
Abstract
Background
Because of the subjective character of symptoms, absence of a diagnostic test, modest response to treatments, and, at times, patient reports of important functional disability, fibromyalgia remains a challenge for the treating health care professionals in the standard clinical practice. The aim of this study was to develop an up-to-date consensus and evidence-based clinical practice guidelines for a treat-to-target management of fibromyalgia. Fifteen key clinical questions were identified by a scientific committee according to the Patient/Population, Intervention, Comparison, and Outcomes (PICO) approach. A literature review team performed a systematic review to summarize the evidence advocating the benefits and harms of available pharmacologic and nonpharmacologic therapies for fibromyalgia. Subsequently, recommendations were formulated. The level of evidence was determined for each section using the Oxford Centre for Evidence-based Medicine (CEBM) system. A 3-round Delphi process was conducted with 16 experts. All rounds were conducted online. A consensus was achieved on the direction and the strength of the recommendations.
Results
An online questionnaire was sent to an expert panel who participated in the three rounds (response rate 100%). At the end of round 3, a total of fifteen recommendation items, categorized into 10 sections to address the main fibromyalgia categories, were obtained. Agreement with the recommendations (ranks 7–9) ranged from 85 to 100%. Consensus was reached (i.e., ≥ 80% of respondents strongly agreed or agreed) on the wording of all the 15 clinical standards identified by the scientific committee. An algorithm for the management of fibromyalgia has been suggested.
Conclusions
These recommendations provide an updated consensus on both the non-pharmacological and the pharmacological treatments of fibromyalgia. The provided strategies to reach optimal treat-to-target outcomes in common clinical scenarios are based on a combination of evidence and expert opinions. Best treatment decisions should be tailored to each individual patient situation.
Similar content being viewed by others


Key points
-
Fibromyalgia is a challenging disease, with no specific diagnostic tests identified.
-
Fibromyalgia treat-to-target management approach should be tailored to the main manifestations of fibromyalgia including pain, function, associated features (e.g., depression), sleep difficulty, fatigue, and associated comorbidities.
Background
Fibromyalgia (FM) is a chronic disabling musculoskeletal condition of unknown etiology characterized by generalized musculoskeletal pain, extreme fatigue, mood disturbance, impaired cognition, and lack of refreshing sleep [1]. As long as pain is the dominant symptom in FM, it has an extensive negative impact on the patient’s physical as well as psychological status. Several patients have been identified as physically disabled with great impaired quality of life [2]. FM can be either primary (identified as idiopathic FM) or secondary if it occurred in association with other diseases. The pathophysiology of FM remains unclearly understood although aberration in processing of pain at several levels (both peripheral and central), impairment of sleep, dysregulation of the hypothalamo–pituitary–adrenal axis, and dysfunction of the autonomic nervous system have been recognized as contributing factors [3].
The onset of FM occurs mainly in the middle age; however, FM in children is not uncommon. The estimated prevalence of FM worldwide is 0.5 to 5.8% in North America and Europe [4]. In Egypt, the prevalence of FM was assessed in cohorts of patients with concomitant illnesses. The higher prevalence was reported in rheumatoid arthritis and SLE patients at 21% [5,6,7] and 18% [8], respectively, whereas 6.7% in systemic sclerosis, while it was less commonly prevalent at 3.3% in Behcet’s disease patients [9] and 1.9% in patients with chronic liver disease [10].
There are no specific diagnostic tests identified for FM. Diagnosis is usually considered after the exclusion of other disorders whether psychological such as depression, musculoskeletal, or neurological. This lack of a solely uniting pathophysiology is mirrored by a non-specific and complex management approach. Every year, new data is published on the disease epidemiology, pathogenesis, genetic, and management approach. Evidence-based guidelines aim to guide health care providers and patients in the choice of treatment options. In spite of several treatment recommendations and guidelines published [11,12,13], there is still a debate regarding the treatment options and first choice of therapy for FM. As Egypt has launched a nationwide universal health coverage in 2020, setting up guidelines for the management of patients is vital to the process. The overarching objective of this work was to develop an up-to-date consensus and evidence-based clinical practice guidelines for a treat-to-target management of FM. This would be of value not only for health care professionals managing musculoskeletal conditions, but also for regulatory bodies, health-related organizations, and interested patients’ groups/laypersons. This project was carried out under the Consensus, Evidence-based, Guidelines (CEG) initiative setup in Egypt which aims at promoting evidence-based practice in rheumatology by developing treat-to-target clinical practice guidelines addressing relevant clinical problems.
Methods
Design
The CEG for fibromyalgia were developed adopting a multistep process strategy. The study design was formulated based on the CEG guideline development process protocol which involves a scientific evidence and consensus, based on the existing scientific evidence and clinical experience. The manuscript conformed to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for reporting systematic reviews [14].
Development stages
Core team
This was formed of four experts with recognized experience in FM management. The core team coordinated and supervised the teamwork; assisted with developing the scope of the project and initial Patient/Population, Intervention, Comparison, and Outcomes (PICO) clinical questions; and reached a consensus on the key questions to include in the guidelines. For each PICO question, the core team pre-identified the outcomes as critical for the systematic literature review. The team also nominated the expert panel and drafted the manuscript.
Key questions used to develop the guideline
This guideline was centered on a series of structured key questions that define the target population, the intervention, investigation, the comparison(s) used, and the outcomes used to measure efficacy, effectiveness, or risk. The evidence to answer the clinical questions was collected according to the following steps: formulation of clinical questions, structuring of questions, search for evidence, critical evaluation and selection of evidence, presentation of results, and recommendations. These questions, shown in Table 1, formed the basis of the systematic literature search and consequently the clinical care standards. Evidence-based recommendations for the diagnosis and investigation of FM have not been included in this guideline.
Literature review team
Led by an experienced literature review consultant and based on the specific research questions identified to focus on the management of FM, the literature review was conducted with the assistance of an expert in methodology. To acquire proper evidence-based background knowledge for consideration, a systematic literature search was carried out using PubMed/MEDLINE, EMBASE, and Cochrane databases. Following the data abstraction, reviewing the published recommendations, the quality of evidence rating [15, 16], revision was carried out by the experts responsible for the literature review, who provided a comprehensive list of propositions for the management of FM based on available research evidence and their own clinical expertise. The level of evidence was determined for each section using the Oxford Centre for Evidence-based Medicine (CEBM) system [16].
Data sources and search strategies
The search strategy was planned to capture all studies in which the study population was adults living with FM arthritis. The PICO questions (Table 1) were used to conduct the literature search. Literature search strategies were carried out to locate randomized clinical trials evaluating the efficacy of FM management as well as quality improvement outcomes/approaches. The search terms were related to FM, myofascial pain, and fibrositis. No specific term related to “therapies” was used to increase the sensitivity of our search and avoid exclusions of possible relevant therapies of which we were not aware. Trials comparing these therapies with a control group were included. Two outcomes were identified: pain and QOL measured with the FM Impact Questionnaire (FIQ) [17]. This choice was based on pain being the most characteristic symptom of FM [18] and the FIQ being an instrument that captures other commonly reported symptoms in this population (i.e., fatigue, stiffness, anxiety, and depression). For pain, data was analyzed if rated using the visual analog scale (VAS), or when the VAS was not available, Numerical Rating Scales (NRSs) or other valid instruments were used.
Keywords used were dependent on the PICO elements used in different combinations. Literature searches on 14 September 2021 for PubMed and Cochrane Library databases and on 28 September 2021 for Embase. The search was updated on 25 October 2021. Duplicate screening of literature search results was performed electronically. Additional relevant studies were retrieved by reviewing the reference lists of studies identified with the database search strategies that met the inclusion criteria.
Study selection
Relevant studies were selected by applying the inclusion and exclusion criteria to the literature retrieved with the search strategies
Inclusion criteria
Articles included were systematic reviews, randomized controlled trials (RCTs), uncontrolled trials, observational studies including cohort, case-control, and cross-sectional studies, or those where economic evaluation was made. Trials were eligible if they included people with FM regardless of age or sex, from any health care setting receiving any therapy. The included studies should have the criteria of classification evidence and recommendations used identified. Also, the formal process for establishing recommendations (Delphi exercise, panel conference) is outlined.
Exclusion criteria
Editorials, commentaries, conference abstracts and non-evidence-based narrative/personal reviews, and manuscripts lacking of English version were excluded. Trials investigating surgical therapies were not considered in our review because these are rarely offered for the management of FM.
Ethical aspects
This study was performed in accordance with the Helsinki Declaration. The “Clinical, Evidence-based, Guidelines” (CEG) initiative protocol was approved by the local ethical committee: ethical approval code: 34842/8/21, ethical board Tanta University. Written ethics approval from the experts sharing in this work was deemed unnecessary according to national regulations. As per the Egyptian national Ethical Committee regulations, verbal informed consent was required from all the participants included in the study. All the participants were kept anonymous, in compliance with data protection regulations.
Expert panel
The core leadership team nominated 16 participants. The criteria for their selection included have professional knowledge and experience (at least 8 years of experience) in the field of rheumatology, management of inflammatory arthritis, and in particular FM as well as active participation in scientific research on rheumatic diseases. The expert panel assisted with developing the scope of the project and refining the PICO questions. PICO questions were drafted into recommendation statements and were sent to the expert panel with the evidence report who voted on the recommendations.
Target audience
The guideline has been developed to provide assistance to healthcare professionals who treat and manage patients with FM. The guideline should also provide a helpful resource for patients and those responsible for commissioning care for patients with FM in the National Health Service
Developing the clinical care standards framework
Based on the answers to the structured key questions and the literature review, a structured template was developed to facilitate standardized identification of guideline components. For each guideline component, the format in which the recommendations/information will be provided and extracted has been identified.
Delphi process
The Delphi technique [19] is a structured method widely used to gather important information on a specific topic. It relies on the key assumption that projections from a group are generally more accurate than those from individuals. Therefore, the aim of the Delphi method is to construct consensus forecasts from a group of experts in a structured iterative manner. Its methodology is based on a series of questionnaires or “rounds” addressed to experts. The Delphi method generally involves the following stages: (1) a panel of experts is assembled; (2) forecasting tasks/challenges are set and distributed to the experts; (3) experts return initial forecasts and justifications. These are compiled and summarized in order to provide feedback; (4) feedback is provided to the experts, who reviewed their forecasts considering the feedback. This step may be iterated until a satisfactory level of consensus is reached; and (5) final forecasts are constructed by aggregating the experts’ forecasts. The key features of this method are the anonymity of participants and the controlled feedback [19,20,21].
Consensus process
Three Delphi rounds were carried out to establish consensus regarding the T2T (treat-to-target) strategy in FM. The structured Delphi approach ensures that the opinions of participants are equally considered. The Delphi process was conducted through online questionnaires. The first round of the electronic questionnaire included 11 items involved in the T2T strategy of FM.
Voting process
Live online delivered voting was carried out in three rounds that were strictly time-limited. All members of the task force were invited to participate and were pre-informed of the time of opening and closure of each round of votes. Unique access links were sent out, and anonymous votes were gathered and processed. Comments on re-phrasing, potential ambiguity, and unidentified overlaps were gathered regarding each statement at the same time in the voting process. Only the members of the task force had the right to vote on the statements.
Rating
Each statement was rated between 1 and 9 with 1 indicative of “complete disagreement” and 9 indicating “complete agreement.” Generally, 1–3, 4–6, and 7–9 represent disagreement, uncertainty, and agreement, respectively. Voting on all statements was not mandatory, and the members were encouraged to refrain if they feel that a statement falls outside their area of expertise. An “uncertainty” vote represents “inconvenience about the accuracy of the recommendation.” All statements were allowed for the entry of comments which were reviewed by the scientific committee after each round of voting. In all the votes’ rounds, particularly wherever they vote a disagreement, the members were urged to leave comments. This enabled the panel to identify an instance of misinterpretation of statement and invalidate the vote on that statement.
Definition of consensus
Definition of consensus was established before data analyses. It was determined that consensus, consequently, to become a recommendation in this guideline, would be achieved if at least 80% of participants reached agreement (scores 7–9) or disagreement (scores 1–3) [19,20,21]. A statement was retired if it had a mean vote below 3 or a “low” level of agreement. Statements whose rate came in the uncertainty score (4–6) were revised in view of the comments. The levels of agreement on each statement of recommendation were defined as “high” if after the second round of votes all votes on a statement fell into the agreement bracket (7–9) [21,22,23].
Chronogram of Delphi rounds
The first round took place between 20 and 24 November 2021 (4 days). The aspects about which respondents did not reach consensus in this first round were revised in view of the comments and included in the second round. The second round lasted for 4 days (till 3 December 2021). Lastly, the comments raised by the panel members in the second round were all revised in the third round which was from 24 to 28 December 2021.
Results
Literature research and evidence selection
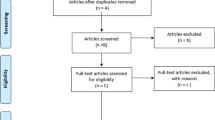
In the study selection process, we found 2119 potentially relevant studies by search strategy. A total of 1871 were excluded: 326 duplicates and 2545 by screening of title and abstracts (studies did not examine population or intervention of interest, did not match study design of interest, or did not report outcome measures of interest). Therefore, 248 relevant studies were included for a full article review. A total of 225 studies were excluded as citations did not provide evidence matching a PICO; consequently, 23 studies were included in this work (Fig. 1).

Treat-to-target algorithm for fibromyalgia patients. CBC, complete blood count; TSH, thyroid-stimulating hormone; CK, creatine kinase; CRP, C-reactive protein; CBT, cognitive–behavioral therapy; SNRI, serotonin and norepinephrine reuptake inhibitor
Expert panel characteristics
The Delphi form was sent to expert panel (n = 16), of whom 14 (93.3%) completed in the two rounds. The respondents were drawn from different governorates and health centers across Egypt: Ain Shams University (n = 4, 28.6 %), Cairo University (n = 1, 7.1%), Tanta University (n = 2, 14.3%), Benha University (n = 1, 7.1%), Alexandria University (n = 1, 7.1%), Fayoum University (n = 1, 7.1%), Zagazig University (n = 2, 14.3%), and Assiut University (n = 1, 7.1%), in addition to (n = 1, 7.1%) international expert from UK. All the experts’ panel (100%) were rheumatologists.
Delphi round 1
The key clinical question comprised of 14 questions stratified under 9 domains (Table 1) including targeted patients, treatment target, diagnosis, investigations, patient’s evaluation, treatment, comorbidity, outcomes, and monitoring. Each domain entails one or more elements. In this round, the participants were asked to rate the overall principles considered in the decision-making for T2T management of FM. The response rate for round 1 was 87.5% from the experts’ panel (14/16). Consensus was reached on the domains (as ≥ 80% of respondents strongly agreed or agreed), and only one question was added about self-management; otherwise, all the suggested questions were accepted by the panel and no questions were retired.
Delphi round 2
Considering the input from round 1, a list of 10 domains involving 15 proposed recommendations was developed based on the review of the literature, 1 for targeted patients and 1 for the treatment target, 2 for the diagnosis, 1 for the investigations, and 1 for patient’s evaluation, while 5 for the treatment, 1 related to treatment of FM as a comorbidity, 1 for the outcomes, and at last 1 for the self-management. The response rate for round 2 was 100% from the experts’ panel (14/14). Modifications were suggested for 4 statements (1 in the investigations, 2 in the treatment, and 1 in the outcomes). The statements were modified and amended. For the rest of the statements, the consensus was reached (as ≥ 80% of respondents strongly agreed or agreed).
Delphi round 3
Based on the input from round 2, the experts were presented with modified 4 statements. The response rate for round 3 was 100% (14/14). The core team reviewed the statements, and the frequency of the strongly agreed recommendation (ranks 7–9) ranged from 80 to 100%. The experts were comfortable with the final list of the statements and with the Delphi process overall (Table 2).
Table 3 also shows the level of evidence assigned to each statement, in accordance with the Oxford Centre for Evidence-Based Medicine (CEBM) criteria as well as mean ± standard deviation and level of agreement.
Discussion
FM is a recognized medical condition, with ACR-defined preliminary criteria and revised 2016 criteria as well as severity scales [25,26,27]. It is characterized by generalized body pain and associated core symptoms of fatigue, sleep disturbance, and significant negative impact on both physical and psychological well-being. Although it remains unclear, FM pathogenesis is mainly linked to disorders in the nervous system rather than a musculoskeletal disease, as the nomenclature of “FM” infers [28]. FM may occur as a primary diagnosis, but the association with other somatic and mental disorders broadens the concept as well as the impact of this disorder [29].
This study aimed at answering the difficult question of “Can a treat-to-target strategy for FM be adopted?”. The work proposed an evidence-based algorithm, developed and agreed upon by a consensus of experts. The results identified pain and physical and psychological well-being as the treatment targets. Self-reported patient-reported outcome measure [30] has been identified as a composite measure with threshold values scored using a numerical scale. This agrees with the outcomes of the study carried out by Hauser et al. [31] which revealed that the self-reported Patient Health Questionnaire 15 (PHQ 15) can be used as a measure of overall severity in FM.
The results of this work endorsed the concept that FM treat-to-target management approach should be tailored to the main manifestations of FM including pain, function, associated features (e.g., depression), sleep difficulty, fatigue, and associated comorbidities. Medical treatment should also be targeted at balancing benefit and risk of the medical therapy, improving health-related quality of life, and maintaining physical activity. Often, this is achieved by adopting a multidisciplinary approach with a mix of treatment modalities as well as non-/pharmacological modalities. This strategy agrees with the management recommendations endorsed by both the EULAR [11] as well as the Canadian Pain Society and the Canadian Rheumatology Association [24].
The main challenge in FM management is to set up a management plan that would be implemented by the patient. The results of this work endorsed the concept that while the management approach to FM starts with a diagnosis, its core is based on shared decision-making, self-management, and motivation approach as well as exercise program or at least remain active. Such multifaceted treatment strategy reflects the changes in the FM model of care which took place over the past decade. This work has been set up to address the new concepts in the management of this illness. FM should no longer be a conundrum but rather recognized as a valid disorder with treatment strategies that are aimed to reduce symptoms and maintain function. This agrees with the outcome of Wolfe et al. [26] work, which revealed that a combination of physician and questionnaire criteria, minimizes misclassification of regional pain disorders, and eliminates the previously confusing recommendation regarding diagnostic exclusions. Also, it agrees with the management strategy recommended by the EULAR [11] and the Canadian Pain Society and Canadian Rheumatology Association [24].
To optimize treatment outcomes for FM patients, particularly after a lack of response to initial nonpharmacological therapy, this guideline endorsed the use of combination therapy for this cohort of non-responsive patients. Combination therapy may include non-pharmacologic and pharmacologic therapies or be a combination of two medical therapies. This is in agreement with the outcomes of a meta-analysis of 16 studies that used various two-drug combinations for the treatment of FM pain. The meta-analysis reported that three combinations (melatonin-amitriptyline, fluoxetine-amitriptyline, and pregabalin-duloxetine) produced a greater reduction in pain compared with monotherapy alone [32]. This also agrees with the outcome of another report which revealed that patients who exhibit polygenic chronic illnesses may be treated with combinations of medications based on their different mechanisms of action [29]. Education and active participation with reassurance to FM patients have a great influence as a self-management that will facilitate the practice of a health-promoting lifestyle. This was stated in the metanalysis which concluded that self-management interventions can be effective in improving physical function and reducing pain in fibromyalgia [33].
The main strengths of the study are related to the diversity as well as the expertise of the participants, the high levels of consensus achieved, and the agreement with the most recently published recommendations. Also, the adoption of the PICO methodology approach as well as the treat-to-target outcome as the main pillars of this work.
Limitations of the guideline
Though the guideline reflects the best data available at the time the report was prepared, one of its limitations is the limited comparative evidence to inform the selection of therapies. This incorporates the primary comparative benefit/efficacy and harms evidence. In view of the absence of head-to-head comparative studies identified in the literature review, indirect comparisons among trials/therapies were used for the purpose of this work. Caution should be exercised in interpreting the data; the results of future studies may require alteration of the conclusions or recommendations in this report. It may be necessary or even desirable to depart from the guidelines in the interests of specific patients and special circumstances. Just as adherence to guidelines may not constitute a defense against a claim of negligence, so deviation from them should not necessarily be deemed negligent.
Conclusion
In conclusion, FM is one of the most common chronic pain disorders which has been attributed to abnormal pain processing. Being a complex and heterogeneous illness, a full understanding of FM necessitates comprehensive assessment of pain, functional ability, and quality of life, as well as psychosocial context. The goals of management should be to lessen the severity of symptoms and to improve health-related quality of life. This guideline endorsed a management strategy tailored to the individual patient’s condition with a mix of treatment modalities as well as non-/pharmacological modalities. Patients who are fully informed about their condition and the available treatment options can take charge and learn to live with FM the best way possible.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Change history
20 June 2022
A Correction to this paper has been published: https://doi.org/10.1186/s43166-022-00137-x
Abbreviations
- PICO:
-
Population, Intervention, Comparator, and Outcomes
- CEBM:
-
Centre for Evidence-based Medicine
- T2T:
-
Treat-to-target
- CEG:
-
Consensus, Evidence-based, Guidelines
- FM:
-
Fibromyalgia
- RCTs:
-
Randomized controlled trials
- NRSs:
-
Numerical Rating Scales
- ACR:
-
American College of Rheumatology
References
Bazzichi L, Giacomelli C, Consensi A et al (2016) One year in review: fibromyalgia. Clin. Exp. Rheumatol. 34:S145–S149
Annemans L, Lay K, Le J, Taïeb C (2009) Societal and patient burden of fibromyalgia syndrome. Pharmacoeconomics 27:547–559
Kia S, Choy E (2017) Update on treatment guideline in fibromyalgia syndrome with focus on pharmacology. Biomedicines. 5(2):20
Gran JT (2003) The epidemiology of chronic generalized musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 17:547–561
El-Tokhy H, Attia F, Mousa S, Kotb H, Attia H (2014) Fibromyalgia in Egyptian rheumatoid arthritis patients and patients with depression. Egypt J Rheumatol Clin Immunol 2(1):97–103
Gheita TA, Sayed S, Gheita HA, Kenawy SA (2016) Vitamin D status in rheumatoid arthritis patients: relation to clinical manifestations, disease activity, quality of life and fibromyalgia syndrome. Int J Rheum Dis 19(3):294–299
Ragab O, Khairy N, Taha R, Iskander M (2018) Serum serotonin in rheumatoid arthritis patients: relation to rheumatoid factor positivity, clinical manifestations and fibromyalgia Egypt. Rheumatol 40(3):149–153
El-Rabbat SM, Mahmoud NK, Gheita TA (2018) Clinical significance of fibromyalgia syndrome in different rheumatic diseases: relation to disease activity and quality of life. Reumatol Clín 14(5):285–289
Gheita TA, Eesa NN (2019) Rheumatology in Egypt: back to the future. Rheumatol Int. 39(1):1–12
Mohammed RHA, ElMakhzangy HI, Gamal A, Mekky F, El Kassas M, Mohammed N et al (2010) Prevalence of rheumatologic manifestations of chronic hepatitis C virus infection among Egyptians. Clin Rheumatol 29(12):1373–1380
Macfarlane GJ, Kronisch C, Dean LE et al (2017) EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis. 76(2):318–328
Fitzcharles MA, Ste-Marie PA, Pereira JX (2013) Canadian Fibromyalgia Guidelines Committee. Fibromyalgia: evolving concepts over the past 2 decades. CMAJ. 185(13):E645–E651
Häuser W, Thieme K, Turk DC (2010) Guidelines on the management of fibromyalgia syndrome - a systematic review. Eur J Pain. 14(1):5–10
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med 151:W65–W94
Leclercq E, Leeflang MM, van Dalen EC, Kremer LC (2013) Validation of search filters for identifying pediatric studies. J Pediatr 162:629–634
OCEBM Levels of Evidence Working Group (2011) The Oxford levels of evidence 2. Oxford Centre for Evidence-Based Medicine, Oxford
Burckhardt CS, Clark SR, Bennett RM (1991) The Fibromyalgia Impact Questionnaire: development and validation. J Rheumatol. 18(5):728–733
Wolfe F, Smythe HA, Yunus MB et al (1990) The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the Multicenter Criteria Committee. Arthritis Rheum. 33(2):160–172
Hsu CC, Sandford BA (2007) The Delphi technique: making sense of consensus. Practical assess. Res Eval 12:1–8
Diamond IR, Grant RC, Feldman BM et al (2014) Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol 67(4):401–409
Von der Gracht H (2012) Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc 79(8):1525–1536
Hansen MP, BjerrumL G-HB, Jarbol DE (2010) Quality indicators for diagnosis and treatment of respiratory tract infections in general practice: a modified Delphi study. Scand J Public Health 28:4–11
Lai L, Flower A, Moore M, Lewith G (2015) Developing clinical practice guidelines for Chinese herbal treatment of polycystic ovary syndrome: a mixed-methods modified Delphi study complement. Ther Med 23(3):430–438
Fitzcharles MA, Ste-Marie PA, Goldenberg DL et al (2013 Aug) Canadian Pain Society and Canadian Rheumatology Association recommendations for rational care of persons with fibromyalgia: a summary report. J Rheumatol. 40(8):1388–1393
Wolfe F, Clauw DJ, Fitzcharles MA et al (2010) The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken) 62:600–610
Wolfe F, Clauw DJ, Fitzcharles MA et al (2016) 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 46(3):319–329
Wolfe F, Clauw DJ, Fitzcharles MA et al (2011) Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR preliminary diagnostic criteria for fibromyalgia. J Rheumatol 38:1113–1122
Hauser W, Ablin J, Fitzcharles MA et al (2015) Fibromyalgia. Nat Rev Dis Primers 1:15022
Clauw DJ (2014) Fibromyalgia: a clinical review. JAMA 311:1547–1555
El Miedany Y, El Gaafary M, Youssef S, Ahmed I (2016) Towards tailored patient’s management approach: integrating the modified 2010 ACR Criteria for Fibromyalgia in Multidimensional Patient Reported Outcome Measures Questionnaire. Arthritis. 2016:5371682
Hauser W, Brahler E, Wolfe F, Henningsen P (2014) Patient Health Questionnaire 15 as a generic measure of severity in fibromyalgia syndrome: surveys with patients of three different settings. J Psychosom Res 76:307–311
Thorpe J, Shum B, Moore RA et al (2018) Combination pharmacotherapy for the treatment of fibromyalgia in adults. Cochrane Database Syst Rev. 2(2):CD010585
Geraghty AWA, Maund E, Newell D et al (2021) Self-management for chronic widespread pain including fibromyalgia: a systematic review and meta-analysis. PLoS One. 16(7):e0254642. https://doi.org/10.1371/journal.pone.0254642 PMID: 34270606; PMCID: PMC8284796
Acknowledgements
The authors would like to thank all contributors to this work especially Dr. Yasser El Miedany and Dr. Salwa Galal for their hard work in this study.
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Dr. Yasser El Miedany, Naglaa Gadallah, Diaa Mohasseb, Nahla M. Gaballah, Abeer K. El Zohiery, Mohammed Hassan, Maha El Gaafary, Waleed Hassan, Mohamed Mortada, Mervat Eissa, Samar Abdelhamed Tabra, Nermeen Foad, Fatma H El Nouby, Sally Saber, and Salwa Galal. The first draft of the manuscript was written by Dr. Salwa Galal and Dr. Yasser El Miedany. All authors commented on the previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in accordance with the Helsinki Declaration. The “Clinical, Evidence-based, Guidelines” (CEG) initiative protocol was approved by the local ethical committee: ethical approval code: 34842/8/21, ethical board Tanta University.
Consent for publication
Not applicable
Competing interests
The authors declare that the corresponding author Dr. Salwa Galal, and the co-author Dr. Mohammed Hassan, are associate editors in the Egyptian Rheumatology and Rehabilitation. Co-authors Dr. Yasser El Miedany, Dr. Diaa Mohasseb, Dr. Abeer El Zohiery, Dr. Waleed Hassan and Dr. Mohamed Mortada, are members of the editorial board of the journal.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised to update the "Competing interests" section.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Miedany, Y., Gadallah, N., Mohasseb, D. et al. Consensus evidence-based clinical practice recommendations for the management of fibromyalgia. Egypt Rheumatol Rehabil 49, 30 (2022). https://doi.org/10.1186/s43166-022-00129-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-022-00129-x