
Abstract
Background
Ciliated Muconodular Papillary Tumor (CMPT) was first reported in 2002, and fewer than 100 cases have since been reported. The prognosis after surgical resection is good, and recurrence has not been reported. However, it is easily misdiagnosed as adenocarcinoma. Summarizing the CT features of CMPT will help doctors better understand the disease.
Case presentation
Here, we report a rare and interesting case of ciliated muconodular papillary tumor. A 6-mm diameter solid nodule with slight lobulation, short spines, and subpleural indentation. Patients with clinical diagnosis of high-risk subpleural nodule in the left lung underwent thoracoscopic surgery. Most CMPT cases lack specific clinical manifestations and were found incidentally on physical examination or during a workup for other diseases. The disease was diagnosed through CT and biopsy, and it responded well to surgery.
Conclusions
This paper presents the detailed computed tomography features of CMPT to help prevent misdiagnosis. The typical manifestations of CMPT imaging as solid and partial nodules, nodules in subpleural or peripheral zones, and nodules contain cavities.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
A ciliated muconodular papillary tumor (CMPT) is a rare benign tumor, with fewer than 100 cases reported in the literature. No specific clinical symptoms have been identified, and it is often diagnosed incidentally. This paper emphasizes the cytological and computed tomography (CT) features of CMPT via a case study and literature review.
In 2002, Ishikawa et al. first described a rare pulmonary nodule composed of ciliated columnar cells, mucous cells, and basal cells [1]. This disease was named CMPT. Only a few surgically confirmed cases have been reported worldwide, and more cases have been reported in East Asia than in the USA or Europe [2]. It is easily confused with adenocarcinoma and mucoepidermoid carcinoma due to the lack of typical clinical manifestations, imaging features, and pathological features. Consequently, it is easily misdiagnosed as lung cancer and thus overtreated. In this paper, by reviewing the CT images of cases in the literature, the imaging manifestations were summarized, so as to improve the clinical and imaging doctors’ understanding of the disease, reduce misdiagnosis, improve the rate of early diagnosis and early treatment, and reduce complications.
Case presentation
The patient was a 64-year-old woman with no history of smoking. She initially had persistent attacks of dull epigastric pain that became worse after eating. There is not any relevant past medical or family history. On hospitalization, there were no fevers, chills, cough, sputum, chest tightness, palpitations, or shortness of breath. Physical examination showed no chest deformity or sternal tenderness, normal thoracic breathing rhythm, chest symmetry, symmetric chest wall movement, and normal vocal fremitus. The lungs were hyper-resonant on percussion and while breathing. No moist rales or pleural rubs were heard.
Laboratory tests revealed elevated levels of carcinoembryonic antigen (CEA) and thyroid-stimulating hormone, no carbohydrate antigens, and an alpha-fetoprotein (AFP) level of 8.18 ng/ml (0–7 ng/ml).
On May 9, 2018, CT showed a 5-mm diameter solid subpleural nodule with a smooth margin in the outer posterior basal segment of the left lower lobe (Fig. 1). The doctor recommends that the patient have an annual review. CT on June 11, 2020, revealed a 6-mm diameter solid nodule with slight lobulation, short spines, and subpleural indentation (Fig. 2).

CT showed a round, 5-mm diameter solid, subpleural nodule. There were no spikes, lobulation, or pleural indentation

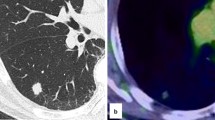
A CT showed a round part solid subpleural nodule 6 mm in diameter, Lobulation, spikes, pleural indentation; three-dimensional reconstruction; and three-dimensional pulmonary reconstruction. B and C show the tumor under the pleura, with pleural indentation and thickening
Diagnosis and treatment (Table 1)
The high-risk subpleural nodule in the left lung was found enlarged on CT review two years later. The nodule has the characteristic: slightly nodule lobules, spikes, and pleural indentation. Thus, the patient underwent thoracoscopic surgery six days later. The incision was made in the fifth intercostal space in the left anterior axillary line. No pleural effusion or adhesions were found, and the lung was well differentiated. Local protuberant nodules were seen at the posterolateral basal segment of the left lower lobe. The surrounding area was slightly red and swollen, but no nodules were found on the parietal pleura or diaphragm. A cut was made along the base of the tumor, and a frozen section suggested a micro-invasive adenocarcinoma with acinar cells; the nodule was approximately 6 mm in diameter.
A wedge-shaped slice of tissue was removed for pathological examination. The tissue contained a 4-mm diameter gray-white nodule with a clear margin and no envelop. Microscopically, glandular tubular and papillary structures were seen. The glandular cavity and papilla were covered with two layers of the epithelium. The inner layer contained basal cells and the outer layer mostly ciliated cells. A few cells were mucinous, and mucinous secretions could be seen in the glandular cavity. The cells were regular in shape and size, and no mitosis or necrosis was observed. The tumor was not connected to the bronchus. There was an area of perivascular cell proliferation in the tumor (Fig. 3).

A Hematoxylin and eosin staining (H&E) of loupe image. A Tumor cells are proliferating along the alveolar walls, surrounded by mucous lakes, B Tumor cells are proliferating along the alveolar walls, consisting of ciliated columnar cells and goblet cells with basaloid
Immunohistochemistry showed positivity for TTF-1 (clone SPT24) in epithelial and basal cells, partial positivity for napsin A in epithelia, positivity for CK7 in epithelia, positivity for P40 in the basal layer, positivity for P63, positivity for CK5/6, negativity for Syn, negativity for CgA, negativity for CD56, 1% positivity for Ki67, partial positivity for CEA, and negativity for CK20(Fig. 4).

A Ciliated cells, mucous cells, and basal cells positive for CK7 (EnVision, ×100). B TTF-1 is weak to moderately positive in the basal cells but negative in the luminal cells. C Cells lining the cavity are positive for CEA (EnVision, ×100)
Follow-up and outcomes
Pathologically, distal-type CMPT was diagnosed. There has been no disease recurrence, and no treatment such as chemotherapy or radiotherapy was required. On February 19, 2021, CT scan showed no recurrence.
Discussion
In this study, an extensive literature search of PubMed and Web of Sciences was conducted on 20 August 2020 to include all published studies. A total of 18 CMPT articles were published and 87 cases, 35 cases of which contained CT images. There were 36 CT images, including that from our case. The reported images were evaluated by two senior radiologists for the respiratory system. CT findings were summarized in Table 2. The 36 images showed 18 solid nodules (50.0%), 11 partially solid nodules (30.5%), three GGNs (8.3%), two inflammatory solid lesions (5.56%), and two hollow lesions (5.56%). Subdividing the lungs into the inner, middle, and outer parts, there were 22 subpleural nodules (61.1%), 13 peripheral lesions (36.1%), and 2 central lesions (5.6%). Of the lesions, 15 showed air bronchograms (41.6%), 20 showed spikes (55.6%), 19 showed lobulation (52.8%), 15 showed pleural indentation (41.6%), 11 were subpleural nodules with cavities (30.6%), and 4 in the lung periphery had cavities (11.1%). Imaging manifestations of typical CMPT nodules are as follows: elderly people, solid or partially solid nodules, located under the pleura or peripheral zone, the nodules contain cavities, and pleural depression, air bronchograms, spikes.
In this study, all of the articles containing CT images had pathology. In a literature search, we found 87 cases in 18 articles in addition to our case (a total of 88 cases). The average age of the patients was 64.8 (range 31 to 82) years. The ratio of males to females was 42:46. The ratio of lesions in the left lung to those in the right lung was 30:36 (in 21 cases, the affected lung was not reported). There was a history of smoking in 21 of 64 (32.8%) patients, and the smoking history was not known in 24 patients. Table 3 shows the average tumor diameter 6.91 mm.
We found articles related to the CT findings of CMPT in 18 publications from 2002 to 2020 [3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20], but none provided a detailed description of the CT findings. Most CMPT cases lack specific clinical manifestations and are found incidentally on physical examination or during a workup for other diseases. A summary of the CT manifestations of CMPT would give doctors a better understanding of this disease, thereby reducing misdiagnosis, missed diagnosis, and especially overtreatment. Qiang Zheng summarized the CT imaging features of CMPT for 11 typical pathological and 10 atypical pathological cases [20]. CMPT are more likely to develop in the elderly and females, The lesion diameter averaged 7 (range 4–20) mm. Small pseudocavitation was found in 64% of the typical cases but only 10% of the atypical cases, In this paper, the ratio of male to female is 1:1. This article summarizes typical CMPT image characteristics based on CMPT image performance. Onishi et al. summarized the CT imaging features of 16 lesions, of which 9 were in the right lung and 7 in the left lung. Ten lesions were subpleural, while six were 3–18 mm from the pleura. One case had ground-glass nodules (GGNs), seven had partial GGNs, and nine had solid nodules; the average diameter was 9.1±2.4 mm [13]. The sex of these patients was unknown, our study further summarizes the nodules lobules, pleural indentation, spikes, and air bronchograms, summarizes the most characteristic imaging manifestations of subpleural nodules with cavities.
The imaging findings of CMPT have been differentiated from those of adenocarcinoma [21]. Compared with adenocarcinomas, CMPT are usually found in older patients, are smaller, and contain pseudocavitation in the nodules. In a study that classified the nodules as central or peripheral [21], the nodules were peripheral in 36 cases (97.2%) and were round or oval in most cases (see Table 4).
On gross pathology, the nodules are usually pale or grayish brown, soft, and well-recognized, with a mucinous or gelatinous substance [17]. The tumors are composed of ciliated columnar cells, mucous cells, and basal cells. The ciliated columnar cells are on the surface of adenoids and papilla-like structures. The basal cells act as a scaffold in the outer layer, whereas the mucous cells are scattered. Microscopically, there was no obvious atypia, mitotic figures (mitosis), or necrosis of the tumor cells. A large amount of mucus was found in the alveolar space or around the tumor. Some of the tumor epithelium grew discontinuously along the alveolar wall, and there was no surrounding envelop. Irregular bronchial walls or thick-walled vessels were found in most cases [22]. The diagnosis of CMPT is based primarily on morphology; cilia, mucus, and papilla are often seen in this disease, although all three components may not be present in some cases. The latter cases are known as atypical CMPT, which needs to be validated by more studies.
Immunohistochemically, CEA and CK7 were highly positive in the three cell types of CMPT, whereas TTF-1 was weakly positive, and Ki-67 expression was low (≤10%). CK20 and MUC2 expression was negative. p40, p63, and CK5/6 were highly positive in basal cells. MUC5AC was not expressed in mucous cells but was expressed in some ciliated cells [23].
Many gene mutations are detected in CMPT. Among 18 cases, BRAF-V600E mutations were detected in six cases, EGFR exon 19 deletions in three cases, KT1-E17K mutations in two cases, and BRAF-G606R and KRAS-G12D mutations in one case each. Given the few cases reported and lack of research on gene mutations in CMPT, cancer driver genes have yet to be identified. Although Udo E and Kamata T thought CMTP was an inflammatory lesion, they did not use anti-inflammatory treatment before surgery, which was consistent with our study [24, 25].
Initially, CMPT were thought to be malignant [7], but with increasing knowledge, these tumors now tend to be classified as benign. No recurrence has been reported in any case undergoing surgical resection after long-term follow-up. Cilia were found in all cases, while only a few malignant tumors have cilia. There was an absence of atypia, mitotic figures, and necrosis and a presence of low Ki-67 expression, and high BRAF expression; the opposite features indicate malign lesions [25]. More importantly, no ciliated or goblet cells were seen in these tumors. The differential diagnosis based on pathological findings includes squamous metaplasia, intrabronchial papilloma, mucoepidermoid carcinoma, and well-differentiated adenocarcinoma. Well-differentiated papillary adenocarcinoma has been reported [26], and its pathology is similar to that of CMPT, except that the cells are heterogeneous.
In summary, CMPT has the characteristic of typical pulmonary nodules, the nodules lobules, pleural indentation, spikes, and air bronchograms, comprise the most characteristic imaging manifestations of subpleural nodules with cavities. Regular review can be performed. When nodules become enlarged, surgical treatment should be performed. The diagnosis of CMPT is based primarily on morphology; cilia, mucus, and papilla are often seen in this disease, The atypical CMPT is missing one of these components, CMPT is easily misdiagnosed to lung adenocarcinoma on CT, The former nodule is small (with an average diameter of 6 mm), while the latter is 24mm. The former is mostly located in the peripheral zone, about 97.2%, while the latter is located in the middle and inner zone, 34.8%. Moreover, lung adenocarcinoma has vessel convergence, air bronchiologram (irregularity, disruption, or dilatation) (Table 4).
Conclusion
Few cases of CMPT have been reported, and this disease has no specific clinical manifestations. The CT imaging features, pathological and immunohistochemical features, and possible gene mutations in the disease were discussed. This paper should give radiologists, thoracic surgeons, and pathologists a better understanding of CMPT to help them avoid misdiagnosis.
Availability of data and materials
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CMPT:
-
Ciliated muconodular papillary tumor
- CT:
-
Computed tomography
- CEA:
-
Carcinoembryonic antigen
- AFP:
-
Alpha-fetoprotein
References
Ishikawa Y (2002) Ciliated muconodular papillary tumor of the peripheral lung: benign or malignant? Pathol Clin Med (Byouri-to-Rinsho) 20:964–965. https://doi.org/10.1016/j.rmedc.2008.04.005
Liu L, Aesif SW, Kipp BR, Voss JS, Daniel S, Aubry MC et al (2016) Ciliated muconodular papillary tumors of the lung can occur in western patients and show mutations in BRAF and AKT1. Am J Surg Pathol 40(12):1631–1636. https://doi.org/10.1097/PAS.0000000000000707
Miyai K, Takeo H, Nakayama T, Obara K, Aida S, Sato K, Matsukuma S (2018) Invasive form of ciliated muconodular papillary tumor of the lung: a case report and review of the literature. Pathol Int 68(9):530–535. https://doi.org/10.1111/pin.12708
Tachibana M, Saito M, Kobayashi J, Isono T, Yatabe Y, Tsutsumi Y (2019) Distal-type bronchiolar adenoma of the lung expressing p16INK4a – morphologic, immunohistochemical, ultrastructural and genomic analysis – report of a case and review of the literature. https://doi.org/10.1111/pin.12904
Abe M, Osoegawa A, Miyawaki M, Noda D, Karashima T, Takumi Y, Hashimoto T, Okamoto T, Daa T, Sugio K (2019) Ciliated muconodular papillary tumor of the lung: a case report and literature review. https://doi.org/10.1007/s11748-019-01252-x
Cheung FMF, Guan J, Luo QG, Sihoe ADL, Shen XP (2019) Ciliated muconodular papillary tumour of the lung mimicking mucinous adenocarcinoma: a case report and literature review. Hong Kong Med J 25(1):71–73. https://doi.org/10.12809/hkmj165032
Harada T, Akiyama Y, Ogasawara H, Kishi F, Hattori A, Okamoto K et al (2008) Ciliated muconodular papillary tumor of the peripheral lung: a newly defined rare tumor. Respir Med CME 1(2):176–178. https://doi.org/10.1016/j.rmedc.2008.04.005
Hata Y, Yuasa R, Sato F, Otsuka H, Goto H, Isobe K et al (2013) Ciliated muconodular papillary tumor of the lung: a newly defined low-grade malignant tumor with CT findings reminiscent of adenocarcinoma. Jpn J Clin Oncol 43(2):205–207. https://doi.org/10.1093/jjco/hys218
Ishikawa M, Sumitomo S, Imamura N, Nishida T, Mineura K, Ono K (2016) Ciliated muconodular papillary tumor of the lung: report of five cases. J Surg Case Rep 2016(8). https://doi.org/10.1093/jscr/rjw144
Jin Y, Shen X, Shen L, Sun Y, Chen H, Li Y (2017) Ciliated muconodular papillary tumor of the lung harboringALKgene rearrangement: case report and review of the literature. Pathol Int 67(3):171–175. https://doi.org/10.1111/pin.12512
Kon T, Baba Y, Fukai I, Watanabe G, Uchiyama T, Murata T (2016) Ciliated muconodular papillary tumor of the lung: a report of five cases. Pathol Int 66(11):633–639. https://doi.org/10.1111/pin.12460
Mikubo M, Maruyama R, Kakinuma H, Yoshida T, Satoh Y (2019) Ciliated muconodular papillary tumors of the lung: cytologic features and diagnostic pitfalls in intraoperative examinations. Diagn Cytopathol 47(7):716–719. https://doi.org/10.1002/dc.24169
Onishi Y, Kusumoto M, Motoi N, Watanabe H, Watanabe S-i (2020) Ciliated muconodular papillary tumor of the lung: thin-section CT findings of 16 cases. Am J Roentgenol 214(4):761–765. https://doi.org/10.2214/ajr.19.21945
Onishi Y, Ito K, Motoi N, Morita T, Watanabe S, Kusumoto M (2020) Ciliated muconodular papillary tumor of the lung: 18F-FDG PET/CT findings of 15 cases. https://doi.org/10.1007/s12149-020-01457-8
Sato S, Koike T, Homma K, Yokoyama A (2010) Ciliated muconodular papillary tumour of the lung: a newly defined low-grade malignant tumour. Interact Cardiovasc Thorac Surg 11(5):685–687. https://doi.org/10.1510/icvts.2009.229989
Shao K, Wang Y, Xue Q, Mu J, Gao Y, Wang Y et al (2019) Clinicopathological features and prognosis of ciliated muconodular papillary tumor. J Cardiothorac Surg 14(1). https://doi.org/10.1186/s13019-019-0962-3
Kamata T, Yoshida A, Kosuge T, Watanabe S-i, Asamura H, Tsuta K (2015) Ciliated muconodular papillary tumors of the lung: a clinicopathologic analysis of 10 cases. Wolters Kluwer Health 39(6):753–760
Uchida T, Matsubara H, Ohnuki Y, Sugimura A, Matsuoka H, Ichihara T, Nakajima H (2019) Ciliated muconodular papillary tumor of the lung presenting with polymyalgia rheumatica-like symptoms: a case report. https://doi.org/10.21037/acr.2019.09.06
Yao X, Gong Y, Zhou J, Lyu M, Zhang H, Zhou H, Luo Q, Liu L (2019) A surgical case of ciliated muconodular papillary tumor. https://doi.org/10.1111/1759-7714.12997
Zheng Q, Luo R, Jin Y, Shen X, Shan L, Shen L et al (2018) So-called “non-classic” ciliated muconodular papillary tumors: a comprehensive comparison of the clinicopathological and molecular features with classic ciliated muconodular papillary tumors. Hum Pathol 82:193–201. https://doi.org/10.1016/j.humpath.2018.07.029
Kim SK, Kim TJ, Chung MJ, Kim TS, Lee KS, Zo JI et al (2018) Lung adenocarcinoma: CT features associated with spread through air spaces. Radiology 289(3):831–840. https://doi.org/10.1148/radiol.2018180431
Chuang HW, Liao JB, Chang HC, Wang JS, Lin SL, Hsieh PP (2014) Ciliated muconodular papillary tumor of the lung: a newly defined peripheral pulmonary tumor with conspicuous mucin pool mimicking colloid adenocarcinoma: a case report and review of literature. Pathol Int 64(7):352–357. https://doi.org/10.1111/pin.12179
Kamata T, Yoshida A, Kosuge T, Watanabe S, Asamura H, Tsuta K (2015) Ciliated muconodular papillary tumors of the lung: a clinicopathologic analysis of 10 cases. Am J Surg Pathol 39(6):753–760. https://doi.org/10.1097/PAS.0000000000000414
Udo E, Furusato B, Sakai K, Prentice LM, Tanaka T, Kitamura Y et al (2017) Ciliated muconodular papillary tumors of the lung with KRAS/BRAF/AKT1 mutation. Diagn Pathol 12(1):62. https://doi.org/10.1186/s13000-017-0651-2
Kamata T, Sunami K, Yoshida A, Shiraishi K, Furuta K, Shimada Y et al (2016) Frequent BRAF or EGFR mutations in ciliated muconodular papillary tumors of the lung. J Thorac Oncol 11(2):261–265. https://doi.org/10.1016/j.jtho.2015.10.021
Imai T, Suga M, Kaimori M, Hiyama M, Yokoyama K, Kurotaki H (2010) Peripheral pulmonary papillary adenocarcinoma with prominent cilia: report of a rare case that was difficult to diagnose preoperatively. Acta Cytol 54(5 Suppl):949–957
Acknowledgements
Grateful acknowledgement is made to Dr. Ben Bishop and Dr. Mary Macalalad who gave me considerable help by means of suggestion.
Patient perspective
The patient shared ideas to decrease their burden of treatment and was very satisfied with the treatment.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
HL L and XMQ contributed equally to the present study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from the patient for the publication of this report and any accompanying images.
Consent for publication
Written informed consent for publication was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, H., Huang, P., Zhang, M. et al. Ciliated muconodular papillary tumor of the lung: a case report and literature review. Egypt J Bronchol 16, 20 (2022). https://doi.org/10.1186/s43168-021-00094-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-021-00094-7