
Abstract
Background
For various types of cancer in oncologic patients, the clinical features of pulmonary embolism (PE) are unknown. The purpose of the study is to identify pulmonary embolism incidence and type among oncologic patients along with evaluating any associated clinical variables.
Patients and methods
A prospective cohort study was conducted on 540 patients who had various types of cancers and attended to a 1-day care unit of oncology in King Fahd Hospital, Kingdom of Saudi Arabia. Chest CT with contrast and CT pulmonary angiography was applied when indicated.
Results
This study was conducted on 540 patients who have different types of cancers; among them, 24 (4.44%) developed PE. Pulmonary embolism was reported in 50% of patients who had seminoma and germ cell tumor, while in cancer larynx, it was represented in 33.4% of them. Moreover, PE was less common among patients who had cancer colon, prostate, and breast (6.68%, 4.7%, and 2.54%, respectively). Seven patients with PE (1.3%) were diagnosed incidentally during cancer staging, while 17 patients (3.14%) had symptomatic PE. Eighty-four percent of the PE cases were diagnosed within the first 6 months of cancer diagnosis, while 4/24 (16%) of the PE cases were diagnosed throughout patient follow-up within the first year of diagnosis. Chest pain and dyspnea were the common presentations in confirmed PE either symptomatic or incidental group.
Conclusions
Low-risk PE was the most frequent degree; massive and sub-massive PE was uncommon in oncologic patients. Dyspnea and chest discomfort are concerning signs of PE in cancer. Meticulous care during the first 6 months for cancer patients to pick up pulmonary embolism is recommended.
Similar content being viewed by others


Introduction
The fatality rate for patients who develop acute pulmonary embolism (PE) is high, ranging from 4.1 to 14.5%, indicating the severity of the condition [1]. When compared to non-cancer patients, cancer patients have a threefold higher risk of venous thromboembolism (VTE). Numerous factors, such as the use of newer, more potent chemotherapy drugs, have been linked to a higher probability of thrombosis [2] and increased the frequency of thrombophilia in cancer patients [3]. The majority of cancer patients have an increase in platelet activation and aggregation, as well as an upregulation of the coagulation cascade. Moreover, the coagulation activation state in cancer patients appears to be caused by a multifactorial mechanism. Tumor cells may express prothrombotic molecules and produce enzymes such as cysteine proteases, which directly result in clotting by activating factor X, as well as physiological tissue factor, which is related to the activation of the extrinsic blood coagulation pathway. Furthermore, tumor cells can contribute to clotting indirectly by secreting cytokines that act on endothelial and mononuclear cells, boosting the production of prothrombotic molecules. [4] 567.
Additionally, the incidence of PE is influenced by the type of cancer, as well the stage, type, and duration of chemotherapy, the response to therapy, an individual’s mobility, nutritional status, surgery, patient aging, and kidney and liver status [8].
Today, whereas most cancer patients are mobile and get treatment and monitoring at outpatient clinics of hospitals, PE is recognized as a serious consequence [9].
Despite many of researches on PE, it is uncertain what PE looks like clinically overall in oncology outpatients and in different forms of cancer. Numerous studies have detected PE incidence among patients who have cancer generally or among particular types of cancer [10]. Also, many of them documented the general venous thromboembolism (VTE) incidence rather than a precise type of PE. Since then, the majority of them concentrated on hospitalized patients and a few studies are exclusively focused on oncology patients when they describe the clinical characteristics of PE in outpatient clinics [11].
Advanced multi-detector computed tomography (MDCT) technology has improved pulmonary embolism detection, enhanced evaluation of the pulmonary arterial tree, and making CT pulmonary angiography the preferred imaging technique for PE diagnosis [12].
Unsuspected patients with PE who are diagnosed clinically are commonly seen on routine chest CT during their staging and follow-up, despite the fact that the modality utilized for a regular chest CT is different from that used for CT pulmonary angiography [13].
The aim of the current study is PE incidence estimation, diagnosis of various PE types, and assessment of some clinical characteristics among oncologic outpatients.
Patients and methods
The current research is a prospective study carried out on 540 cancer patients receiving care at the oncology day care unit in King Fahd Hospital, KSA, within a duration started from January 2016 to June 2020. Patients were categorized under the more advanced stage of malignancy when they had several active malignancies. The primary cancer type was documented according to the International Classification of Diseases, Ten Revision, and Clinical Modification (ICD-9–10) 2012–2016. The patients were classified into two groups (incidental group and symptomatic group).
Every patient is evaluated by a pulmonology consultant for detection of presence of any chest symptoms (cough, chest pain, expectoration, dyspnea, hemoptysis, palpitation, and syncope) for the potential of a pulmonary embolism at any time. In the current study, patients were subjected to the following:
-
1.
The different demographic data, such as age, sex, and history of smoking.
-
2.
The type, staging, and treatment strategy of primary cancer according to ICD-9–10 2012–2016.
-
3.
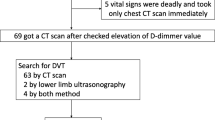
CT chest with contrast: the included patient’s chest was scanned by using a 64-row multi-detector CT scanner (Aquilion 64; Toshiba USA) in a supine position. It was carried out for all studied patients during the early staging of cancers after treatment is completed, and through patient follow-up at 3, 6, 9, and 12-month intervals according to the protocol of each type of cancer.
-
4.
CT pulmonary angiography (CTA) was done for patients who had clinical suspicion of PE. It was done for 37 patients whose modified wells criteria score was > 4 to be likely PE.
-
5.
Echo-cardiology and the level of a cardiac enzyme (serum troponin I) were carried out for patients who had submissive PE (acute PE in hemodynamic stable patients). They were done for only three patients.
-
6.
The PE degree was classified according to the European Society of Cardiology (ESC) into massive PE, sub-massive PE, and low risk [14].
-
7.
The PE time onset: It is recorded either during the initial 6 months or during the follow-up period (after 6 months).
-
8.
Treatment of PE: according to ESC guidelines [14]
-
9.
Two patients received unfractionated heparin while twenty-two patients were given fractionated one.
-
10.
One patient received thrombolytic therapy (tissue plasminogen activator (TPA) (ultiplas) with a dose of 100 mg daily.
-
11.
Two patients had IVC filters inserted; one had colon cancer and the other had laryngeal cancer. IVC filter was inserted because the patients had an anticoagulation therapy-related side effect (bleeding).
The studied patients were followed up for 1 year.
Exclusion criteria
In the current study, patients with inadequate gathered data, patients who developed PE during their hospital stay, and patients under the age of 18 were excluded.
Ethical consideration
The privacy, rights, well-being, and health of the participants were protected through informed consent, which they were asked to, read and sign if they agreed to participate in the study.
Data analysis
The data were performed by using the Statistical Package for Social Sciences version 18.0. Descriptive data were tabulated. The age of the patients, the degree and time of PE, and the type and stage of cancer were all displayed using means and standard deviations (SD). Using Fisher’s exact test, the risk of PE for patients in each cancer group was compared to that of all other patients. Using the Bonferroni correction to account for multiplicity, the incidence of PE was considered significantly different at p value < 0.0031. Furthermore, the t test and Fisher’s exact test were done to analyze the correlation with the outcome as significantly accepted at p value ≤ 0.05.
Results
This study was carried out on 540 cancer outpatients, and the cancer patients who had PE were classified into two subgroups, depending on whether the PE was clinically suspected or unsuspected.
-
1.
Symptomatic PE: the patient was clinically suspected and CT pulmonary angiography (CTA) study was carried out.
-
2.
Incidental PE: it was incidentally noticed either during the staging of cancer or follow-up using a CT scan.
Incidence of PE (symptomatic versus incidental)
The whole number and percentage of patients who had PE were 24 (4.445%); 17 patients (3.14%) had symptomatic PE while 7 patients (1.3%) had an incidental one. All patients with an incidental PE had lung, uterus, and pancreas cancer, while patients with symptomatic PE were more frequent in cancer patients with breast, prostate, colon, seminoma, and germ cell tumors, as follows: 7/8 (87.5%), 2/2 (100%), 4/5 (80%), and 2/4 (50%), respectively as shown in Fig. 1 and Table 1.

The incidence of symptomatic and incidental PE in different cancers
Demographic data and characteristics of PE in different cancer types
Seventy-five percent of PE patients were in stage VI of cancer, according to the type of cancer treatment: 100% of patients with lung and uterus cancer, seminoma, and germ cell tumor received chemotherapy; 100% of patients with prostate cancer and 25% of breast cancer received hormonal therapy, while 100% of patients with larynx and pancreas cancer; and 60% of colon cancer and 12.5% of breast cancer did not receive any medications due to cancers in late stages, and patients were deemed unfit for treatment. It was revealed that 20/24 (84%) of PE in cancer patients developed during the initial 6 months after diagnosis, 4/24 (16%) of the patients developed PE, while the remaining 4/24 (16%) developed during the first year of follow-up (2 patients have cancer prostrate, one patient has cancer larynx, and one patient has cancer breast). The majority of PE degrees (75%) were low risk, whereas massive and sub-massive PE degrees occurred in three patients (12.5%). Majority of the patients received LMWH (22/24), while one patient received thrombolytic therapy (TPA), and an IVC filter was implanted in two patients as shown in Table 2.
Clinical characteristics of both studied groups of PE (symptomatic versus incidental)
Table 3 detected that there were no significant differences in age, gender, or smoking history between the incidental and symptomatic PE groups. PE in patients who had lung and pancreas cancer were 100% incidental, while PE in patients who had prostate and larynx cancer, seminoma, and germ cell tumor were 100% symptomatic. Furthermore, the symptomatic PE incidence in breast, colon, and bladder cancer were 7/8 (87.5%), 4/5 (80%), and 1/2 (50%), respectively. On the other side, the patients with low-risk PE were represented as 100% who had incidental PE and 70.7% who had symptomatic PE. Moreover, 100% of patients with incidental PE were diagnosed during the staging of cancers within the initial 6 months while 82.5% of patients with symptomatic PE settled during chemo/hormonal therapy. The whole patients who had incidental PE received LMWH, while only one patient received thrombolytic therapy (TPA), and an IVC filter was inserted for two patients who had symptomatic PE.
Presentation of symptoms among studied groups
Table 4 shows that chest pain, cough, and dyspnea were the highest symptoms between all oncogenic patients (200,145, and 120 patients, respectively). In contrast, the less common symptoms were hemoptysis, palpitation, and syncope. In diagnosed PE, chest pain and dyspnea were higher either in the symptomatic group (88% and 82%) or the incidental group (42% and 28%).
Discussion
The frequency of suspected and unsuspected PE among oncologic outpatients in Al-Madina Al-Monwara, Saudi Arabia, has not before been the subject of a comprehensive investigation. Additionally, the prevalence of PE among various types of cancer has not been previously discussed in this patient cohort. The results of the present study during a 4-year period were in agreement with the study of Reynolds et al. (2008) [15], which reported that PE incidence among patients who had cancer was ranging from 0.13 to 8.65% generally. The current study estimated a PE incidence of 4.4% in a total of 540 patients who had various cancer types.
In the study, PE risk was higher in cancers of the larynx, pancreas, bladder, and genitourinary system, particularly lung adenocarcinoma, prostate cancer, and uterine cancers, while it was relatively less common in breast cancer. This finding is consistent with earlier studies that found a higher incidence of PE in pancreatic, lung, renal, uterine, and pancreatic cancers [16]. It was declared that aging of the patients, cancer stage, and immobility are some potential causes of an increased risk of PE [17]. According to Chew et al. (2006) [18], breast cancer patients had a decreased incidence of PE. A recent study showed that lung cancer patients now had a 20-fold higher chance of developing PE than the general population, particularly those with the adenocarcinoma histological type [10].
In this study, the majority of PE (20/24, 84%) emerged within the first 6 months of a cancer diagnosis and in severe stages, while only 16% (4/24) of PE developed throughout the first 2 to 3 years of the patient follow-up. This finding is in concordance with the results of Biedka et al. (2012) [6].
In the first 6 months following the diagnosis of malignancy, PE may develop for a variety of reasons, including the impact of an active cancer and treatment (chemo, radiation, and hormone therapy), which results in the downregulation of anticoagulants and the overexpression of procoagulant proteins [3]. Other mechanisms at play include endothelial damage, endothelial cells activation to release procoagulant substances, inflammation that occurred due to necrosis or acute-phase reactants secretion, and other factors including surgery and immobilization [19] 20.
Regardless of the type of cancer, low-risk PE was the most prevalent degree in cancer patients with 75% (18/24) of patients while central PE only made up 25% (6/24) of PE. These results are different from Karippot et al.’s (2012) study [2] which reported that central pulmonary embolism was developed at a higher rate among cancer patients. This might be brought on by variations in the whole patient number and the presence of patients who had various malignancies.
The present study found that the incidental PE incidence was 1.3%, which differs from the findings of several earlier studies that found the incidental PE incidence to be 4.3%. The variability of the population of the patient under study and characteristics of the tumors, such as the stage of disease, may be the causes of these disparities [21].
Since incidental PE is common in malignancies of the pancreas, lungs, and uterus and 100% of PE identified in chest MDCT throughout the staging of cancer, patients should have nearby follow-up and exploration for any PE in chest MDCT in the course of staging and follow up [22].
It was detected that dyspnea was a higher percentage of symptoms among cancer patients with PE which is in agreement with different studies in oncogenic patients as regards dyspnea [23] 24. In a study by Chlapoutakis et al. (2022) [23], chest pain was detected as a lower clinical presentation (39.4%) than in the present study. This can be explained by the fact that, in our study, patients with breast cancer were higher than other malignancies and more likely to have dyspnea and chest pain, which are warning signs of malignancy for the examination of PE.
Conclusion
While PE is less frequent among patients who had breast cancer, it is common among patients who had cancers of the pancreas, lungs, throat, uterus, and prostate. Chest discomfort and dyspnea are warning indicators for PE in malignancy, and the initial 6 months following the discovery of cancer are the most risky period for developing PE. The most frequent type of PE in cancer patients was low-risk PE. A considerable high risk of incidental PE exists in those who had cancer in the lung, pancreas, uterus, or bladder. Therefore, it is advised that the cancer patients should receive rigorous monitoring during the first 6 months to detect pulmonary embolism.
Availability of data and materials
The patient’s data are presented on a computerized patient file at the King Fahd Hospital Recording Department, Al-Madina Al-Monoura, KSA. www//KFHM-moh.gov.sa.
Abbreviations
- CTA:
-
Computed tomography pulmonary angiography
- ESC:
-
European Society of Cardiology
- ICD:
-
International Classification of Disease
- IVC:
-
Inferior vena cava
- KSA:
-
Kingdom of Saudi Arabia
- MDCT:
-
Multi-detector computed tomography
- PE:
-
Pulmonary embolism
- TPA:
-
Tissue plasminogen activator
- VTE:
-
Venous thromboembolism
References
Fujieda K, Nozue A, Watanabe A, Shi K, Itagak H, Hosokawa Y, Nishida K, Tasaka N, Satoh T, Nishide K (2021) Malignant tumor is the greatest risk factor for pulmonary embolism in hospitalized patients: a single-center study. Thrombosis J 19(77):2–7
Karippot A, Shaaban HS, Maroules M, Guron G (2012) The clinical characteristics of pulmonary embolism in patients with malignancy: a single medical institutional experience. N Am J Med Sci [Internet]. 4(11): 600–604 Available from: https://doi.org/10.4103/1947-2714.103333
Griffiths GO, Burns S, Noble SI, Macbeth FR, Cohen D, Maughan TS (2009) FRAGMATIC: a randomised phase III clinical trial investigating the effect of fragmin added to standard therapy in patients with lung cancer. BMC Cancer [Internet]. 9(1):355. Available from: https://doi.org/10.1186/1471-2407-9-355
Abdol Razak NB, Jones G, Bhandari M, Berndt MC, Metharom P (2018) Cancer-associated thrombosis: an overview of mechanisms, risk factors, and treatment. Cancers (Basel) 10:380
Blom JW, Doggen CJM, Osanto S, Rosendaal FR (2005) Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA [Internet]. 293(6):715–22. Available from: https://doi.org/10.1001/jama.293.6.715
Biedka M, Ziółkowska E, Windorbska W (2012) Acute pulmonary embolus in the course of cancer. Contemp Oncol (Pozn) [Internet]. 16(5):388–93. Available from: https://doi.org/10.5114/wo.2012.31766
Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olson RE (2006) Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med [Internet]. 119(1):60–8. Available from: https://doi.org/10.1016/j.amjmed.2005.06.058
Heraudeau A, Delluc A, Le Henaff M, Lacut K, Leroyer C, Desrues B, Couturaud F and Tromeur C. Risk of venous thromboembolism in association with factor V leiden in cancer patients ± The EDITH case-control study. PLoS ONE 13(5): e0194973. Available from: https://doi.org/10.1371/journal.pone.0194973
Perry JR, Julian JA, Laperriere NJ, Geerts W, Agnelli G, Rogers LR, et al (2010) PRODIGE: a randomized placebo-controlled trial of dalteparin low-molecular-weight heparin thromboprophylaxis in patients with newly diagnosed malignant glioma: PRODIGE: a randomized placebo-controlled trial of dalteparin. J Thromb Haemost [Internet]. 8(9):1959–65. Available from: https://doi.org/10.1111/j.1538-7836.2010.03973.x
Blom JW, Osanto S, Rosendaal FR (2006) High risk of venous thrombosis in patients with pancreatic cancer: a cohort study of 202 patients. Eur J Cancer [Internet]. 42(3):410–4. Available from: https://doi.org/10.1016/j.ejca.2005.09.013
Farrell C, Jones M, Girvin F, Ritchie G, Murchison JT (2010) Unsuspected pulmonary embolism identified using multidetector computed tomography in hospital outpatients. Clin Radiol [Internet]. 65(1):1–5. Available from: https://doi.org/10.1016/j.crad.2009.09.003
Ghaye B, Ghuysen A, Bruyere P-J, D’Orio V, Dondelinger RF (2006) Can CT pulmonary angiography allow assessment of severity and prognosis in patients presenting with pulmonary embolism? What the radiologist needs to know. Radiographics [Internet]. 26(1):23–39; discussion 39–40. Available from: https://doi.org/10.1148/rg.261055062
Desai SR (2007) Unsuspected pulmonary embolism on CT scanning: yet another headache for clinicians? Thorax [Internet]. 62(6):470–2. Available from: https://doi.org/10.1136/thx.2006.067884
Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing G-J, Harjola V-P, et al (2019) ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J [Internet]. 54(3):1901647. Available from: https://doi.org/10.1183/13993003.01647-2019
Reynolds MW, Shibata A, Zhao S, Jones N, Fahrbach K, Goodnough LT (2008) Impact of clinical trial design and execution-related factors on incidence of thromboembolic events in cancer patients: a systematic review and meta-analysis. Curr Med Res Opin [Internet]. 24(2):497–505. Available from: https://doi.org/10.1185/030079908x261050
Khorana AA, Connolly GC (2009) Assessing risk of venous thromboembolism in the patient with cancer. J Clin Oncol [Internet]. 27(29):4839–47. Available from: https://doi.org/10.1200/JCO.2009.22.3271
Agnelli G, Bolis G, Capussotti L, Scarpa RM, Tonelli F, Bonizzoni E, et al (2006) A clinical outcome-based prospective study on venous thromboembolism after cancer surgery: the @RISTOS project. Ann Surg [Internet]. 243(1):89–95. Available from: https://doi.org/10.1097/01.sla.0000193959.44677.48
Chew HK, Wun T, Harvey D, Zhou H, White RH (2006) Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med [Internet]. 166(4):458–64. Available from: https://doi.org/10.1001/archinte.166.4.458
Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH (2007) Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer [Internet]. 110(10):2339–46. Available from: https://doi.org/10.1002/cncr.23062
Sørensen HT, Mellemkjaer L, Olsen JH, Baron JA (2000) Prognosis of cancers associated with venous thromboembolism. N Engl J Med [Internet]. 343(25):1846–50. Available from: https://doi.org/10.1056/NEJM200012213432504
Abdel-Razeq H, Mansour A, Ismael Y (2011) Incidental pulmonary embolism in cancer patients: clinical characteristics and outcome – a comprehensive cancer center experience. Vasc Health Risk Manag [Internet]. 7:153–8. Available from: https://doi.org/10.2147/vhrm.s17947
Dentali F, Ageno W, Becattini C, Galli L, Gianni M, Riva N, et al (2010) Prevalence and clinical history of incidental, asymptomatic pulmonary embolism: a meta-analysis. Thromb Res [Internet]. 125(6):518–22. Available from: https://doi.org/10.1016/j.thromres.2010.03.016
Chlapoutakis S, Georgakopoulou VE, Trakas N, Kouvelos G, Papalexis P, Damaskos C, et al (2022) Characteristics and outcomes of cancer patients who develop pulmonary embolism: A cross-sectional study. Oncol Lett [Internet]. 23(5):168. Available from: https://doi.org/10.3892/ol.2022.13288
Pollack CV, Schreiber D, Goldhaber SZ, Slattery D, Fanikos J, O’Neil BJ, et al (2011) Clinical characteristics, management, and outcomes of patients diagnosed with acute pulmonary embolism in the emergency department: initial report of EMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry). J Am Coll Cardiol [Internet]. 57(6):700–6. Available from: https://doi.org/10.1016/j.jacc.2010.05.071
Acknowledgements
Thanks to all participating patients, medical record staff, and radiology unit staff.
Funding
It supplied from up to date, WHO, Google search.
Author information
Authors and Affiliations
Contributions
The authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The current study was permitted by ethics approval and consent to engage King Fahd Hospital- Al-Madina Al-Monoura, KSA, with number (66) in March 2019.
Consent for publication
There was taken written consent from the participants and they were available if wanted.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Samra, S.R., Said, A.M., Elsayed, D.H. et al. The incidence and clinical characteristics of pulmonary embolism in oncologic patients. Egypt J Bronchol 16, 64 (2022). https://doi.org/10.1186/s43168-022-00167-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-022-00167-1