), followed by the EOS group (31.9%), and then the non-EOS group (14.8%). The descriptive data and comparisons for the epidemiological, clinical, and laboratory characteristics among the total study participants and the categorized groups are illustrated in Table 1.
The higher eosinophilic count was associated with an increased risk of eosinophilic exacerbations, as revealed by the significant positive correlation between the number of exacerbations and both EOS count and EOS/WBCs (Table 2).
Moreover, higher blood eosinophilic count and higher eosinophils/WBCs ratio were associated with increased utilization of steroids without a statistically significant difference (Table 3).
Discussion
Regarding the prevalence of patients when categorized according to blood EOS level, the majority of the patients were in the fluctuating blood EOS group (53.3%), followed by the EOS group (31.9), then the non-EOS group (14.8%). However, clinical studies and population-based research investigating the distribution pattern of blood eosinophils in patients with COPD usually observed that the vast majority of COPD patients possessed a blood eosinophil level “constantly exceeding” 150 cells/l [14]. This may be explained as we have excluded all causes that may lead to eosinophilia, such as bronchial asthma, allergic diseases, or parasitic infections that were not usually adopted in prior studies. The patients’ blood eosinophilic count probably fluctuated as during the follow-up, there may be more substantial variations in disease stability or adjustments in pharmacologic COPD therapy.
Concerning age, the subjects were elderly, especially in the non-EOS group (68.13 ± 9.08 years), with no difference among groups.
There was male predominance since, in Egypt, the majority of smokers are of male gender. This was in agreement with Ko and his colleagues. who found that the participants were predominantly men and aged 74.9 ± 7.8 years [15].
For BMI, the mean was higher in the EOS group (31.36 ± 4.89 kg/m2) (obese) without a significant difference among groups. This agreed with a study that showed that the likelihood of developing eosinophilic COPD was increased in people with more considerable body mass indices [16].
Most patients were current smokers, with no statistical difference between the three groups. The median pack/year index was higher in the non-EOS group (68 (22–136)). This agrees with a study in which the number of current smokers was somewhat higher in people with eosinophils of 2% or greater. However, the two groups’ pack-years of smoking were not significantly different [17]. Despite prior research revealing that the percentage of current smokers was lower among patients with relative eosinophilia, smoking habits did not influence the stability of blood eosinophils in COPD [18].
Most patients experienced minimally two exacerbations/year to ensure the stability of blood eosinophils [19].
The mean length of hospital stay was longer in the fluctuating group, 5 days without statistical significance. This agreed with Ko and his coworkers, who revealed that the individuals’ median length of hospital stay throughout their hospitalization was five days [15].
Fortunately, all the patients were improved. This may be attributable to close observation and early hospitalization.
Statistically significant positive correlation between number of exacerbations and EOS count. Furthermore, a statistically significant positive association exists between EOS/WBCs and the number of exacerbations. This means that a higher eosinophilic count was associated with an increased risk of eosinophilic exacerbations. This agreed with Yun et al. (2018) and Couillard et al. (2017) who found that a more significant number of eosinophils increased the likelihood of COPD exacerbation [6, 20].
Most patients used inhaled steroids (higher in the EOS group, 61.6%) without a statistically significant difference. Cheng and Shih-Lung reported that inhaled corticosteroids decreased exacerbation rates by 29% among individuals with blood eosinophil levels of 2% or higher. In contrast, they reduced rates by 10% in individuals with fewer blood eosinophil levels. The investigators observed no link between blood eosinophil count and acute bronchodilator responsiveness. Furthermore, exacerbation rates increased continuously along with rising eosinophil levels in leukocytic percentage beginning at 2%, implying that blood eosinophils could be implemented as a potential indicator of upcoming COPD exacerbations. However, they claimed that patients with COPD who received ICS medication and had elevated eosinophil levels were more likely to develop pneumonia [21].
Limitations
First off, since our study is observational, some confounding variables, like pulmonary function tests, were not examined (some patients were unable to finish the tests during the study period for various medical and non-medical reasons, resulting in incomplete data), which may have an impact on the study’s findings. Second, as this is a single-center investigation, additional confirmation of some findings in a multicenter trial could be necessary.
Conclusion
The blood EOS of AECOPD patients is relatively stable over 1 year. A higher eosinophilic count was associated with an increased risk of eosinophilic exacerbations. Moreover, higher blood eosinophilic count and higher eosinophils/WBCS ratio were associated with increased utilization of steroids.
Availability of data and materials
The data produced and analyzed during the current research are available to the relevant author upon reasonable request.
References
Barnes PJ (2019) Inflammatory endotypes in COPD. Allergy Eur J Allergy Clin Immunol 74:1249–1256. https://doi.org/10.1111/all.13760
Abdelhalim HA, Aboelnaga HH (2018) Serum uric acid levels and uric acid/creatinine ratios: affordable biomarkers for predicting chronic obstructive pulmonary disease severity and exacerbations. Egypt J Chest Dis Tuberc 67:231. https://doi.org/10.4103/ejcdt.ejcdt_39_18
Tinè M, Biondini D, Semenzato U et al (2019) (2019) Reassessing the role of eosinophils as a biomarker in chronic obstructive pulmonary disease. J Clin Med 8:962. https://doi.org/10.3390/JCM8070962
Abdelhalim HA, Aboelnaga HH, Aggour RL (2018) Chronic obstructive pulmonary disease exacerbations and periodontitis: a possible association. Egypt J Bronchol 12:303–309. https://doi.org/10.4103/ejb.ejb_12_18
Aboelnaga HH (2019) The puzzle of patients awareness of having COPD. Cronicon EC Pulmonol Respir Med 3:276–277
Yun JH, Lamb A, Chase R et al (2018) Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol 141:2037-2047.e10. https://doi.org/10.1016/J.JACI.2018.04.010
Kreindler JL, Watkins ML, Lettis S et al (2016) Effect of inhaled corticosteroids on blood eosinophil count in steroid-naïve patients with COPD. BMJ Open Respir Res 3:e000151. https://doi.org/10.1136/BMJRESP-2016-000151
Mycroft K, Krenke R, Górska K (2020) Eosinophils in COPD—current concepts and clinical implications. J Allergy Clin Immunol Pract 8:2565–2574. https://doi.org/10.1016/J.JAIP.2020.03.017
Vogelmeier CC, Agusti A et al (2023) Global strategi for prevention, diagnosis and management of COPD. Report 2023:16–17
Gong Y, Sun H (2022) Stability of blood eosinophils in COPD with multiple acute exacerbations within 1 year and its relationship with prognosis. Int J COPD 17:3123–3128. https://doi.org/10.2147/COPD.S392660
Ortega H, Llanos JP, Lafeuille MH et al (2019) Effects of systemic corticosteroids on blood eosinophil counts in asthma: real-world data. J Asthma 56:808–815. https://doi.org/10.1080/02770903.2018.1502301
Citgez E, Van Der Palen J, Van Der Valk P et al (2021) Stability in eosinophil categorisation during subsequent severe exacerbations of COPD. BMJ open Respir Res 8:e000960
Zhang Y, Liang L-R, Zhang S et al (2020) Blood eosinophilia and its stability in hospitalized COPD exacerbations are associated with lower risk of all-cause mortality. Int J Chron Obstruct Pulmon Dis 15:1123–1134
Landis S, Suruki R, Maskell J et al (2018) Demographic and clinical characteristics of COPD patients at different blood eosinophil levels in the UK clinical practice research datalink. COPD 15:177–184. https://doi.org/10.1080/15412555.2018.1441275
Ko FWS, Chan KP, Ngai J et al (2020) Blood eosinophil count as a predictor of hospital length of stay in COPD exacerbations. Respirology 25:259–266. https://doi.org/10.1111/RESP.13660
Wu HX, Zhuo KQ, Cheng DY (2019) Prevalence and baseline clinical characteristics of eosinophilic chronic obstructive pulmonary disease: a meta-analysis and systematic review. Front Med 6:1–12. https://doi.org/10.3389/fmed.2019.00282
Vedel-Krogh S, Nielsen SF, Lange P et al (2016) Blood eosinophils and exacerbations in chronic obstructive pulmonary disease: the Copenhagen General Population Study. Am J Respir Crit Care Med 193:965–974. https://doi.org/10.1164/RCCM.201509-1869OC/SUPPL_FILE/DISCLOSURES.PDF
Oshagbemi OA, Burden AM, Braeken DCW et al (2017) Stability of blood eosinophils in patients with chronic obstructive pulmonary disease and in control subjects, and the impact of sex, age, smoking, and baseline counts. Am J Respir Crit Care Med 195:1402–1404. https://doi.org/10.1164/RCCM.201701-0009LE
Cui Y, Zhang W, Ma Y et al (2021) Stability of blood eosinophils in acute exacerbation of chronic obstructive pulmonary disease and its relationship to clinical outcomes: a prospective cohort study. Respir Res 22:1–12. https://doi.org/10.1186/S12931-021-01888-5/FIGURES/5
Couillard S, Larivée P, Courteau J, Vanasse A (2017) Eosinophils in COPD exacerbations are associated with increased readmissions. Chest 151:366–373. https://doi.org/10.1016/J.CHEST.2016.10.003
Cheng SL (2018) Blood eosinophils and inhaled corticosteroids in patients with COPD: systematic review and meta-analysis. Int J COPD 13:2775–2784. https://doi.org/10.2147/COPD.S175017
Funding
The authors disclose that they did not receive any funding, grants, or other forms of assistance while preparing this paper.
Author information
Authors and Affiliations
Contributions
The idea and design of the study were contributed to by all authors. Samir M. Fahyim handled the preparation of the materials as well as the data collecting and analysis. El Shaimaa Sabry Mohammed Hassan authored the original draft of the manuscript, while Hesham A. Abdelhalim revised it. Every author offered feedback on earlier drafts of the work. The final manuscript was read and approved by all writers.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study’s procedures adhered to all ethical norms of the National Institutional Review Board and the 1964 Helsinki Declaration and its later revisions. The study was approved by the local institutional review board (ERN: MED (1/5/2023) S.no (87) CHS_001).
Consent for publication
The study was waived from obtaining consent as it is a retrospective study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fahyim, S.M.M., AbdelHalim, H.A. & Hassan, E.S.S.M. Blood eosinophil variability in patients presenting with acute exacerbations of COPD within the past year and its correlation with treatment plan. Egypt J Bronchol 18, 23 (2024). https://doi.org/10.1186/s43168-024-00274-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-024-00274-1