
Abstract
Background
Lupus nephritis (LN) affects a substantial number of the patients living with Systemic lupus erythematosus (SLE), representing a major cause of morbidity and mortality. Patients with lupus nephritis should be referred to a lupus nephritis expert who can confirm the diagnosis, assess the level of disease activity, and offer guidance on treatment and monitoring of the disease, as well as its consequences and side effects. The aim of this guideline was to develop recommendations for the management of adult lupus patients, including lupus nephritis diagnosis, assessment, and monitoring.
Nineteen key clinical questions were identified by scientific committee according to the Patient/Population, Intervention, Comparison, Outcomes and Timing (PICOT) approach. Literature review team performed a systematic review to summarize evidence advocating the benefits and harms of available pharmacologic and nonpharmacologic therapies for LN. Subsequently, recommendations were formulated. The level of evidence was determined for each section using the Oxford Centre for Evidence-based Medicine (CEBM) system. A 2-round Delphi process was conducted with 24 experts. All rounds were conducted online. A consensus was achieved on the direction and the strength of the recommendations.
Results
An online questionnaire was sent to an expert panel who participated in the two rounds (response rate 100%). At the end of round 2, a total of 19 recommendation items, categorized into 11 sections to address the main LN categories, were obtained. The percentage of those who agreed with the recommendations (ranks 7–9) ranged from 90.5 to 100%. The phrasing of all 19 clinical standards identified by the scientific committee was agreed upon (i.e., 75% of respondents strongly agreed or agreed).
Conclusion
These recommendations provide an updated consensus on the pharmacological treatment of lupus nephritis and strategies to reach optimal treat to target outcomes in common clinical scenarios, based on a combination of evidence and expert opinion. Best treatment decisions should be tailored to each individual patient situation.
Similar content being viewed by others


Background
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by the production of autoantibodies and the deposition of immune complexes, affecting a broad range of systemic affection and causing variable degrees of organ damage. Consequently, progressive accumulation of irreversible organ damage remains the predominant cause of mortality in SLE patients [1, 2]. Lupus nephritis (LN) affects a substantial number of the patients living with SLE, representing a major cause of morbidity and mortality. Up to 40% of SLE patients develop kidney disease [3]. Overall survival in patients with SLE is approximately 95% at 5 years after diagnosis and 92% at 10 years. The presence of lupus nephritis significantly reduces survival, to approximately 88% at 10 years [4, 5]. In spite of treatment, 10% of persons with LN develop end-stage kidney disease (ESKD) [6]. These findings have been endorsed by the outcomes of earlier studies which clearly indicated that once irreversible damage ensues in SLE, especially early in the course of the disease, it has a direct impact on the prognosis [7, 8].
The treat-to-target (T2T) strategy has proven its efficacy in the management of several chronic medical illnesses including rheumatoid and spondylo-arthritis. However, in SLE with its multi-organ affection, the possibility of implementing the T2T principle has become a topic of discussion. A European panel of rheumatologists [9] was in favor of implementing the concept of treat to target for SLE treatment of SLE which should target at several goals including control of disease activity, prevention of disease flares, minimization of disease or treatment-related comorbidity, and improvement of quality of life. However, implementing the T2T concept specifically in LN remains another challenge in this cohort of patients. Several features of this condition influence the decision to use a treat-to-target (T2T) strategy. Furthermore, until recently, outcomes of targeted treatment strategies were unsatisfactory in terms of complete renal response, prevention of relapses, chronic kidney disease (CKD), and progression to end-stage kidney disease. To improve the LN prognosis, recent data [10] suggested that treatment approaches should be modified to (1) adapt the current treat-to-target approach to include, in addition to a clinical target, a pathological target and (2) switch from the conventional sequential therapeutic approach to combination therapy policy.
As Egypt has launched a nationwide universal health coverage in 2020, setting up guidelines for management of patients is vital to the process. Therefore, there was a real need to update the treatment recommendations for LN management. Treatment recommendations are developed aiming at several goals: optimize the standards of clinical care, minimize inadequate management variance, and establish quality control parameters and also, to update clinicians, principally in a landscape of changing therapeutics, highlighting where there is evidence to guide treatment decisions, promoting resource efficiency, and highlighting the research that needs to be done to improve future care [11]. This consensus main objective is to provide updated, evidence-based recommendations for treat-to-target management of lupus nephritis and its associated clinical manifestations. Although these guidelines were developed for Egyptian patients with LN, we hope that they would be helpful to rheumatologists all over the world.
Methods
Design
A multistep procedure was used to create evidence-based, consensus therapy recommendations for lupus nephritis. The study was designed utilising the “Clinical, Evidence-based, Guidelines” (CEG) guideline creation process methodology, which involves a scientific data and consensus approach based on established scientific evidence and clinical experience. The publication adhered to the required reporting elements for systematic reviews and meta-analyses criterion [12].
Development stages
Core team
This team included of two rheumatologists and two nephrologists with deep experience of LN management. The core team oversaw and organized the team’s efforts, aided in the development of the project’s scope and initial Population, Intervention, Comparison, Outcomes (PICO) clinical questions, and came to an agreement on the essential questions to be included in the recommendations. The core team identified outcomes as critical for each PICO question’s systematic literature review. The group was also in responsible of choosing the expert panel and putting together the manuscript.
Key questions used to develop the guideline
The suggestions were based on a series of structured key questions that identified the target audience, treatment, enquiry, comparison(s), and outcomes that were used to measure efficacy, effectiveness, or risk. To acquire evidence to answer the clinical questions, researchers employed the following methods: formulation of clinical questions, question structure, evidence search, critically selection and evaluation of evidence, presentation of the results, and suggestions. The questions guiding the systematic literature search and, as a results, the clinical treatment guidelines are shown in Table 1.
Literature review team
The literature study was carried out with the help of a methodology specialist, under the supervision of experienced literature review consultant, and was based on the study questions selected to focus on the management of LN. A systematic literature search was conducted utilising the PubMed/MEDLINE, EMBASE, and Cochrane databases to get sufficient evidence-based baseline knowledge for considerations. Following data abstraction, evaluation of published recommendations, and quality of evidence grading [13, 14], the specialists in charge of the literature review revised the list of propositions for the management of LN based on available research evidence and their own clinical competence. The Oxford Centre for Evidence-based Medicine (CEBM) approach was used to establish the degree of evidence for each section [14].
Data sources and search strategies
The search approach was designed to find all studies having adults living with LN as the study population. The literature search was conducted using the PICO questions. Randomized clinical studies testing the diagnosis and efficacy of LN management, as well as quality improvement outcomes/approaches, were found using literature search methodologies.
The keywords used were determined by the PICO elements utilized in various combinations. Namely, clinical (search terms: diagnosis, clinical manifestations, classification, clinical features, presentation), Lab (search terms: immunology/Immunological, antibody/auto-antibody/serological, anti-nuclear antibodies, ANA, anti-dsDNA, anti-Ro, anti-Sm, C3, C4, antiphospholipid, anticardiolipin, lupus anticoagulant), LN features (assessment, disease activity, monitoring, damage, prognosis, quality indicators, recommendations), and LN treatment (treatment or therapy). PubMed and Cochrane Database of systematic reviews databases were being searched on January 14, 2022, and Embase was being searched on January 16, 2022. Electronically, duplicate screening of literature search results was performed. Additional studies that satisfied the inclusion requirements were found by looking through the reference lists of research indicate using database search tools.
Study selection
Relevant studies were chosen using inclusion and exclusion criteria applied to the literature found using the search methodologies.
Inclusion criteria
Articles included were systematic reviews, randomized controlled trials (RCTs), uncontrolled trials, observational studies including cohort, case-control and cross-sectional studies, or those where economic evaluation was made. Trials were eligible if they included people with LN regardless of age or sex, from any health care setting receiving any therapy. The included studies should have the criteria of classification evidence and recommendations used identified. Also, the formal process for establishing recommendations (Delphi exercise, panel conference) outlined.
Exclusion criteria
Editorials, commentaries, conference abstracts, and non-evidence-based narrative/personal reviews, manuscripts lacking of English version, were excluded.
Ethical aspects
The Helsinki Declaration was followed when doing this research. The local ethical committee approved the Clinical, Evidence-based, Guidelines (CEG) initiative protocol: ethical approval code: 34842/8/21, ethical board Tanta University. All study participants were required to provide informed consent. All individuals were kept anonymous in compliance with data protection regulations.
Expert panel
Twenty-four people were nominated by the core leadership team (20 rheumatologists, 3 nephrologists, one internist with special interest in rheumatology). Professional skill and experience (at least 8 years) in the area of rheumatology, management of inflammatory arthritis, notably SLE and LN, and active participation in rheumatic illness scientific research were among the criteria for their selection. The expert panel endorsed the project’s scope as well as the preparation of the PICO questions. The PICO questions were transformed into recommendation sentences and delivered to the expert panel for voting along with the evidence report.
Target audience
The guideline was created to assist health care providers who manage LN patients. The guideline should also be useful to patients and those responsible for managing SLE care in the National Health Service.
Developing the clinical care standard framework
Based on responses to the structural key questions and the literature review, a structured template was created to aid in the consistent identification of guideline components. The format in which the recommendations/information will be delivered and extracted has been identified for each guideline component.
Delphi process
The Delphi method [15] is a systematic method for acquiring critical information on a certain topic. It is based on the assumption that group forecasts are more precise than individual estimates. The Delphi method’s purpose is to generate structured iterative consensus forecasts from a group of experts. Its method is based on a set of “rounds” of expert questions. The stages of the Delphi technique are usually as follows: (1) a group of experts is put together. (2) Forecasting tasks/challenges are assigned to professionals and spread. (3) Experts provide preliminary predictions and justifications. In order to provide input, these are collated and summarized. (4) The experts receive comments, which they consider when revising their forecasts. This process can be repeated until there is a reasonable degree of agreement. (5) The final forecasts are created by combining the forecasts of the experts. The anonymity of participants and the controlled feedback are two key features of this strategy [15,16,17].
Consensus process
To reach consensus on the T2T technique in LN, three Delphi rounds were conducted. The structured Delphi method ensures that all participants’ opinions are taken into account equally. Online surveys were used to conduct the Delphi method. The computerized questionnaire’s initial round contained 11 domains related to LN T2T strategy.
Voting process
There were two rounds of live online voting, each with a stringent time limit. All task force members were invited to vote, and the beginning and finish timings of each round were publicized in advance. Votes were collected and processed anonymously, and special access links were sent forth. For each statement, comments on rephrasing, potential confusion, and unidentified overlaps were received at the same time as the voting process. Only the task force members were allowed to vote on the statements.
Rating
Each statement was assessed on a scale of 1 to 9, with 1 representing “total disagreement” and 9 representing “complete agreement.” 1–3, 4–6, and 7–9, respectively, signify disagreement, uncertainty, and agreement. It was not necessary for members to vote on all statements, and they were encouraged to do so if they felt a statement was outside their area of competence. “Inconvenience concerning the veracity of the recommendation” is represented by an “uncertainty” vote. All statements allowed for the submission of comments, which the scientific committee assessed following each round of voting. Members were encouraged to offer comments during all rounds of voting, especially when there was a disagreement. This allowed the panel to spot a case of statement misinterpretation and invalidate the vote on that statement.
Definition of consensus
Prior to data analysis, a consensus definition was established. Consensus was attained, and this guideline became a suggestion if at least 80% of respondents obtained agreement (scores 7–9) or disagreement (scores 1–3). A statement was retired if it earned a mean vote of less than 3 or a “bad” degree of agreement. Statements having an ambiguity score of 4–6 were altered as a result of the input. If all votes on a statement dropped into the agreement bracket after the second round of voting (7–9), the levels of agreement on that statement were considered “strong” [17,18,19].
Chronogram of Delphi rounds
The first round took place on January 29 and February 1, 2022 (4 days). In view of the feedback, the aspects on which respondents could not agree in the first round were updated and included in the second round. The second round began on February 4, 2022, 3 days after the first round, and lasted 9 days (till 12 Feb 2022).
Results
Literature research and evidence selection
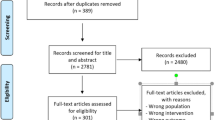
By using a search strategy, we identified 3174 possibly relevant studies during the research selection phase. 3013 were excluded: 406 duplicates and 2607 by title and abstract screening (studies did not examine population or intervention of interest, did not match study design of interest, or did not report outcome measures of interest). As a result, 161 studies were selected for full-article evaluation. Due to the fact that 133 research did not provide evidence that matched a PICO, only 28 studies were considered in this study (Fig. 1).

Flow chart for the study selection process
Expert panel characteristics
The Delphi form was sent to expert panel (n=24), of whom 24 (100%) completed in the two rounds. The participants were from governorates and health centres throughout Egypt: Ain Shams University (n=4, 16.6%), Cairo University (n=7, 29.2%), Tanta University (n=2, 8.3%), Benha University (n=2, 8.3%), South Valley University (n=1, 4.15%), Alexandria University (n=1, 4.15%), Fayoum University (n=1, 4.15%), Sohag University (n=1, 4.15%), Zagazig University (n=1, 4.15%), Assiut University (n=1, 4.15%), Minia University (n=1, 4.15%), Ministry of Health (n=1, 4.15%), in addition to (n=1, 4.15%) international expert from the UK. 83.4% of the experts’ panel (20) were rheumatologists and 16.6% (4) were nephrologists.
Delphi round 1
The clinical question round was made up of 19 questions divided into 11 categories (Table 1) including targeted patients, treatment target, renal biopsy, lab tests, treatment of lupus nephritis, management outcome, management of refractory lupus nephritis, pregnancy and lupus nephritis, patient’s education and lifestyle advice, comorbidities screening, and novel treatments facilitating T2T of lupus nephritis. Each domain entails one or more elements. Participants were asked to evaluate the overall principles considered in LN T2T management decision-making in this round. The experts’ panel responded 100% (24/24) in round one. All domains and questions were agreed upon (with 80% of respondents strongly agreeing or agreeing), and no questions were retired.
Delphi round 2
Based on the literature research, a list of 11 domains with 19 recommended suggestions was generated using the input from round 1, 2 for targeted patients and 1 for the treatment target, 2 for the renal biopsy, 1 for the lab tests, 7 for treatment of lupus nephritis, 1 for management outcome, 1 for management of refractory lupus nephritis, 1 for pregnancy and lupus nephritis, 1 for patient’s education and lifestyle advice, 1 for comorbidities screening, and 1 for novel treatments facilitating T2T of lupus nephritis. The response rate for round 2 was 100% from the experts’ panel (24/24). Modifications of the words were suggested for 4 statements (1 in the investigations, 2 in the treatment, and 1 in the outcomes). The statements were modified and amended. For all statements, the consensus was reached (as ≥ 80% of respondents strongly agreed or agreed).
Based on those results, this document was written, containing the answers to the key clinical questions which entails recommendations for the management of lupus nephritis, as follows:
General principles
Level of evidence: 1, grades of recommendations (GoR): A, mean+SD: 8.9+0.5, percentage of agreement: 100%
Level of agreement: High
-
Management of lupus nephritis should adopt a multidisciplinary approach, in specialized centers. The team should include both rheumatologists and nephrologists, adopting a shared decision-making process with the patients.
-
Because of slower proteinuria recovery in these patients, prompt switching of therapies is not necessary as long as proteinuria is improving.
-
It is fairly straightforward to establish the target in a T2T management approach for lupus nephritis. Lupus nephritis management is based on both clinical (e.g., hypertension, lower limb oedema, fluid overload symptoms and signs) and laboratory measures (e.g., proteinuria, erythrocyturia, RBC casts, and serum creatinine). Reappearance of glomerular hematuria or cellular casts can be a predictor of impending kidney flare [20].
Treat to target management strategy for lupus nephritis
-
1.
Establishment of target(s) tailored to the patient condition and prospects (individual patient’s clinical condition/patient’s requirements and expectations)
-
2.
Identify the management plan to achieve the target (medications/dose adjustments)
-
3.
Monitor case progression till target achievement
-
4.
Optimization of the management strategy (response to therapy, dose adjustment, side effects, comorbidities)
-
The use of combined immunosuppressive (“multitarget”) therapy and reducing the dosages of concomitant glucocorticoids have been suggested in some cases to increase efficacy, lower toxicity, or both
Who are the targeted patient?
Level of evidence: 1, GoR: A, mean+SD: 8.77+1.7, percentage of agreement: 95.2%,
Level of agreement: High
-
SLE patients who develop nephritis
-
SLE patients, with poor prognostic markers for LN (at high risk of developing lupus nephritis:
-
The presence of hypertension, hypercreatininemia/renal failure, massive proteinuria, and high activity index score of LN.
What is the classification system for lupus nephritis?
Level of evidence:1, GoR: A, mean+SD:8.8+0.5, percentage of agreement: 100%,
Level of agreement: High
According to the World Health Organization (WHO) and subsequent clinicopathologic data [21],
-
Class I and II are used for purely mesangial involvement:
-
I: mesangial immune deposits without mesangial hypercellularity.
-
II: mesangial immune deposits with mesangial hypercellularity).
-
Class III for focal glomerulonephritis (involving <50% of total number of glomeruli) with subdivisions for active and sclerotic lesions.
-
Class IV for diffuse glomerulonephritis (involving ≥50% of total number of glomeruli) either with segmental (class IV-S) or global (class IV-G) involvement and also with subdivisions for active and sclerotic lesions.
-
Class V for membranous lupus nephritis.
-
Class VI for advanced sclerosing lesions.
Combinations of membranous and proliferative glomerulonephritis (i.e., classes III and V or classes IV and V) should be reported individually in the diagnostic line.
What are the targets of lupus nephritis treatment?
Level of evidence: 1, GoR: B, mean+SD: 8.67+0.82, percentage of agreement: 100%
Level of agreement: High
Short term
-
Improved proteinuria levels by 3 months, and a 50% reduction in proteinuria (partial clinical response) by 6 months.
-
By 12 months, therapy should aim for proteinuria <0.5 g per 24 h, normal or stable renal function and an inactive urinary sediment (complete clinical response).
-
Nephrotic-range proteinuria at baseline: an additional 6 to 12 months may be required to reach complete clinical response.
Long term
-
Inducing and maintaining remission of the kidney inflammation so as to preserve renal function and improve survival in the long term.
-
Prevent chronic kidney disease and end-stage renal disease.
-
Minimize LN flares.
-
Improve disease-related quality of life [22].
What are the indications for a renal biopsy in an SLE patient?
Level of evidence: 1, GoR: A, mean+SD: 8.3+2.28, percentage of agreement: 95.2%
Level of agreement: High
-
Increasing serum creatinine levels without a compelling reason (e.g., hypovolemia and medication)
-
Confirmed proteinuria of ≥ 1 g/24 h
-
Proteinuria ≥ 0.5 g/day plus hematuria or cellular casts
What is the importance of evaluating biopsies for the extent of activity or chronicity?
Level of evidence: 2, GoR: B, mean+SD: 8.5+1.25, percentage of agreement: 90.5%
Level of agreement: H
Pathologists used to generate a calculated score to signify disease activity and chronicity on a kidney biopsy report [23]. Though these formulas are no longer widely used, identifying histologic changes that signify chronicity and activity can help with the overall description of the renal biopsy. Fibrosis indicates a chronic scarring illness that is less likely to respond to treatment.
When following a patient with lupus nephritis, which serologic tests are most useful?
Level of evidence: 1, GoR: A, mean+SD: 8.5+0.82, percentage of agreement: 100%
Level of agreement: High
-
Anti-dsDNA can be elevated with disease flare.
-
Complement component levels decreased complement component levels (e.g., C3 and C4) as well as total hemolytic complement (CH50), correlate also with the renal disease activity. (Many lupus patients have partial C4 deficiency so may have a low C4 level. In those patients, only C3 levels can be followed) [24].
-
Glomerulonephritis can develop in a patient with SLE who has no anti-dsDNA antibodies and normal complement levels (especially in membranous lupus nephritis).
Which patients with severe lupus nephritis are more likely to progress to end-stage renal disease (ESRD)?
Level of evidence:2, GoR: A, mean+SD: 8.67+1.12, percentage of agreement: 95.2%
Level of agreement: High
-
Lower socioeconomic status
-
Poor medication compliance
-
Comorbidities such as diabetes and hypertension
-
Failure to normalize serum creatinine or serum creatinine of >2mg/dL on therapy
-
Failure to decrease proteinuria to <1 g/day within 6 months of starting treatment
-
Renal biopsy evidence of high disease activity (cellular crescents) and chronicity (interstitial fibrosis) [25]
Management strategy for LN
What is the first line of therapy for patients with severe lupus nephritis?
Level of evidence: 1, GoR: A, mean+SD: 8.43+1.48, percentage of agreement: 95.2%
Level of agreement: High
-
A)
Induction therapy
-
Class III/IV lupus nephritis
-
Intravenous (IV) pulse methylprednisolone (500 mg to 1 g) daily for 3 days followed by prednisone 1 mg/kg/ day (crescents on biopsy) or 0.5 mg/kg/day (no crescents). Taper after few weeks to lowest effective dose
-
-
Plus
-
Mycophenolate mofetil (MMF) 2–3 g/day for 6 months or cyclophosphamide (CYC) in 2 different regimens:
-
High-dose IV regimen (500–1000 mg/m2 monthly × 6 doses)
-
Low-dose IV regimen (Euro-lupus: 500 mg IV every 2 weeks × 6 doses)
-
-
Patients who fail improving on MMF, switching to CYC is considered. Patients who fail to respond to CYC consider switching to MMF.
-
In patients who fail responding to both, they are candidates for rituximab, calcineurin inhibitors (cyclosporine, tacrolimus), or a combination of calcineurin inhibitors and low-dose MMF.
-
The combination of MMF with a calcinurine inhibitors (CNI) (especially tacrolimus (TAC) might be a therapeutic option, especially in nephrotic-range proteinuria
-
Anticoagulant therapy: Anticoagulant therapy should be considered in nephrotic syndrome with heavy proteinuria and serum albumin less than 20 g/L.
Class V lupus nephritis
-
Oral prednisone 0.5 mg/kg/day for 6 months; plus MMF 2–3 g/day for 6 months
-
Calcineurin inhibitors (cyclosporine/tacrolimus) can be added to MMF: use caution in patients with renal insufficiency or hypertension.
-
IV CYC if other therapies fail
-
B)
Adjunctive therapies
-
Hydroxychloroquine
-
Angiotensin-converting enzyme (ACE) inhibitor or angiotensin-receptor blocker (ARB) if proteinuria ≥0.5 g/24 h
-
Control blood pressure (BP): should be ≤130/80
-
Statin therapy if low-density lipoprotein (LDL) cholesterol >100 mg/dL
-
Stop smoking
-
Counsel against pregnancy while nephritis is active or creatinine >2mg/dL
-
Which cytotoxic agents are most frequently used for maintenance therapy in the treatment of lupus nephritis?
Level of evidence: 1, GoR: A, mean+SD: 8.67+0.82, percentage of agreement: 100%
Level of agreement: High
-
After induction therapy, maintenance therapy is provided to ensure a long-term response.
-
Hydroxychloroquine 200–400 mg/day
-
oral AZA (up to 2 mg/kg/day) or MMF; which is generally preferred (1–3 g/day)
-
Patients on allopurinol (gout) or warfarin should avoid azathioprine (AZA) (warfarin resistance)
-
Patients who cannot tolerate AZA or MMF can get CYC IV every 3 months after induction.
-
Prednisone is tapered over time if renal and extra-renal manifestations are in control.
-
Maintenance therapy is recommended for at least 1–2 years (or longer)
-
Other maintenance therapies
-
Rituximab or Blimumab
-
Calcineurin inhibitors (cyclosporine, volcosporin, or tacrolimus): alone or combined with low-dose MMF.
-
Drugs used in LN
-
I.
Cyclophosphamide
-
Is there an optimal dosing regimen for CYC?
-
Level of evidence: 1, GoR: A, mean+SD: 8.7+0.82, percentage of agreement: 100%
Level of agreement: High
-
The two commonly recommended IV regimens are as follows:
-
High dose: Monthly boluses of 0.5–1.0 g/m2 IV × 6 months
-
Low dose (Euro-Lupus protocol): 500 mg IV every 2 weeks × 6 doses
-
Low-dose therapy is associated with fewer serious infections and less risk of infertility, but some patients may fail to respond to lower doses
-
IV dosing regimens (compared with oral) result in a lower total CYC exposure, which is important when considering effects on fertility and bladder toxicity.
-
Premature ovarian failure risks correlate with the cumulative dose of CYC (>10–15 g total dose) and the age of the patient (>30 years) [26].
-
Anti-Mullerian hormone measurement can be used to determine ovarian reserve, but its clinical value is unclear.
Consider rituximab 1 g IV plus CYC 500–750 mg IV for resistant disease, followed by the same 14 days later.
-
Describe a protocol for using monthly IV CYC
Level of evidence:1, GoR: A, mean+SD:8.57+1.12, percentage of agreement: 100%
Level of agreement: High
-
a)
Prior to CYC
-
Premedication 15–30 min prior to CYC: dexamethasone 10 mg, and ondansetron (Zofran) 8 mg or ganisetron (Kytril) 1 mg in 100 cc normal saline IV
-
Mesna (25% of CYC dose in milligrams) in 250 cc normal saline
-
-
b)
CYC infusion
-
CYC 0.5–1.0 g/m2 of a body surface area in 1000 cc normal saline for initial dose. If creatinine clearance is less than 35–40 cc/minute, then start initial dose at 0.5 g/m2 of bovine serum albumin. If on dialysis, give 0.4–0.5 g/m2 8–10 h before or after dialysis.
-
-
c)
Post CYC infusion
-
Mesna (25% of CYC dose in mg) in 250 cc normal saline
-
-
d)
Follow-up patients for hematuria and cancer bladder whenever feasible.
-
e)
To prevent premature gonadal failure from long-term therapy, consider using gonadotropin-releasing hormone (Leuprolide) 3.75 mg intramuscularly (IM) 10 days prior to each monthly CYC dose or testosterone supplementation (200 mg IM every 2 weeks) for men (data is limited) [20].
-
e) Maintenance after the CYC course
-
Maintenance with AZA or MMF
-
-
II.
B cell therapy in lupus nephritis
-
Role of B cell depletion therapy
-
Lupus nephritis is characterized by a complicated interplay of immunologic disturbances and renal damage caused by the development of pathogenic autoantibodies and immune complexes, which activate complement and cause inflammatory cell infiltration in the kidney. B lymphocytes are key players in this process because they are the progenitors of plasma cells, which create pathogenic autoantibodies, and they also serve as antigen presenters for T lymphocytes [27].
-
Rituximab (anti-CD20)
Loading: 1 g on days 1 and 15
Maintenance dose: 500 mg IV every 6 months
-
Ocrelizumab (anti-CD20)
The first dose is a 300-mg intravenous infusion given over 2.5 h, followed by another 300 mg intravenous infusion 14 days later.
Then, every 6 months, a 600-mg intravenous infusion is given over 3.5 h.
-
Obinutuzumab (anti-CD20) [28]
Obinutuzumab is a humanized type II anti-CD20 monoclonal antibody that binds to the CD20 antigen in a different way than type I anti-CD20 antibodies (1000mg/40ml).
-
Epratuzumab (anti-CD22)
-
Epratuzumab is a recombinant humanized monoclonal IgG antibody to CD22 that promotes antibody-dependent cellular cytotoxicity and depletes B cells. Epratuzumab is thought to alter B cell function without killing them; however, the exact mechanism of action is unknown.
-
Targeting B cell survival factors
-
-
Belimumab
Indicated for active lupus nephritis in patients who are receiving standard therapy.
IV
Initial: 10 mg/kg IV q 2 weeks x 3 doses, THEN
Maintenance: 10 mg/kg IV q 4 weeks
SC
Initial: 400-mg dose (two 200-mg injections) sc q week x 4 doses, THEN
Maintenance: 200 mg sc q week thereafter. Transitioning from IV to SC dosing at any time after completing the first 2 IV doses.
If transitioning, administer first sc dose of 200 mg 1–2 weeks after the last IV dose [29].
-
Atacicept
Atacicept inhibits B cell stimulation by binding to both BLys and a proliferation-inducing ligand (APRIL). Atacicept is thought to impair mature B cells and plasma cells while having little effect on progenitor and memory B cells.
What is the strategy for management of refractory Lupus nephritis?
Patients with refractory LN are those who do not obtain a partial response after 6–12 months, or whose LN worsens after 3 months, or who have treatment failure as determined by the treating physician after 6 months [30].
-
Several therapeutic options are available, including the following:
-
Switching from CYC to MMF or vice versa
-
For patients with refractory LN, switching to a different first-line induction therapy is the suggested first step, according to both the EULAR/ERA-EDTA and the American College of Rheumatology guidelines. CYC-resistant patients are usually treated with MMF, while MMF-resistant patients are treated with CYC. Some patients combine switching immunosuppressive medications with three days of intravenous glucocorticoids pulses [31].
-
Prolonged courses of cyclophosphamide
Patients who do not satisfy remission criteria after 6 months may be eligible for extended CYC therapy. The severe treatment toxicities of CYC, including as infertility, urotoxicity, and oncogenicity, which are especially relevant because the majority of patients are of reproductive age, constitute a major limitation [32].
-
B cell therapies
B cells play a principal role in the pathogenesis of LN and are therefore attractive therapeutic targets as Rituximab (RTX) and Belimumab [33, 34].
-
Calcineurin inhibitors
The CNIs cyclosporine A (CSA) and tacrolimus have been widely researched in LN, with rising evidence for their efficacy in refractory LN. CSA binds to cyclophyllin, its cytoplasmic receptor, and the resulting drug-receptor complex binds to calcineurin and inhibits IL-2 synthesis, resulting in a selective and reversible suppression of T cell-mediated immune response. CSA has been demonstrated to have direct antiproteinuric effects in addition to its immunosuppressive effects. The mechanism is linked to actin stabilization in podocytes. Tacrolimus binds to the FK-binding protein-12, a distinct cytoplasmic receptor that interacts with calcineurin [35].
Volcosporin
This is indicated in combination with a background immunosuppressive therapy regimen for active lupus nephritis (LN) 23.7 mg PO BID initially; modify dose based on eGFR—used in combination with mycophenolate mofetil (MMF) and corticosteroids. Consider discontinuation if no therapeutic benefit by 24 weeks [36].
Table 2 shows the list of medication and their advised doses which are recommended for induction therapy (class III/IV) lupus nephritis.
-
Plasma exchange and immunoadsorption
Plasma exchange and immunoadsorption have little evidence in refractory LN. Patients with contraindications to traditional therapy, such as severe infection risk and substantial leucopenia, as well as additional indications including pulmonary hemorrhage, may benefit from extracorporeal therapies [37].
Figure 2 presented an algorithm for management of lupus nephritis.

Algorithm for management of lupus nephritis
Discussion
In SLE, an international panel of experts recently proposed the notion of “treat-to-target” (T2T), which is a therapeutic strategy aimed at improving illness outcomes by achieving predetermined treatment targets [38]. The T2T approach has been applied to a variety of chronic medical conditions, including diabetes and hypertension, as well as rheumatology, where the current therapeutic paradigm in rheumatoid arthritis (RA) focuses on disease remission to avoid long-term structural damage [39].
Unlike other SLE signs, LN is managed mostly through lab testing (primarily proteinuria, serum creatinine/eGFR, and erythrocyturia). Essentially, this would make the monitoring procedure for identifying the treatment goal in a T2T plan simple and fair, albeit problems remain. Complete renal remission, defined as normal or stable renal function, low proteinuria, and, in some studies, inactive urinary sediment [40, 41], is the ultimate goal of therapy. Proteinuria of 0.5 to 0.7 g per 24 h was found to be the strongest positive individual predictor of long-term renal outcomes, despite the lack of consensus on the ideal target level. This agrees with the results of published research which identified <0.7 g daily as the expected treatment target [42, 43]. Otherwise, the use of other clinical measures to distinguish between ongoing disease activity and renal damage in those patients with persistent urinary aberrations remains challenging without carrying out and assessing a renal biopsy [44, 45].
The present treatment approach for LN is composed of 2 steps: (1) Induction phase where rigorous management with immunosuppressive therapies in combination with glucocorticoids is advised aiming to minimize the likelihood of early damage of the kidney glomeruli and preserve the kidney functions on the long term. (2) Maintenance phase: which follows the induction phase and involves the continuation of immunosuppressive management. This phase aims at attaining a complete renal response and minimizing or preventing renal flares [46, 47]. Sequential immunosuppressive treatments, such as cyclophosphamide followed by azathioprine, or monotherapy, such as MMF, can be used in both the induction and maintenance stages. This two-phase technique has drawbacks, such as a lower likelihood of reaching total effectiveness and the possibility of medication-induced adverse effects, which are mostly associated to the administration of large dosages of glucocorticoids and their known role in long-term damage in SLE [48]. In line with previous research [49,50,51,52], this advice proposed using “multitarget” combination immunosuppressive therapy and lowering concomitant glucocorticoids dosage in a study to improve efficacy and reduce toxicity or both.
Safety concerns have been raised particularly for increased prevalence of infectious complications among LN patients [53]. These have been attributed to the limited current management options, the tight control management approach (T2T), and the use of aggressive/high-dose immunosuppressive therapy. This recommendation included a variety of recently approved therapies for LN. These novel biologic therapies are likely to boost the T2T approach to LN. Such approach would pave the way to develop and validate better complete renal remission assessment tools.
The study’s main strengths include the diversity and experience of the participants, the high levels of consensus attained, and conformity with the most recent publication recommendations. The PICO methodology technique, as well as the treat-to-target outcome, were chosen as the work’s main pillars.
Limitations of the guideline
Though the guideline reflects the best data available at the time the report was prepared, one of its limitations is the limited comparative evidence to inform selection of therapies. While these recommendations were developed using rigorous methodology, guidelines do have inherent limitations in informing individual patient care; hence the selection of the term “recommendations.” While they should not supplant clinical judgment or limit clinical judgment, they do provide expert advice to the practicing physician managing patients with lupus nephritis.
In conclusion, this evidence/consensus-based recommendation has endorsed an individualized treatment approach tailored to the patient’s predominant clinical manifestation and associated morbidity. The main objective is to help health care professionals as well as patients in making challenging disease management decisions and achieve remission of their lupus nephritis.
Availability of data and materials
The data will be available upon reasonable request.
Abbreviations
- ACE:
-
Angiotensin-converting enzyme
- aPL:
-
Anti-phospholipid antibodies
- ARB:
-
Angiotensin receptor blockers
- APRIL:
-
A proliferation-inducing ligand
- AZA:
-
Azathioprine
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- CNIs:
-
Calcineurin inhibitors
- CEBM:
-
Centre for Evidence-based Medicine
- CEG:
-
Consensus, Evidence-based, Guidelines
- CKD:
-
Chronic kidney disease
- CYC:
-
Cyclophosphamide
- CSA:
-
Cyclosporine A
- ESRD:
-
End-stage renal disease
- GFR:
-
Glomerular filtration rate
- GoR:
-
Grade of recommendation
- HCQ:
-
Hydroxychloroquine
- LN:
-
Lupus nephritis
- MMF:
-
Mycophenalate Mofetil
- PICOT:
-
Patient/Population, Intervention, Comparison, Outcomes and Time
- RCT:
-
Randomized control trial
- RTX:
-
Rituximab
- SC:
-
Subcutanous
- SLE:
-
Systemic lupus erythematosus
- TAC:
-
Tacrolimus
- T2T:
-
Treat to target
- WHO:
-
World Health Organization
References
Rahman P, Gladman DD, Urowitz MB, Hallett D, Tam LS (2001) Early damage as measured by the SLICC/ACR damage index is a predictor of mortality in systemic lupus erythematosus. Lupus 10(2):93–96
Nived O, Jonsen A, Bengtsson AA, Bengtsson C, Sturfelt G (2002) High predictive value of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for survival in systemic lupus erythematosus. J Rheumatol 29(7):1398–1400
Morales E, Galindo M, Trujillo H, Praga M (2021) Update on lupus nephritis: looking for a new vision. Nephron. 145(1):1–13
Bernatsky S, Boivin JF, Joseph L, Manzi S, Ginzler E, Gladman DD, Urowitz M, Fortin PR, Petri M, Barr S et al (2006) Mortality in systemic lupus erythematosus. Arthritis Rheum 54(8):2550–2557 [PubMed: 16868977]
Cervera R, Khamashta MA, Font J, Sebastiani GD, Gil A, Lavilla P, Mejia JC, Aydintug AO, Chwalinska-Sadowska H, de Ramon E et al (2003) Morbidity and mortality in systemic lupus erythematosus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000 patients. Medicine (Baltimore) 82(5):299–308
Wang H, Ren YL, Chang J, Gu L, Sun LYA (2018) systematic review and meta-analysis of prevalence of biopsy-proven lupus nephritis. Arch Rheumatol 33:17–25
Fanouriakis A, Bertsias G (2015) Treat-to-target in lupus: what does the future hold? Int J Clin Rheumatol 10(6):461–477
Bruce IN, O’Keeffe AG, Farewell V et al (2015) Factors associated with damage accrual in patients with systemic lupus erythematosus: results from the Systemic Lupus International Collaborating Clinics (SLICC) Inception Cohort. Ann Rheum Dis 74(9):1706–1713
van Vollenhoven RF, Mosca M, Bertsias G, Isenberg D, Kuhn A, Lerstrøm K et al (2014) Treat-to-target in systemic lupus erythematosus: recommendations from an international task force. Ann Rheum Dis 73(6):958–967
Tamirou F, Houssiau FA (2021) Management of lupus nephritis. J Clin Med 10(4):670
Ogdie A, Coates LC, Gladman DD (2020) Treatment guidelines in psoriatic arthritis. Rheumatology (Oxford) 59(Suppl 1):i37–i46
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med 151:W65–W94
Leclercq E, Leeflang MM, van Dalen EC, Kremer LC (2013) Validation of search filters for identifying pediatric studies. J Pediatr 162:629–634
OCEBM Levels of Evidence Working Group (2011) The Oxford levels of evidence 2. Oxford Centre for Evidence-Based Medicine, Oxford
Hsu CC, Sandford BA (2007) The Delphi technique: making sense of consensus. Pract Assess Res Eval 12:1–8
Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, Wales PW (2014) Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol 67(4):401–409
Von der Gracht H (2012) Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc 79(8):1525–1536
Hansen MP, BjerrumL G-HB, Jarbol DE (2010) Quality indicators for diagnosis and treatment of respiratory tract infections in general practice: a modified Delphi study. Scand J Public Health 28:4–11
Lai L, Flower A, Moore M, Lewith G (2015) Developing clinical practice guidelines for Chinese herbal treatment of polycystic ovary syndrome: a mixed-methods modified Delphi study complement. Ther Med 23(3):430–438
Hahn BH, Mcmahon MA, Wilkinson A, Wallace WD, Daikh DI, Fitzgerald JD, Grossman JM (2012) American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res 64(6):797–808
Weening JJ, D’A Gati VD, Schwart MM et al (2004) The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int 65:521–530
Kostopoulou M, Ugarte-Gil MF, Pons-Estel B, van Vollenhoven RF, Bertsias G (2022) The association between lupus serology and disease outcomes: a systematic literature review to inform the treat-to-target approach in systemic lupus erythematosus. Lupus 31(3):307–318. https://doi.org/10.1177/09612033221074580
Ingeborg BM et al (2018) Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int 93(4):789–796
Cozzani E, Drosera M, Gasparini G, Parodi A (2014) Serology of lupus erythematosus: correlation between immunopathological features and clinical aspects. Autoimmune Dis 2014:321359. https://doi.org/10.1155/2014/321359
Carter EE, Barr SG, Clarke AE (2016) The global burden of SLE: prevalence, health disparities and socioeconomic impact. Nat Rev Rheumatol 12(10):605–620
Giambalvo S, Garaffoni C, Silvagni E, Furini F, Rizzo R, Govoni M, Bortoluzzi A (2022) Factors associated with fertility abnormalities in women with systemic lupus erythematosus: a systematic review and meta-analysis. Autoimmun Rev 21(4):103038. https://doi.org/10.1016/j.autrev.2022.103038
Sherer Y et al (2004) Autoantibody explosion in systemic lupus erythematosus: more than 100 different antibodies found in SLE patients. Semin Arthritis Rheum 34(2):501–537 WB Saunders
Furie RA et al (2022) B-cell depletion with obinutuzumab for the treatment of proliferative lupus nephritis: a randomised, double-blind, placebo-controlled trial. Ann Rheum Dis 81(1):100–107
Mackay F, Schneider P (2009) Cracking the BAFF code. Nat Rev Immunol 9(7):491–502
Yo JH, Barbour TD, Nicholls K (2019) Management of refractory lupus nephritis: challenges and solutions. Open Access Rheumatol 11:179
Sahay M, Saivani Y, Ismal K, Vali PS (2018) Mycophenolate versus cyclophosphamide for lupus nephritis. Indian J Nephrol 28(1):35–40
Mok CC (2016) Con: cyclophosphamide for the treatment of lupus nephritis. Nephrol Dial Transplant 31(7):1053–1057
Almaani S, Rovin BH (2019) B-cell therapy in lupus nephritis: an overview. Nephrol Dial Transplant 34(1):22–29
Karasawa K, Uchida K, Takabe T, Moriyama T, Nitta K (2018) Recent advances in treatment strategies for lupus nephritis. Contrib Nephrol 195:42–50. https://doi.org/10.1159/000486933
Mok CC (2017) Calcineurin inhibitors in systemic lupus erythematosus. Best Pract Res Clin Rheumatol 31(3):429–438
Ponticelli C, Podestà MA (2021) Calcineurin inhibitors in lupus nephritis. J Nephrol 34(2):399–402
Kronbichler A et al (2016) Efficacy of plasma exchange and immunoadsorption in systemic lupus erythematosus and antiphospholipid syndrome: a systematic review. Autoimmun Rev 15(1):38–49
Parra Sánchez AR, Voskuyl AE, van Vollenhoven RF (2022) Treat-to-target in systemic lupus erythematosus: advancing towards its implementation. Nat Rev Rheumatol 18:146–157. https://doi.org/10.1038/s41584-021-00739-3
Smolen JS, Breedveld FC, Burmester GR et al (2015) Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum 75(1):3–15. https://doi.org/10.1136/annrheumdis-2015-207524
Davidson JE et al (2018) Renal remission status and longterm renal survival in patients with lupus nephritis: a retrospective cohort analysis. J Rheumatol 45:671–677
Dall’Era M et al (2015) Predictors of long- term renal outcome in lupus nephritis trials: lessons learned from the Euro-Lupus Nephritis cohort. Arthritis Rheum 67:1305–1313
Tamirou F et al (2015) A proteinuria cut- off level of 0.7 g/day after 12 months of treatment best predicts long-term renal outcome in lupus nephritis: data from the MAINTAIN Nephritis Trial. Lupus Sci Med 2(1):e000123. https://doi.org/10.1136/lupus-2015-000123
Ugolini-Lopes MR et al (2017) Early proteinuria response: a valid real-life situation predictor of long-term lupus renal outcome in an ethnically diverse group with severe biopsy-proven nephritis? Lupus Sci Med 4:e000213. https://doi.org/10.1136/lupus-2017-000213
Gunnarsson I et al (2007) Histopathologic and clinical outcome of rituximab treatment in patients with cyclophosphamide-resistant proliferative lupus nephritis. Arthritis Rheum 56:1263–1272
Sánchez ARP, Voskuyl AE, van Vollenhoven RF (2022) Treat-to-target in systemic lupus erythematosus: advancing towards its implementation. Nat Rev Rheumatol 3:146–157. https://doi.org/10.1038/s41584-021-00739-3
Furie R et al (2020) Op0164 BLISS- LN: a randomised, double- blind, placebo- controlled phase 3 trial of intravenous belimumab in patients with active lupus nephritis. Ann Rheum Dis 79:103–103
Merrill JT et al (2010) Efficacy and safety of rituximab in moderately- to-severely active systemic lupus erythematosus: the randomized, double- blind, phase II/III systemic lupus erythematosus evaluation of rituximab trial. Arthritis Rheum 62:222–233
van Vollenhoven R, Askanase AD, Bomback AS, Bruce IN, Carroll A, Dall'Era M et al (2022) Conceptual framework for defining disease modification in systemic lupus erythematosus: a call for formal criteria. Lupus Sci Med 9(1):e000634. https://doi.org/10.1136/lupus-2021-000634
Fanouriakis A et al (2020) 2019 Update of the Joint European League Against Rheumatism and European Renal Association- European Dialysis and Transplant Association (EULAR/ERA- EDTA) recommendations for the management of lupus nephritis. Ann Rheum Dis 79:713–723
Kostopoulou M, Adamichou C, Bertsias G (2020) An update on the diagnosis and management of lupus nephritis. Curr Rheumatol Rep 22:30
Zeher M et al (2011) Efficacy and safety of enteric-coated mycophenolate sodium in combination with two glucocorticoid regimens for the treatment of active lupus nephritis. Lupus 20:1484–1493
Condon MB et al (2013) Prospective observational single centre cohort study to evaluate the effectiveness of treating lupus nephritis with rituximab and mycophenolate mofetil but no oral steroids. Ann Rheum Dis 72:1280–1286
Lim C et al (2017) Severe infections in patients with lupus nephritis treated with immunosuppressants: a retrospective cohort study. Nephrology 22:478–484
Acknowledgements
Not applicable
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
Conceptualization and design: Yasser El Miedany, Mohammed Hassan Abu-Zaid, and Sally Saber; Acquisition of data: Yasser El Miedany and Mohammed Hassan Abu-Zaid; Formal analysis: Maha El Gaafary; Investigation: Ahmed Ezzat and Abeer Mokbel; Methodology: all authors; Writing—original draft: Yasser El Miedany, Mohammed Hassan Abu-Zaid, and Samar Tabra. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in accordance with the Helsinki Declaration. This was a multistep process which followed the “Clinical, Evidence-based, Guidelines” (CEG) initiative protocol (ethical approval code: 34842/8/21, ethical board Tanta University) aiming at setting up an actionable clinical gold standard for treat-to-target management of rheumatic and bone diseases. As per the Egyptian National Ethical Committee regulations, verbal informed consent was required from all the participants included in the study. All the participants included in the study gave their verbal informed consent. All the participants were kept anonymous, in compliance with data protection regulations.
Consent for publication
Not applicable
Competing interests
The authors declare that the corresponding author and Rehab Ali are associate editors in the Egyptian Rheumatology and Rehabilitation, and Mohammed Mortada and Yasser El Miedany are from the editorial board of the journal.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Miedany, Y., Kamel, N.S., Abu-Zaid, M.H. et al. Egyptian evidence-based consensus on clinical practice recommendations for the management of lupus nephritis. Egypt Rheumatol Rehabil 49, 48 (2022). https://doi.org/10.1186/s43166-022-00146-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-022-00146-w