
Abstract
Background
Tuberculosis in Egypt is a main public health problem. Egypt is categorized among the mid-level incidence countries. The objective of this work is to study the epidemiology of TB in Giza Governorate during the period from 2014 to 2018.
Results
This study revealed that the total number of TB cases in Giza Governorate during the period from 2014 to 2018 was 3357 (2035 males and 1322 females including 199 children) with the highest number of cases in 2017 (n=770 cases). The highest incidence occurred in the age group 18–65 years (86.3%%, 78.8%, 83.8%, 84.2%, and 87.1%) and male gender (56.8%, 62.8%, 59.9%, 61.3%, and 61.5%) during the study period, respectively, and in urban residence, the higher percentage occurred in PTB than EPTB in 2014, 2015, 2016, and 2018 (66.2%, 58.9%, 57.3%, and 55.5%), respectively, while the incidence of the extra PTB was higher than PTB in 2017 (51.6% versus 48.4%). The increased incidence of new cases (92.9%, 89.6%, 92.7%, 91.8%, and 92.9%) during the 5 studied years are smear-positive and cure outcome (86.3%, 87.7%, 88.7%, 83.4%, and 83.4%, respectively)
Conclusion
Young, middle-aged male, and new smear-positive cases were highest in percentage. The highest percentage of PTB (66.2%) was registered in 2014, and the highest percentage of EPTB (51.6%) was registered in 2017. The increased percentage of cure outcome was during the period from 2014 to 2018 in Giza Governorate.
Similar content being viewed by others

Background
Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium tuberculosis. The disease typically affects the lungs (pulmonary TB) but can affect other parts of the body as well as extrapulmonary TB [1].
TB represents the second leading cause of death from an infectious disease worldwide after HIV infection [2].
The prevalence rate of TB in Egypt was 26 per 100,000 people according to the World Health Organization estimate in 2014, while the incidence rate was 15 per 100,000 people. Screening, diagnosis, notification, and registration of TB cases were implemented all over Egypt according to the National TB Strategy of the National Tuberculosis Control Program (NTB) [3].
Egypt has massively engaged in early case detection, provision of adequate chemotherapy, and prevention of transmission to new cases [3].
So the objective of this work was to study the epidemiology of TB in Giza Governorate during the period from 2014 to 2018.
Methods
This was a retrospective study involving a record review of notified, registered, and treated TB patients in the chest hospital and clinics in Giza Governorate during the period from 2014 to 2018.
It includes Imbaba, Om El Almasreen, Oseem, El Ayat, Elbadrasheen, El Saff, and Atfeeh. All data were collected from the chest hospitals (two hospitals) and chest dispensaries (5 dispensaries) in El-Giza Governorate.
We analyzed TB cases reported from January 2014 to December 2018. The diagnosis of TB in Giza Governorate is made in line with the National Egyptian TB Control Program Guidelines of the Ministry of Health
Collection and analysis of data
-
Sociodemographic data.
-
Patient classification group: new, relapse, treatment after failure, default or cured.
-
Forms of tuberculosis; either pulmonary (smear-positive or smear-negative) or extrapulmonary (and its site as LN, intestine, meninges, breast, renal).
-
Method of diagnosis: bacteriological, e.g., smear analysis, gene Xpert or culture, radiological, pathological, and radio pathological.
-
Schedule of treatment (recommended treatment regimen according to NTP).
-
The recorded follow-up for smear-positive pulmonary tuberculosis.
-
Outcome: cure, treatment completion, treatment failure, death, or default.
Ethics approval
The ethics approval to use, report, and publish the collected data was obtained from the Ministry of Health, Egypt. Patient information was anonymized and de-identified prior to the analysis. Also, this study was approved by the Institutional Review Board of the Faculty of Medicine for Girls (the committee’s reference number IRB 201910179), Al-Azhar University/Cairo branch on October 1, 2019, and was obliged to the standards of the Declaration of Helsinki.
Statistical analysis
Data were collected into a paper form by authors. Data were fed to the computer as an Excel sheet (Microsoft Corporation, Redmond, WA, USA) and were validated and analyzed by SPSS program version 15 (SPSS Inc., Chicago, IL, USA). A descriptive analysis was done. Comparisons were done among variables using the chi-squared test. A chi-squared test was used to evaluate the differences in proportions. Comparisons at p < .05 were considered significant.
Results
Table 1 showed that during the 5 years of study, the highest incidence occurred in the age group 18–65 years (86.3%%, 78.8%, 83.8%, 84.2%, and 87.1%, respectively) and the lowest incidence occurred at the extremes of age, the age group less than 1 year (0.4%, 1.3%, 0.9%, and 0.3%) except in 2015 (6.4%) and more 65 years (2.4%, 3.8%, 3.6%, 4.0%, and 4.6%) with a highly statistically significant difference p value < 0.001 between studied years as regards age categories.
Table 2 showed that no statistical significant difference (p value > 0.05) between studied years as regards sex and residence of studied patients with higher incidence occurred in both male gender (56.8%, 62.8%, 59.9%, 61.3%, and 61.5%) and urban residence (88.0%, 91.9%, 90.8%, 92.1%, and 92.0%). While there was highly statistical significant difference (p value < 0.001) between the studied years as regards TB form in the studied patients with higher percentage in PTB than in extra PTB in 2014, 2015, 2016, and 2018 (66.2%, 58.9%, 57.3%, and 55.5%, respectively) while the incidence of extra PTB was higher than of PTB in 2017 (51.6% versus 48.4%).
Table 3 demonstrated that there was a statistically significant difference (p value < 0.05) between the 5 studied years as regards patient classification group with the highest incidence of new cases (92.9%,89.6%, 92.7%, 91.8%, and92.9%, respectively) during the 5 studied years followed by the relapse and failure and the lowest incidence of resistant cases (0.6%, 1.4%, 0.4%, 0.5%, and 0.1%, respectively).
Table 4 demonstrated that there was highly statistical significant difference (p value < 0.001) between the studied years as regards the method of diagnosis in studied patients with the highest percentage of bacteriological (smear positive) (59.2%, 47.6%, 48.6%, 46.0%, and 50.6%) followed by the pathological and radiological and lowest percentage was bacteriological (smear negative) (0.6%, 0.6%, 1.0%, 0.1%, and 0.1%, respectively).
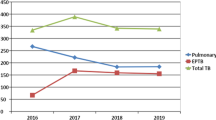
Figure 1 showed that there was a highly statistically significant difference (p value < 0.001) between the studied years as regards treatment outcome in studied patients with the highest percentage of cured cases outcome (86.3%, 87.7%, 88.7%, 83.4%, and 83.4%, respectively).

Distribution of cases according to the treatment outcome during the period of the study
Discussion
TB in Egypt is considered an important community health problem. Delay in the detection of pulmonary and laryngeal cases increases the chances of transmission [4].
There has been a major decline in the TB death rate in the last two decades, but the progress needs to be faster to fulfill the post-2015 WHO TB strategy to end the TB epidemic by 2035; with the global targets of a 95% decrease in the number of TB mortalities and a 90% reduction in TB cases [5].
Thus, the aim of this work was to study the epidemiology of TB in chest hospitals and clinics in Giza Governorate during the period from 2014 to 2018.
Our study revealed that the total number of TB cases was 3357 (2035 males and 1322 females including 199 children) with the highest number of cases in 2016, 2017, and 2018 with a peak in 2017 (n=770 cases). The higher incidence of TB occurred in males than in females in the five studied years (Table 2) which was in concordance with most individual governorate studies [3, 6,7,8,9,10]. This variance may be due to less awareness in females as many female patients do not ask for medical advice because of factors such as illiteracy and the traditions predominant in the society, which may prohibit them from going out and seeking medical advice. TB stigma is felt more strongly in females [11]. Moreover, the awareness in men is higher, indicating the differences in exposure to more outdoor activities and contact. Transfer from infection to disease owing to sex differences was related to other risk factors for TB such as cigarette and shisha smoking [12].
These findings were in disagreement with that of Mohamed et al. [1] who studied TB in patients admitted to the Assiut Chest Hospital from 2005 to 2009, where it was 70.87% for females and 29.13% for males. They attributed the higher prevalence of TB in women to men in their study due to different conditions in Upper Egypt, where females especially farmers have a chief role of work outside or inside the home, with a greater chance of exposure to infection.
This study reported that the higher incidence of TB occurred in the age group 18–65 years may be due to a high prevalence of smoking behavior in this active age group and more exposure to infection [10], and the lowest incidence occurred at the extremes of age, the age group less than 1 year (0.4%, 1.3%, 0.9%, 0.3%) except in 2015 (6.4%) and more 65 years (2.4%, 3.8%, 3.6%, 4.0%, 4.6%) (Table 2) which agreed with Mori and Leung [13] who stated that in Africa, the age group of 15–44 years comprised about 74% of the population, whereas in the USA, this age group was only 24%; therefore, in high-prevalence settings, TB affects the most productive age groups which necessitates more attention in TB control programs targeting those age groups.
This study showed that the higher incidence of TB during the 5 years study occurred in urban than rural areas (Table 2) which can be explained by the possibility of overcrowding in the urban areas, especially the slums with lack of proper aeration and increase of air pollution.
There is a difference in the distribution of TB between governorate studies where El-Behira [6], Dakahlia [14], Qalyobia, Minofia, Assiut [1], Sohag [15], and Aswan [3] showed that TB cases were more in rural areas. Those studies explained that higher TB cases in rural areas owing to poverty, drinking contaminated milk, exposure to cough spray from infected cattle, or close physical contact with infected animals. But our results were in agreement with studies in Sharkia [16] and Ismailia [13] as TB cases were higher in those studies in the urban areas.
This study reported that the higher percentage in PTB than extra PTB in 2014, 2015, 2016, and 2018. The highest percentage of PTB was in 2014 (66.2%), while the highest percentage of EPTB was in 2017 (51.6%), Table 2. Similarly, Essawy et al. (2016) [17] found that 72.8% were PTB and 27.2% were EPTB with a significant difference in the years 2009, 2007, and 2006.
This study reported that the higher percentage was in new cases than other patient classification groups with a peak in 2018 (92.9%); however, the lowest percentage is in resistant cases which can be explained by increasing awareness of cases by treatment protocol (Table 3). Also, this study reported that smear-positive diagnosed cases were the highest used method of diagnosis during the studied 5 years than other methods (Table 4) which are in concordance with Allam et al. 2019 [18] who found that Upper Egypt has higher incidence rates of new adult smear-positive cases and new extrapulmonary TB cases.
As regards the outcome in studied patients, our study revealed the highest percentage of cured cases outcome (86.3%, 87.7%, 88.7%, 83.4%, and 83.4%, respectively) in Giza Governorate during the period from 2014 to 2018 (Fig. 1).
Conclusions
The TB affects the most productive age groups, and this requires more attention in TB control programs aiming at these age groups. The highest percentage of PTB (66.2%) was registered in 2014, and the highest percentage of EPTB ((51.6%) was registered in 2017. In our study, the most common type of patients were new cases, smear-positive, and increased percentage of cure outcome during the period from 2014 to 2018 in Giza Governorate.
Limitation of the study
The unavailability of clinical data, radiologic findings, and other laboratory investigations, in particular, the culture results of patients, are the limitations of this study.
Availability of data and materials
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
Abbreviations
- TB:
-
Tuberculosis
- PTB:
-
Pulmonary tuberculosis
- EPTB:
-
Extrapulmonary tuberculosis
- NTB:
-
The National Tuberculosis Control Program
- WHO:
-
World Health Organization
- HIV:
-
Human immunodeficiency virus
References
Mohamed A, Mohamed G, Ahmed F (2010) A study of tuberculous cases admitted at Assiute Chest Hospital during period (2005–2009). South Vally University
Tadesse T, Demissie M, Berhane Y, Kebede Y, Abebe M (2011) Two-thirds of smear-positive tuberculosis cases in the community were undiagnosed in Northwest Ethiopia: population based cross-sectional study. PLoS One. 6(12):e28258. https://doi.org/10.1371/journal.pone.0028258
Sobh E, Kinawy SAE, Abdelkarim YMA, Arafa MA (2016) The pattern of tuberculosis in Aswan Chest Hospital. Egypt. Int J Mycobacteriol. 5(3):333–340. https://doi.org/10.1016/j.ijmyco.2016.08.001
Caylà JA, Orcau A (2011) Control of tuberculosis in large cities in developed countries: an organizational problem. BMC Med. 9(1):127. https://doi.org/10.1186/1741-7015-9-127
Zumla A, Chakaya J, Centis R, D’Ambrosio L, Mwaba P, Bates M et al (2015) Tuberculosis treatment and management—an update on treatment regimens, trials, new drugs, and adjunct therapies. Lancet Respir Med 3(3):220–234
Alwani AK, Al-Aarag AH, Omar MM, Hibah NA (2015) Incidence of tuberculosis before and after DOTS (direct observed therapy short course strategy) implementation in El-Behira Governorate, Egypt. Egypt J Bronchol 9(1):101–108
Khalifa HK, Al-Aarag AH, Omar M (2014) Tuberculosis situation in Gharbia Governorate (1994–2010) before and after direct observed therapy short course strategy DOTS. Benha Fac Med
Zedan M, Al Wakeel E, Shaarawy AT, Nour M (2015) Pattern of tuberculosis in patients of a university hospital during the period (2004–2011). Egypt J Chest Dis Tuberc. 64(1):85–89. https://doi.org/10.1016/j.ejcdt.2014.09.003
Shabana SMA, Omar MM (2015) Al mehy GF, Mohammad OE, Eldesouky RS. Tuberculosis situation in port said governorate (1995–2011) before and after direct observed therapy short course strategy (DOTS). Egypt J Chest Dis Tuberc. 64(2):441–447. https://doi.org/10.1016/j.ejcdt.2014.12.008
Eastwood SV, Hill PC (2004) A gender-focused qualitative study of barriers to accessing tuberculosis treatment in The Gambia, West Africa. Int J Tuberc Lung Dis. 8(1):70–75
Ambrose JA, Barua RS (2004) The pathophysiology of cigarette smoking and cardiovascular disease: an update. J Am Coll Cardiol. 43(10):1731–1737. https://doi.org/10.1016/j.jacc.2003.12.047
Mori T, Leung CC (2010) Tuberculosis in the global aging population. Infect Dis Clin North Am. 24(3):751–768. https://doi.org/10.1016/j.idc.2010.04.011
Negm MF, Al mehy GF, Ali TM, Abd Elfadil SS (2016) Tuberculosis situation in Ismailia governorate (2002–2012) before and after Direct Observed Therapy Short Course Strategy (DOTS). Egypt J Chest Dis Tuberc. 65(1):211–217. https://doi.org/10.1016/j.ejcdt.2015.09.005
Negm MF, Allam AH, ElZeheiry AH (2017) Assessment of directly observed therapy short-course (DOTs) of tuberculosis in Dakahlia governorate chest hospitals from 2006 to 2011. Egypt J Bronchol. 11(2):88–97. https://doi.org/10.4103/ejb.ejb_55_16
Mohammadien H, Alkhayat K, Hamed A, Shaaban M (2017) Patterns, trends and treatment outcomes of extra-pulmonary tuberculosis in Sohag, Upper Egypt. Egypt J Chest Dis Tuberc. 66(2):313–316. https://doi.org/10.1016/j.ejcdt.2017.02.001
Nafae RM, Elshahat HM, Said AM, Ibrahim MA (2017) Reviewing treatment outcomes of tuberculosis patients at Zagazig Chest Hospital (2008–2012). Egypt J Chest Dis Tuberc. 66(4):623–630. https://doi.org/10.1016/j.ejcdt.2017.10.006
Essawy T, Eissa S, Okab A, El Ghany E (2016) Assessment of tuberculosis situation in Cairo governorate from 2006 to 2012 after application of directly observed therapy short-course strategy. Egypt J Bronchol. 10(1):52
Allam A, Negm M, Goda T, Elawady M (2019) Tuberculosis in Upper and Lower Egypt before and after directly observed treatment short-course strategy: a multi-governorate study. Egypt J Bronchol. 13(5):722
Acknowledgements
Not applicable
Funding
Nil
Author information
Authors and Affiliations
Contributions
ARA conceived of the presented idea, recorded the data, and wrote the manuscript with the support of HHE. AEA developed the theory and performed the computations and verified the analytical methods. The authors have read and approved the final manuscript and ensure that this is the case.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval to use, report, and publish the collected data was obtained from the Ministry of Health, Egypt. Patient information was anonymized and de-identified prior to the analysis. Also, this study was approved by the Institutional Review Board of the Faculty of Medicine for Girls (the committee’s reference number IRB 201910179), Al-Azhar University/Cairo branch on October 1, 2019, and was obliged to the standards of the Declaration of Helsinki.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Malik, A.R.A., El Wahab, A.E.E.A. & Eltrawy, H.H. Retrospective study of pulmonary and extrapulmonary tuberculosis cases in Giza Governorate during the period of 2014–2018. Egypt J Bronchol 15, 24 (2021). https://doi.org/10.1186/s43168-021-00072-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-021-00072-z