
Abstract
Background
Multiple sclerosis (MS) is a persistent inflammatory condition affecting the central nervous system, often associated with cognitive impairment. This impairment frequently presents itself as deficiencies in short-term memory, attention, and information processing speed. This research was designed to investigate P300 in patients with MS and its correlation with their cognitive function and their state of fatigue and depression. This work included two groups: the control group (20 subjects) and the study group (30 MS patients). Evaluation encompassed clinical history, audiological assessment, the Expanded Disability Status Scale (EDSS), the fatigue severity scale, the Beck Depression Inventory, Addenbrooke’s cognitive examination, and P300 component of event-related potentials (ERPs).
Results
The study group exhibited varying degrees of fatigue and depression. The scores of Addenbrooke’s cognitive evaluation were reduced in the MS group. The MS group exhibited a considerably prolonged P300 latency compared to the control group.
Conclusion
This study demonstrates the effectiveness of P300 in assessing cognitive function in persons diagnosed with MS.
Similar content being viewed by others


Background
Multiple sclerosis (MS) is a persistent inflammatory disease that affects the central nervous system (CNS) and causes harm to both white and gray matter [1]. It is characterized by demyelination, which is followed by degeneration. This results in damage to neurons and loss of axons. Approximately 45–70% of individuals with MS encounter cognitive dysfunction, with the majority of cases exhibiting impaired information processing, memory deficits, and learning difficulties [2].
Event-related potentials (ERPs) are types of auditory evoked potentials (AEPs) used for studying the processing of information and the cognitive functions of the brain such as attention, learning, and memory [3]. The P300 is a component of the ERPs that appears as a positive deflection occurring approximately 300 ms after the stimulus. It has been linked to cognitive processes such as memory, attention, focus, and the mental processing speed [4].
P300 has been used for evaluating the central information processing during the course of various neurological diseases including MS, due to its easy recording and reliability [5]. P300 abnormalities have been described in MS patients and are thought to be associated with impaired cognition, including executive functions, working memory, attention, and information processing [6]. Previous researchers [7,8,9] have reported abnormal P300 latency and amplitude in those patients but little research was done to correlate P300 findings with neuropsychological tests such as Addenbrooke’s cognitive examination. Moreover, few studies were done to find a correlation between P300 results and MRI findings which will be addressed in this work. MS patients suffered several degrees of fatigability and depression which have a great impact on MS patients’ cognitive functions; however, they did not receive enough attention. So, this work was designed to study the status of the cognitive function in MS patients using P300 and correlate it with their fatigue or depression statuses.
Methods
This study was done at the Audiovestibular Unit and Neurology Department of Kafrelsheikh University Hospital. A total of 50 individuals were selected to take part in the study, and they were separated into two groups: the control group, consisting of 20 volunteers who had no previous neurologic or psychiatric disorders, and the study group, which comprised 30 patients diagnosed with multiple sclerosis. Both groups were carefully selected to have participants within the age range of 18 to 45 years, with an equal distribution of males and females, and similar levels of education. The duration of this study was from May 2021 to November 2022.
The 2017 revised McDonald criteria for MS patients with clinically definite illness were incorporated in the study group’s inclusion criteria [10]. In terms of the exclusion criteria, it specifically eliminated individuals with MS who were experiencing a relapse or had received steroids within 1 month prior to the assessment. Additionally, patients with severe motor disability or functional disability were also excluded. The following cases were excluded from both groups: cases with any level of hearing loss or visual impairment; cases with known disorders that impact the cognitive functions; cases with psychiatric illness; or cases using anticholinergic, antiepileptic, tranquillizers, or antidepressant drugs.
The study group was evaluated as following:
-
Complete history taking, complete general and full neurological examination.
-
Assessment of disability using the Expanded Disability Status Scale (EDSS), which evaluates disability scores in eight functional systems (FS): pyramidal, cerebellar, brain stem, sensory, visual, bowel/bladder, mental, and ambulation. This rating scores range from 0 (representing normal neurological status) to 10 (representing mortality caused by MS) with increments of 0.5 at each interval [11].
-
Assessment of fatigue and its effect on a person’s activities and lifestyle using the 9-item fatigue severity scale [12].
-
Assessment of depression using the Beck Depression Inventory scale which is a composed of 21-question multiple-choice self-report assessment [13].
-
Radiological investigation: Magnetic resonance imaging (MRI) of brain and/or spinal cord using T2, pregadolinium and postgadolinium (Gd), enhancing T1 images were done as a part of their MS diagnosis to assess:
Both groups were subjected to:
-
Assessment of cognition using the Arabic version of Addenbrooke’s cognitive examination, which consists of 19 activities that are categorized into five cognitive domains: attention, memory, fluency, language, and visuospatial abilities [15].
-
Basic audiological evaluation.
-
P300 component of event-related potentials.
P300 was measured in response to auditory stimulation with tones of 1000 Hz and 2000 Hz. The oddball paradigm was used, where the 1000 Hz tone was provided more frequently (85% of the time) and the 2000 Hz tone was presented less frequently (15% of the time). Both tones were delivered by insert phones at 70 dBSPL, with a rise and fall period of 10 ms, 30 ms duration, and a repetition rate of 0.6 per second. The recording time frame spanned from − 50 to 500 ms. The gain factor was × 50,000 and the band-pass filter was set at 1–30 Hz.
P300 was recorded using Ag/AgCl surface electrodes placed at Fz (upper forehead) as the active electrode, Fpz (lower forehead) as the ground electrode, and the mastoids as reference electrodes depending on the side of stimulation. The skin was properly cleaned by gauze soaked with alcohol and scrubbing gel to keep the impedances at a value of 5 kΩ or below. The recording took place in a quiet room, where participants were given instructions to mentally keep track of all “target” tones. The P300 was recognized as the most prominent positive peak that appeared within the time frame of 250–450 ms after the presentation of the stimulus. Both latency (time taken between stimulus presentation and the appearance of the positive peak of P300) and peak-to-peak amplitude were calculated.
The statistical analysis was conducted using the SPSS software, specifically version 26 (IBM SPSS Statistics for Windows version 26.0; Armonk, NY: IBM Corporation). Both the Kolmogorov–Smirnov test, which assesses the distribution type, and the Levene test, which examines the homogeneity of variances, were employed to confirm the assumptions required for conducting parametric testing. The Student t-test was employed to compare quantitative variables between the two groups when the data was regularly distributed. On the other hand, the Mann–Whitney test was used for comparing quantitative variables when the data was discrete and not normally distributed. The Spearman rank correlation coefficient was employed to evaluate the correlation between two continuous variables that exhibit non-normal distribution.
Results
Both groups exhibited no statistically significant disparity in terms of age (32.45 ± 7.49 years and 30.23 ± 8.78 years for the control and study groups, respectively), gender, education, or marital status. In the study group, the occurrence of MS was more common among females, with a female to male ratio of 2.3:1.
The analysis of the study group (MSG) showed that 56.7% of patients (13 cases) had relapsing–remitting MS (RRMS), 23.3% of cases (7 cases) had secondary progressive MS (SPMS), and 20% of cases (6 cases) had primary progressive MS (PPMS). In addition, 46.7% of the cases had signs of disease activity through the presence of enhanced lesions in T2 MRI scans. Table 1 presents the disease features of MS patients.
In the study group, the Expanded Disability Status Scale (EDSS) revealed a mean score of 3.38, which indicates a moderate level of disability. The disease’s progression was assessed using the progression index (PI) and yielded a score of 1.28, indicating a favorable prognostic value. In addition, the multiple sclerosis severity scale (MSSS) demonstrated a score of 5.98, which signifies a moderate level of severity (Table 1).
In addition, the study group showed that all participants exhibited varying degrees of depression and fatigue as shown by the Beck Depression Inventory (BDI) and fatigue severity scales (FSS) (Table 2).
Results of Addenbrooke’s cognitive examination revealed that both the total score and the scores of its five domains (attention, memory, fluency, language, and visuospatial) were considerably lower in the MS group (Table 3; Fig. 1).

Multiple bar chart showing comparison between the control and MS groups regarding Addenbrooke’s total score and its domains
P300 was absent in five patients with MS (bilateral absence in four cases and right absence in one case). The remaining cases had a substantial delay in P300 latency compared to the control group. Nevertheless, the P300 amplitude did not exhibit any noteworthy disparity (p > 0.05) (Table 4).
There was non-significant correlation between the P300 (both latency and amplitude) and the age of onset, disease duration, number of relapses in the last 2 years, total relapse count, and disease severity (as indicated by PI, EDSS, and MSSS) in the MS patients.
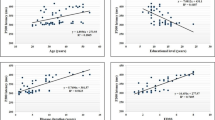
Nevertheless, a statistically significant negative correlation between P300 latency and Addenbrooke’s total score, as well as memory, language, and visuospatial domains, was observed. Meaning that, as the P300 latency increases, Addenbrooke’s total score and the aforementioned three domain scores decrease (Table 4; Fig. 2).

Scatter dot graph showing negative correlation between mean latency and Addenbrooke total score
As regards MRI findings in MS patients, about 53.3% of those patients had high lesion load (more than 9 lesions). As regards the lesions sites, 30% of cases had infratentorial lesions, 83.3% of cases had juxtacortical lesions, and 33.3% of cases had cervical lesions. Black holes (which indicate axonal loss) were present in 36.7% of cases. Moreover, enhancement on MRI (which indicates disease activity) was present in 56.7% of cases (Table 5).
MS patients were further classified according to their MRI findings. This classification showed that only patients with juxtacortical lesions had lower P300 amplitude. As regards P300 latency, there was no effect of MRI finding (Table 6).
Discussion
Multiple sclerosis (MS) is characterized by cognitive impairment, which significantly affects the lives of patients [6]. A significant number of individuals with MS experience cognitive dysfunction, which manifests as abnormalities in processing speed, learning and memory, visuospatial ability, and executive function. The exact pathogenic mechanisms are not yet fully understood, although they may be associated with pathological changes in white matter, certain neuronal gray matter structures, and immunological modifications. These changes have a significant effect on synaptic transmission and plasticity [16].
The study revealed a substantial disparity in the female to male ratio of MS among the study sample, with a ratio of 2.3 females to every 1 male. Wallin et al. [17] also found similar results, with a female to male ratio ranging from 2.3 to 3.5:1. This phenomenon may be attributed to physiological, hormonal, or hereditary reasons [18]. Harbo et al. [19] proposed that the X chromosome may directly contribute to autoimmunity, a hypothesis that has been suggested to be linked to the development of MS. Environmental variables, such as more sun exposure and greater use of vitamin D supplements, may contribute to the decreased occurrence of the condition in males [20].
The scales utilized in this study to assess MS cases indicated a moderate level of disability [11] with an average EDSS score of 3.38. This may be attributed to the relatively short duration of the disease in the study group with mean duration of 4.66 ± 3.83 years [21]. The PI score of 1.28 suggests a favorable prognostic value, while the MSSS score of 5.98 indicates a moderate level of severity. It is advisable to utilize many scales to enhance the reliability of assessments, particularly during the initial phases of MS [22].
Patients with MS often experience the presence of fatigue and depression. Fatigue is considered to be one of the most severe symptoms that significantly impact the overall quality of life (QoL) of these people [23]. Fatigue in patients with MS may result from physical factors, such as muscular weakness, which is defined by a decline in motor performance with continuous muscle activity. Furthermore, such individuals also suffer from cognitive fatigue, which shows up as a decrease in their capacity to complete cognitive tasks as a result of emotional instability, memory loss, and attention issues [24].
In this study, almost all MS patients suffered from fatigue and depression to various degrees. The coexistence of both fatigue and depression agreed with the finding of Tarasiuk et al. [25] who reported that depression can be a manifestation of fatigue. Patrick et al. [26] identified a strong correlation between fatigue and depression where both co-exist in over 50% of MS patients, suggesting common causes of both conditions. First, reduction in the level of serotonin and kynurenine (responsible for neurotransmission in meso-cortico-limbic pathways) by an inflammatory process leading to fatigue and depression [27]. Second, the formation of neurotoxic metabolites that maintain cell death, neurodegeneration, and inflammation in the gray and white matters, such as quinolinic acid [28]. Third, the oxidative and nitrosative stress that induce neurodegeneration through damaging the fatty acids and proteins of the cell membrane is followed by an autoimmune response [29]. Fourth, the possible role of steroids, where the low cortisol level has been implicated in chronic fatigue and depression in MS patients. Fifth, altered serotonin regulation in the limbic and paralimbic regions and the frontal cortex [30]. Finally, the emotional responses to pain, sleep disorders, and the lifestyle changes [31].
Assessment of the cognitive function can be done subjectively through using the Addenbrooke’s cognitive examination (ACE) which showed a significant reduction in MS patients in total scores in addition memory, fluency, language, and visuospatial scores (p < 0.001). Comparable results were also reported by Johnen et al. [32] who pointed out the occurrence of attention disorders, abstract thinking disorders, slow manual speed and skills, memory deficits, and poor language abilities, impaired processing speed and impaired executive functions [33].
Event-related potentials (ERPs) have been used for assessing the cognitive function in MS where the sclerotic plaques along the auditory pathway significantly alters its integrity. P300 is used in many studies to evaluate the central auditory processing of information during the disease course [34]. In this study, P300 was absent in small number of cases (bilateral absence in four cases and right absence in one case) in the study groups. In the rest of the cases, P300 latency was significantly delayed in comparison to normal cases.
Regarding P300 amplitude, it was reduced in the MS group; however, it failed to attain a significant level. Similarly, De Gennaro et al. [35] reported a non-significant reduction in amplitude of P300 in MS patients compared to control group. This could be due to the wide variation of P300 amplitude among normal subjects extending between limits as extreme as 5 to 20 μV.
Cognitive dysfunction and consequently impaired P300 response in MS patients might be attributed to either cortical lesions or disconnection between cortical and subcortical regions [36]. This disconnection would affect more than one cognitive domain, producing a variety of neuropsychological deficits [37].
Latency is a trustworthy measure of the speed at which information is processed in the brain. Prolonged P300 latency indicates a lengthy span of information processing. Conversely, a decrease in P300 amplitude indicates a disturbance in the functioning of certain regions (such as the frontal and parietal cortex, or thalamus) or a delay in the processing of information. Nevertheless, the diagnosis of cognitive impairment necessitates the presence of either prolonged P300 latency or lowered P300 amplitude, or both [38]. Fuhr and Kappos [39] reported that P300 latency provides a nonspecific, simple, and objective index of cognitive dysfunction and it is more sensitive to subtle early changes in cognitive processing impairments in MS patients. The statistically significant delayed P300 latency in the MS group compared to the control group was also found by Pokryszko-Dragan et al. [8] and Kaddoori [9] who reported significantly prolonged P300 latencies in multiple sclerosis patients. The theories about P300 origin suggest that it has mainly a frontal and a parietal cortex origin and any pathology affecting these parts in MS patients will subsequently affect P300 parameters [40]. So, abnormal P300 recording in MS patients might be specifically linked to cognitive symptoms.
The correlation analysis in this work revealed a negative correlation between P300 latency and Addenbrooke’s total score (ACE), memory, language, and visuospatial domains where the lower the scores, the more delay in P300 latency. Similar results were recorded by Fu et al. [41] who reported that P300 latency showed a significant negative correlation with the ACE total score and its memory and language domains. Moreover, Francisco et al. [42] found that P300 latency was more prolonged in patients with lower language scores, in addition to lower P300 amplitude in patients with lower verbal fluency scores.
Several MRI findings were found in this study such as high lesion load (535), juxtacortical lesion (83.3%), cervical lesions (33.3%), black holes (63.3%), and overall enhancement of MRI (56.7). Similar results were reported by Lazeron et al. [43] and Kimiskidis et al. [44] who found that T1 lesion load can be used as a significant predictor of P300 latency. Additionally, Nocentini et al. [45] reported that regional gray matter atrophy in well localized areas of the prefrontal, parietal, temporal, and insular cortex has a significant association with scores of tests measuring the cognitive function.
The assessment of cognitive impairment in MS patients is very important and should be considered as it causes economic and social problems. Identification of cognitive impairments in MS patients has important therapeutic and prognostic implications and plays an essential role in enhancing the quality of life of MS patients. The current study proved that P300 is a reliable indicator of cognitive impairment in MS patients either alone or in conjunction with other behavioral cognitive assessment tests.
Conclusion
Patients with MS suffer from cognitive impairment even if they are apparently normal. Identification of cognitive impairments through using Addenbrooke’s cognitive examination and P300 auditory evoked potential is of high clinical significance and has important therapeutic and prognostic implications in MS patients. P300 can complement or even replace neuropsychological methods for the assessment of cognitive dysfunction and its recording is recommended in MS patients.
Further research on different subtypes of MS is also necessary to evaluate the role of ERPs in conjunction with behavioral tests for evaluation and follow up on different types of MS in addition to studying the effectiveness of treatment and different rehabilitative methods on cognitive impairment and disease prognosis.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Hämäläinen P, Rosti-Otajärvi E (2016) Cognitive impairment in MS: rehabilitation approaches. Acta Neurol Scand 134(Suppl 200):8–13
Mahad DH, Trapp BD, Lassmann H (2015) Pathological mechanisms in progressive multiple sclerosis. Lancet Neurol 14(2):183–193
Patel SH, Azzam PN (2005) Characterization of N200 and P300: selected studies of the event-related potential. Int J Med Sci 2(4):147–154
Casali RL, Amaral MI, Boscariol M, Lunardi LL, Guerreiro MM, Matas CG et al (2016) Comparison of auditory event-related potentials between children with benign childhood epilepsy with centrotemporal spikes and children with temporal lobe epilepsy. Epilepsy Behav 59:111–116
Zwecker M, Sarova I, Lavie M, Zeilig G, Achiron A (2018) Detection of cognitive impairment in multiple sclerosis based on P300 event-related potential. Int J Phys Med Rehabil 6(04):1000479
Lazarevic S, Azanjac Arsic A, Aleksic D, Toncev G, Miletic-Drakulic S (2021) Depression and fatigue in patients with multiple sclerosis have no influence on the parameters of cognitive evoked potentials. J Clin Neurophysiol 38(1):36–42
Sundgren M, Maurex L, Wahlin Å, Piehl F, Brismar T (2013) Cognitive impairment has a strong relation to nonsomatic symptoms of depression in relapsing-remitting multiple sclerosis. Arch Clin Neuropsychol 28(2):144–155
Pokryszko-Dragan A, Zagrajek M, Slotwinski K, Bilinska M, Gruszka E, Podemski R (2016) Event-related potentials and cognitive performance in multiple sclerosis patients with fatigue. Neurol Sci 37(9):1545–1556
Kaddoori HG (2023) P300 event-related potentials in patients with multiple sclerosis. Egypt J Neurol Psychiatry Neurosurg 59(1):126
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G et al (2018) Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol 17(2):162–173
Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33(11):1444–1452
Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD (1989) The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol 46(10):1121–1123
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:561–571
McKinley R, Wepfer R, Grunder L, Aschwanden F, Fischer T, Friedli C et al (2020) Automatic detection of lesion load change in multiple sclerosis using convolutional neural networks with segmentation confidence. Neuroimage Clin 25:102104
Qassem T, Khater MS, Emara T, Rasheedy D, Tawfik HM, Mohammedin AS et al (2020) Validation of the Egyptian-Arabic version of the Addenbrooke’s cognitive examination III (ACE-III) in diagnosing dementia. Dement Geriatr Cogn Disord 49(2):179–184
Portaccio E, Amato MP (2022) Cognitive impairment in multiple sclerosis: an update on assessment and management. NeuroSci 3(4):667–676
Wallin MT, Culpepper WJ, Coffman P, Pulaski S, Maloni H, Mahan CM et al (2012) The Gulf War era multiple sclerosis cohort: age and incidence rates by race, sex and service. Brain 135(Pt 6):1778–1785
Whitacre CC (2001) Sex differences in autoimmune disease. Nat Immunol 2(9):777–780
Harbo HF, Gold R, Tintoré M (2013) Sex and gender issues in multiple sclerosis. Ther Adv Neurol Disord 6(4):237–248
Kragt J, van Amerongen B, Killestein J, Dijkstra C, Uitdehaag B, Polman C et al (2009) Higher levels of 25-hydroxyvitamin D are associated with a lower incidence of multiple sclerosis only in women. Mult Scler 15(1):9–15
Pinto MF, Oliveira H, Batista S, Cruz L, Pinto M, Correia I et al (2020) Prediction of disease progression and outcomes in multiple sclerosis with machine learning. Sci Rep 10(1):21038
Dandu SR, Engelhard MM, Qureshi A, Gong J, Lach JC, Brandt-Pearce M et al (2018) Understanding the physiological significance of four inertial gait features in multiple sclerosis. IEEE J Biomed Health Inform 22(1):40–46
Bakshi R (2003) Fatigue associated with multiple sclerosis: diagnosis, impact and management. Mult Scler 9(3):219–227
Linnhoff S, Fiene M, Heinze HJ, Zaehle T (2019) Cognitive fatigue in multiple sclerosis: an objective approach to diagnosis and treatment by transcranial electrical stimulation. Brain Sci 9(5):100
Tarasiuk J, Kapica-Topczewska K, Czarnowska A, Chorąży M, Kochanowicz J, Kułakowska A (2021) Co-occurrence of fatigue and depression in people with multiple sclerosis: a mini-review. Front Neurol 12:817256
Patrick E, Christodoulou C, Krupp LB (2009) Longitudinal correlates of fatigue in multiple sclerosis. Mult Scler 15(2):258–261
Maes M (2011) An intriguing and hitherto unexplained co-occurrence: depression and chronic fatigue syndrome are manifestations of shared inflammatory, oxidative and nitrosative (IO&NS) pathways. Prog Neuropsychopharmacol Biol Psychiatry 35(3):784–794
Heitmann H, Andlauer TFM, Korn T, Mühlau M, Henningsen P, Hemmer B et al (2022) Fatigue, depression, and pain in multiple sclerosis: How neuroinflammation translates into dysfunctional reward processing and anhedonic symptoms. Mult Scler 28(7):1020–1027
Pokryszko-Dragan A, Frydecka I, Kosmaczewska A, Ciszak L, Bilińska M, Gruszka E et al (2012) Stimulated peripheral production of interferon-gamma is related to fatigue and depression in multiple sclerosis. Clin Neurol Neurosurg 114(8):1153–1158
Hesse S, Moeller F, Petroff D, Lobsien D, Luthardt J, Regenthal R et al (2014) Altered serotonin transporter availability in patients with multiple sclerosis. Eur J Nucl Med Mol Imaging 41(5):827–835
Wallin MT, Wilken JA, Turner AP, Williams RM, Kane R (2006) Depression and multiple sclerosis: review of a lethal combination. J Rehabil Res Dev 43(1):45–62
Johnen A, Landmeyer NC, Bürkner PC, Wiendl H, Meuth SG, Holling H (2017) Distinct cognitive impairments in different disease courses of multiple sclerosis-a systematic review and meta-analysis. Neurosci Biobehav Rev 83:568–578
Hersche R, Roser K, Weise A, Michel G, Barbero M (2022) Fatigue self-management education in persons with disease-related fatigue: a comprehensive review of the effectiveness on fatigue and quality of life. Patient Educ Couns 105(6):1362–1378
Matas CG, Matas SL, Oliveira CR, Gonçalves IC (2010) Auditory evoked potentials and multiple sclerosis. Arq Neuropsiquiatr 68(4):528–534
De Gennaro R, Tamborino C, Mantovan M, Tessari A, Gastaldo E, Quatrale R (2013) 126. P300 and early multiple sclerosis: a study on 11 patients. Clin Neurophysiol 124(11):e217
Cecchi M, Moore DK, Sadowsky CH, Solomon PR, Doraiswamy PM, Smith CD et al (2015) A clinical trial to validate event-related potential markers of Alzheimer’s disease in outpatient settings. Alzheimers Dement (Amst) 1(4):387–394
Schochat E, Matas CG, Sanches SG, Carvallo RM, Matas S (2006) Central auditory evaluation in multiple sclerosis: case report. Arq Neuropsiquiatr 64(3b):872–876
Chiaravalloti ND, DeLuca J (2008) Cognitive impairment in multiple sclerosis. Lancet Neurol 7(12):1139–1151
Fuhr P, Kappos L (2001) Evoked potentials for evaluation of multiple sclerosis. Clin Neurophysiol 112(12):2185–2189
Juckel G, Karch S, Kawohl W, Kirsch V, Jäger L, Leicht G et al (2012) Age effects on the P300 potential and the corresponding fMRI BOLD-signal. Neuroimage 60(4):2027–2034
Fu X, Lu Z, Wang Y, Huang L, Wang X, Zhang H et al (2017) A clinical research study of cognitive dysfunction and affective impairment after isolated brainstem stroke. Front Aging Neurosci 9:400
Francisco HC, Brigola AG, Ottaviani AC, Dos Santos-Orlandi AA, Orlandi FS, Fraga FJ et al (2019) Relationship between cognitive processing, language and verbal fluency among elderly individuals. Dement Neuropsychol 13(3):299–304
Lazeron RH, Boringa JB, Schouten M, Uitdehaag BM, Bergers E, Lindeboom J et al (2005) Brain atrophy and lesion load as explaining parameters for cognitive impairment in multiple sclerosis. Mult Scler 11(5):524–531
Kimiskidis VK, Papaliagkas V, Sotirakoglou K, Kouvatsou ZK, Kapina VK, Papadaki E et al (2016) Cognitive event-related potentials in multiple sclerosis: correlation with MRI and neuropsychological findings. Mult Scler Relat Disord 10:192–197
Nocentini U, Bozzali M, Spanò B, Cercignani M, Serra L, Basile B, Mannu R, Caltagirone C, De Luca J (2014) Exploration of the relationships between regional grey matter atrophy and cognition in multiple sclerosis. Brain Imaging Behav 8:378–386
Acknowledgements
My special thanks to all the staff and patients in the Audiovestibular Unit and Neurology Department.
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
TG provided the research design and wrote the manuscript; AE and SR collected, tabulated, and analyzed data; MK did the statistical analysis; and MK and AE wrote and revised the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is approved by the Scientific Research Ethics Committee of Kafrelsheikh University with approval number, KFSIRB200-96. Informed written consent to participate in the study was provided by all participants since all of them are above 18 years.
Consent for publication
Written informed consent for the publication was obtained from the participants since all of them are above 18 years.
Competing interests
The authors have no competing interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elsayed, A., Kotait, M., Ragab, S. et al. Cognitive assessment in multiple sclerosis patients: electrophysiological and subjective studies. Egypt J Otolaryngol 40, 76 (2024). https://doi.org/10.1186/s43163-024-00648-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-024-00648-8