
Abstract
Background
There is an evidence-practice gap in osteoarthritis (OA) management which has caused several patients living with the disease are receiving suboptimal medical care. Though there are several guidelines and treatment recommendations published, there is a real need to operationalise such evidence-based guidelines and facilitate their implementation by healthcare professionals in their local health systems
Main text
This work was carried out to outline a patient-centred multidisciplinary osteoarthritis care programme for knee and hip joint osteoarthritis that is applicable in standard clinical practice. A scoping review was conducted to identify an evidence-informed osteoarthritis management strategy, which outlines the optimal manner to treat patients living with osteoarthritis and can be implemented by healthcare professionals. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews (PRISMA-ScR) checklist was used to guide the reporting of this review. Based on this, a “Model of Care” based on a patient-centred approach with shared decision-making to enhance the timely consideration of all treatment options (including non-pharmacological, pharmacological therapies, psychotherapy, rehabilitation as well as surgery) has been developed aiming to optimise the outcomes. The goals and principles have been identified as well as the key performance indices. An algorithm for the multidisciplinary management of osteoarthritis has been developed.
Conclusion
The developed osteoarthritis care programme (OACP) provided a “Model of Care” for people living with OA which can be implemented in standard practice. The results will give insight into the features, performance, results, and outcome measures assessed. It will also guide future research towards how “Model of Care” can be patient-centred and tailored to the individual medical status.
Similar content being viewed by others

Background
Osteoarthritis (OA) is a degenerative joint disorder that most commonly affects the knees and hip joints. It is the most common form of arthritis with an estimated prevalence of 302 million people worldwide [1,2,3,4]. Bearing in mind such high prevalence, it is considered one of the major contributors to chronic pain, disability, early retirement, and lost productivity among elder adults.
Patients suffering from OA are likely to be treated with a combination of pharmaceutical and non-pharmaceutical interventions. International guidelines recommend patient education and regular exercise as first-line treatment for OA due to the effectiveness of such approach in reducing pain and disability [5,6,7,8,9,10,11]. This was endorsed by the recently published American College of Rheumatology (ACR) recommendations for OA which strongly commends self-management, weight loss programmes, tai chi, cane use, tibiofemoral bracing, topical NSAIDs for knee OA and oral NSAIDs for knee, and/or hip OA. Intra-articular glucocorticoid injections for knee and/or hip OA have also been strongly recommended in the ACR guideline [12].
However, there is a paucity of literature documenting the implementation of guidelines for OA management into system-wide chronic care osteoarthritis programmes. The implementation of such multimodal, multidisciplinary programmes to manage this cohort of OA patients has not been widely reported or disseminated. In fact, treatment of OA requires a comprehensive management approach. This is expected to benefit the people suffering from such disorder as well as health providers by improving the provided quality of care and subside their use of health services.
To tackle the increasing burden of OA, osteoarthritis care programme (OACP) provides a pathway to improved care for people suffering from this rapidly growing chronic condition. The programme involves a strategy not only to better management of patients’ pain but also the comorbidities associated with their OA. This may support the potential of delaying or reducing their need for joint replacement surgery. In time, it is expected this approach will serve as a model of care to be implemented in other outpatient health services in accordance with local needs and resources. This article outlines the proposed programme which is applicable to standard practice.
Methodology
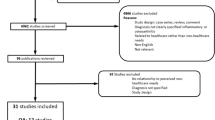
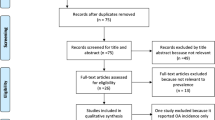
Given the broad and heterogeneous nature of the research questions to be addressed, a scoping review was considered the most appropriate methodological approach [13]. The working team formalised the research questions, searching for the relevant studies, agreeing on a strategy to select the relevant studies, charting the data, and finally collating, summarising, analysing, and presenting the results. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews (PRISMA-ScR) checklist was used to guide the reporting of this review [14].
Main text
Objectives
Several reasons have been linked to the persistent evidence-practice gap in the management of OA. These include high volume of patients, socio-economic status, health schemes, infrastructure, health care professionals training, and health policies implemented [15]. The title “Model of Care” is used to outline the way clinical health services are delivered and is being progressively applied to musculoskeletal conditions [16]. A “Model of Care” can be defined as an “evidence-informed strategy, framework or pathway that outlines the optimal manner in which condition specific care should be delivered to consumers within a local health system” [17]. The aim of a “Model of Care” is to clearly operationalise evidence-based guidelines and consequently endorse the implementation of such management recommendations by healthcare professionals in their local health centres [16]. The objectives of this “Model of Care” for osteoarthritis are:
-
1.
To set up and coordinate the inter-disciplinary, conservative management approach for patients diagnosed to have OA
-
2.
To have an algorithm for patients’ management particularly aiming to reduce the level of pain and improve their quality of life and functional status
-
3.
To endorse the value of patient education and self-management approach
Recognising the need to change
While there have been a growing number of “Model of Care” curricula published internationally for the management of OA [18,19,20], none have been published for local use in Egypt. Therefore, there was a vital need to formulate this programme based on the available evidence in the literature. Furthermore, understanding the principals of OA “Model of Care” is important to inform the services’ design for optimal care. Therefore, the need to change and set up this scoping review are:
-
1.
There is no national Action Plan for the management of Osteoarthritis.
-
2.
Current OA management is based on single practitioner or episodic care. Currently, there is no model of care available for care of OA patients within the context of chronic disease management.
-
3.
There are no current services provided to help patients improve their muscle power or reduce weight. The value of such approaches was evidenced by a large prospective cohort study which revealed that almost 70% of knee replacements are attributed to or associated with over-weight [21]. In addition, another study revealed that approximately 25–50% of all knee replacements could be avoided, if all overweight and obese people reduced their weight by 5kg, or to within the normal body mass index (BMI) range [22].
Patients: case identification and access to the programme
In the context of this work, model of care has been developed for adults and older adults diagnosed to have OA. For the purpose of this work, inclusion was only restricted to the hip and knee joints’ primary OA. Diagnosis may be based on clinical assessment and radiographic criteria. Access to the programme can be outlined as follows:
-
Once it is settled that a chronic care management programme is indicated for an individual’s OA, he/ she can be referred to the service. OA patients can be referred by any healthcare professional, or by self-referral.
-
OA patients (Knee or hip joints) will be considered eligible for the programme, if they meet two clinical criteria:
-
Their knee and/or hip pain has been persistent on most of the days of the last month.
-
Pain score using Visual Analogue Scale (VAS) is at least 4/10 at the first assessment.
-
-
Exclusion criteria for participation are history of hip fracture or total joint replacement within the past 12 months, or hip/ knee surgery within the past 6 months, untreated ligamentous injury, suspicion of tumour, inflammatory arthritis (e.g. rheumatoid arthritis, psoriatic arthritis), infectious and crystalline arthritis (gout and pseudogout), fibromyalgia, and chronic pain disorders.
-
For participants whose reported level of pain is below the VAS threshold, alternatives to OA management will be offered including simple analgesia, self-management as well as exercise programmes.
-
For all the OA patients whether included in the programme or not, special consideration will be given to the presence of modifiable risk factors for OA progression, such as obesity and poor muscle strength and control.
Case manager
The Rheumatology and Rehabilitation specialist will act as case manager for these OA patients referred to the programme with a view towards facilitating comprehensive management and improving the patients’ health- related quality of life abilities as well as self-management skills.
Patient-centred coordination of care
The level of coordination should be tailored to the individual patient’s needs and both medical and physical status. The patient’s problem may be primarily musculoskeletal or linked to an associated comorbidity or the individual psychosocial requirements.
All the patients included will have an initial face-to-face assessment where thorough medical examination will be carried out to assess their physical health, disease severity, quality of life, and psychological status as well as any existing co-morbidities. Based on this initial assessment, the appropriate management plan for the delivery of care will be identified and agreed with the individual patient.
Clinical indicators
-
Demographic data, marital status, occupation, and education level.
-
Clinical disease activity: active synovitis, mechanical derangement, hypermobility, meniscal damage, and ligament injury.
-
Disease severity assessment:
-
Knee and hip radiographs are assessed with Kellgren and Lawrence grading system [23]. Knee radiographs should be performed with the patient standing to reveal joint space narrowing, while weight bearing is not necessary for hip radiographs which include anteroposterior and lateral views.
-
US assessment to evaluate joint and periarticular abnormalities [24].
-
Assessment of functional disability using: Knee injury and osteoarthritis outcome score (KOOS) [25] and hip disability and osteoarthritis outcome score (HOOS) [26].
-
Health-related quality of life (QoL), psychological status using patient-reported outcome measures (PROMs) questionnaire [27].
-
Sarcopenia screening: SARC-F questionnaire [28]
-
Lab tests: vitamin D
-
Muscle power/sarcopenia measures (time up and go, chair stand tests [TUG], 400-m walk) [29].
-
Modifiable risk factors, comorbidity data.
Goals of the programme
Several goals have been identified for the management of OA patients; these include:
-
Manage and control of the patient’s symptoms including both pain and stiffness.
-
Optimise the patient’s functional ability
-
Optimise the patient’s quality of life
-
Slow the progression of the disease
-
Reduce the impact of the associated modifiable risk factors
-
Control the associated comorbidity(ies)
Principles of management
Putting principles into practice is vital to be able to achieve the goals of the programme set above, and secure optimum control of the patients’ symptoms as well as optimum functional ability and quality of life. These include:
-
Provide a systematic approach to osteoarthritis management
-
Endorse self-management
-
Set up a programme for weight reduction
-
Facilitate psychological management
-
Engagement in an appropriate exercise programme
-
Disease management patient education
Multidisciplinary intervention
As there is no single treatment that can be considered adequate/satisfactory for managing OA, a multifaceted approach has been agreed upon as the best strategy for managing this cohort of population (Fig. 1). Such a strategy involves both nonpharmacological and pharmacological therapies. These have been strongly recommended [12] particularly for OA affecting the weight-bearing joints, where mechanics and lifestyle play a major role in shaping the patients’ symptoms.
-
Non-pharmacological therapies:
-
Physiotherapy
-
Occupational therapy
-
Psychological support
-
-
Pharmacological therapies:
-
Review of medications
-
Pain management
-
Visco-supplement therapy
-

Multifaceted approach to the assessment and management of OA patients
Surgical referral
Acceleration to surgical intervention should be considered for aggressive/severe non-responsive cases whose disease progress over a relatively short period and is impacting negatively on the patient’s physical and mental status.
Documentation and data recording
Collecting datasets are essential for conducting post hoc analyses to inform approaches to OA management. Therefore, data will be collected prospectively for every patient including:
-
Every patient will complete a baseline patient-reported outcome measurement questionnaire.
-
Baseline patient’s body weight, height, BMI, BP, and basic lab tests are recorded.
-
The patient-centred management as well as discharge plan will be recorded.
-
Every patient will have a regular face-to-face review to monitor his/her progress and discuss the implementation of self-management approaches.
-
PROMs scores will be recorded before discharge.
-
Scores/lab measures reflecting the control of the associated comorbidity(ies) will be recorded.
Key performance indicators
Key performance indicators (KPI) are a pertinent part of measuring the successes and failures of the service provided. Knowing and measuring the right KPIs are important as it gives a value to compare against the current performance, hence helping to evaluate the outcomes faster. KPIs clearly demonstrate whether or not the targeted goals have been reached. Implementing KPIs as a standard in the service means that goals can be set, a strategy is devised to reach these goals, and evaluate performance along the way of implementing the programme. The KPI can be summarised as follows:
-
Percentage of the OA patients assessed and have a management plan agreed in relation to the total patients referred to the service.
-
Percentage of the patients who have already started their recommended management plan within 3 months of baseline valuation (cut off point documenting objective success will be 80%).
-
Percentage of the patients (measured as a proportion of KPI 1) who have completed their recommended management plan at 12 months of baseline valuation (objective success will be 80%).
Primary outcome
To reduce the level of pain, improve symptoms, prevent disability, and improve the quality of life of OA patients.
Secondary outcome
To ensure timely access to joint replacement treatment and ensure that the patient receives pre-surgery rehabilitation programme.
Discussion
With the increasing number of older population worldwide and the growing incidence of obesity, the burden of osteoarthritis (OA) is expected to upsurge. However, the understanding of the ailment remains limited, and there are indications that there is an evidence-practice gap in OA management and that several patients living with the disease are receiving suboptimal medical care. Furthermore, despite its high prevalence and negative impact on people’s health-related quality of life, it is frequently overlooked in both global as well as national strategic plans for chronic disease management. In fact, OA is more than just a “wear and tear” cartilage pathology. It is a disorder that involves the whole joint, which is an organ in its own. OA is therefore considered an organ “joint” failure. The joint is a complex of various structures, including cartilage, bone, synovial membrane, muscles, nerves, and ligaments. Therefore, the consequences of its failure will expand beyond the limits of degeneration to include inflammation, bone deformity, and mechanical as well as neurological dysfunction. The growing healthcare utilisation and cost of joint replacement make the current socioeconomic impact of OA unsustainable and represent a major worldwide challenge [30, 31]. Therefore, when considering OA management, a “paradigm shift” is highly required to replace of the current “episodic care” implemented in standard practice. This highlights the value of having such multidisciplinary “models of care” for OA to be implemented in the day-to-day medical care. Such approach is expected to indorse the evidence-informed OA management and addresses the underutilised and underemphasised core recommended therapeutic approaches.
In conclusion, this scoping review has developed a “Model of Care” for people living with OA which can be implemented in standard practice. The results will give insight into the features, performance, results, and outcome measures assessed. It will also guide future research towards how “Model of Care” can be patient-centred and tailored to the individual medical status.
Availability of data and materials
Not applicable (NA)
Abbreviations
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- HOOS:
-
Hip disability and osteoarthritis outcome score
- KPI:
-
Key Performance Index
- KOOS:
-
Knee injury and osteoarthritis outcome score
- OA:
-
Osteoarthritis
- OACP:
-
Osteoarthritis care programme
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
- PROMs:
-
Patient-reported outcome measures
- QoL:
-
Quality of life
- VAS:
-
Visual Analogue Scale
References
Cisternas MG, Murphy L, Sacks JJ, Solomon DH, Pasta DJ, Helmick CG (2016) Alternative methods for defining osteoarthritis and the impact on estimating prevalence in a US population-based survey. Arthritis Care Res (Hoboken) 68:574–580
GBD 2015 DALYs and HALE Collaborators (2016) Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388:P1603–P1658
Murphy L, Schwartz TA, Helmick CG, Renner JB, Tudor G, Koch G et al (2008) Lifetime risk of symptomatic knee osteoarthritis. Arthritis Rheum 59:1207–1213
Murphy LB, Helmick CG, Schwartz TA, Renner JB, Tudor G, Koch GG et al (2010) One in four people may develop symptomatic hip osteoarthritis in his or her lifetime. Osteoarthr Cartil 18:1372–1379
Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL (2015) In: Fransen M (ed) Exercise for osteoarthritis of the knee. Wiley, Chichester
Fransen M, McConnell S, Hernandez-Molina G, Reichenbach S (2014) Exercise for osteoarthritis of the hip. Cochrane Database Syst Rev 22(4):CD007912
Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG et al (2013) EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis 72(7):1125–1135
Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J et al (2012) American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken) 64(4):465–474. https://doi.org/10.1002/acr.21596 Epub 2012/05/09
The Swedish National Board of Health and Welfare—National guidelines for orthopaedic conditions. Available from: http://www.socialstyrelsen.se/nationalguidelines/nationalguidelinesfororthopaedicconditions. Accessed 29 Oct 2022
Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA et al (2019) OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil 27(11):1578–1589. https://doi.org/10.1016/j.joca.2019.06.011 Epub 2019/07/07
Juhl C, Christensen R, Roos EM, Zhang W, Lund H (2014) Impact of exercise type and dose on pain and disability in knee osteoarthritis: a systematic review and meta-regression analysis of randomized controlled trials. Arthritis Rheumatol 66(3):622–636
Kolasinski SL, Neogi T, Hochberg MC, Oatis C et al (2020) 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res (Hoboken) 72(2):149–162
Arksey H, O'Malley L (2005) Scoping studies: towards a methodological framework. Int J Soc Res Methodol 8(1):19–32
Tricco AC, Lillie E, Zarin W et al (2018) PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 169(7):467–473
Briggs AM, Bragge P, Slater H et al (2012) Applying a Health Network approach to translate evidence-informed policy into practice: a review and case study on musculoskeletal health. BMC Health Serv Res 12:394
Speerin R, Slater H, Li L et al (2014) Moving from evidence to practice: models of care for the prevention and management of musculoskeletal conditions. Best Pract Res Clin Rheumatol 28(3):479–515
Briggs AM, Towler SCB, Speerin R et al (2014) Models of care for musculoskeletal health in Australia: now more than ever to drive evidence into health policy and practice. Aust Health Rev 38(4):401–405
Smink AJ, van den Ende CH, Vliet Vlieland TP et al (2011) “Beating osteoARThritis”: development of a stepped care strategy to optimize utilization and timing of non-surgical treatment modalities for patients with hip or knee osteoarthritis. Clin Rheumatol 30(12):1623–1629
Hunter DJ, Hinman RS, Bowden JL et al (2018) Effectiveness of a new model of primary care management on knee pain and function in patients with knee osteoarthritis: Protocol for THE PARTNER STUDY. BMC Musculoskelet Disord 19(1):132
Cunningham J, Doyle F, Ryan JM, Clyne B, Cadogan C, Cottrell E, Smith SM, French HP (2021) Primary care-based models of care for osteoarthritis: a scoping review protocol. HRB Open Res 4:48
Liu B, Balkwill A, Banks E, Cooper C, Green J, Beral V (2007) Relationship of height, weight and body mass index to the risk of hip and knee replacements in middle-aged women. Rheumatology 46(5):861–867
Coggon D, Reading I, Croft P, McLaren M, Barrett D, Cooper C (2001) Knee osteoarthritis and obesity. Int J Obes Relat Metab Disord 25(5):622–627
Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16:494–502. https://doi.org/10.1136/ard.16.4.4941006995
Iagnocco A (2014) Ultrasound in osteoarthritis. Clin Exp Rheumatol 32(1 Suppl 80):S48–S52
Rooscorresponding EM, Stefan L, Lohmander. (2003) The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes 1:64
Nilsdotter AK, Lohmander LS, Klässbo M, Roos EM (2003) Hip disability and osteoarthritis outcome score (HOOS)-validity and responsiveness in total hip replacement. BMC Musculoskelet Disord 4:10
El Miedany Y, El Gaafary M, El Arousy N, Ahmed I, Youssef S, Palmer D (2012) Arthritis education: the integration of patient-reported outcome measures and patient self-management. Clin Exp Rheumatol 30(6):899–904
Malmstrom TK, Miller DK, Simonsick EM et al (2016) SARC-F: a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J Cachexia Sarcopenia Muscle 7:28–36
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M (2019) Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 48(1):16–31
Hawker GA (2019) Osteoarthritis is a serious disease. Clin Exp Rheumatol 37 Suppl 120(5):3–6
Cross M, Smith E, Hoy D et al (2014) The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis 73(7):1323–1330
Acknowledgements
No acknowledgements.
Funding
Nothing to declare.
Author information
Authors and Affiliations
Contributions
The authors shared writing the manuscript, revising the draft and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
NA
Consent for publication
NA
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Miedany, Y., Elwakil, W. Multidisciplinary patient-centred model of care for osteoarthritis: scoping review protocol—an initiative by the Egyptian Academy of Bone Health. Egypt Rheumatol Rehabil 50, 3 (2023). https://doi.org/10.1186/s43166-023-00170-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-023-00170-4