
Abstract
Objective
To evaluate the clinical use of acoustic change complex (ACC) as an objective tool in children who use hearing aids (H.As) and explore how far ACC threshold could be correlated to behavioral measures.
Study design
Sixty Arabic-speaking children (34 boys & 26 girls) using binaural H.As participated in the present study. Their age ranged from 6 to 12 years. The short stimulus used in the present study to elicit ACC response was “gap in tone.” Evaluation of H.As of children was performed in the form of questionnaire, aided sound field thresholds, central auditory tests, and aided/unaided cortical ACC recordings. The replicated ACC waveforms were collected and analyzed, and the aided ACC responses were compared with unaided ACC in addition to correlation of ACC-GDT to behavioral thresholds/scores.
Results
The highest percent of ACC detectability achieved with gap in tone with 50-ms duration. Percent detectability reached 65% in aided condition and decreased to 25% in unaided test condition. The aided ACC wave morphology showed no significant difference when compared with unaided condition; however, a significant decrease in ACC latency was observed in the aided condition. The ACC response was elicited easily at 40-dB sensation levels or at MCL in both conditions. The ACC-GDT showed correlation to questionnaire scores rather than behavioral test (AFT).
Conclusions
ACC to relatively short duration stimulus can be successfully recorded in hearing-impaired children in aided and unaided conditions. ACC response parameters (detectability and P1 latency) can reflect the benefit from H.As as an objective measure in evaluation of young children and difficult to test subjects with the usual subjective measures, and finally, ACC-GDT may add a predictive value to questionnaire scores which may help in case of inability of parents or caregivers to fulfill the entire questionnaire items.
Similar content being viewed by others


Background
Monitoring the hearing-related outcomes of infants and children with hearing loss and who are fitted with suitable hearing aids is essential and can be accomplished by behavioral and/or subjective measures.
Behavioral measures in hearing aid users may be placed on a continuum ranging from questionnaires up to central auditory processing tests. Questionnaire is one of the behavioral tests that could be completed by parents or caregivers. The Meaningful Auditory Integration Scale (MAIS) is a parent report scale (10 items) designed to assess hearing-impaired children’s meaningful use of sound in everyday situation [1]. The Arabic version of MAIS questionnaire was developed and standardized by Kamal et al. [2].
One of the central abilities that affect performance of the hearing-impaired children is the auditory temporal processing ability as it is affected in individuals with sensorineural hearing loss. Shabana et al. [3] conducted a study about temporal processing abilities in individuals with mild and moderate degree of hearing loss and found that significant score difference in temporal processing abilities compared with norms and recommended to study the previous abilities after rehabilitation with suitable hearing aids. Mourad et al. [4] also revealed that children with hearing loss showed temporal processing deficit which varies as a function of degree of loss.
Although audiologists find difficulty to apply the previous behavioral measures on young children and/or those with low intelligent quotient (IQ), it could be overcome by using objective tests, and one of them is the acoustic change complex (ACC). ACC is a cortical auditory-evoked potential (CAEP) evoked in response to a change in an ongoing sound [5]. Several studies have shown that the ACC can be recorded in children with normal hearing, CI users, and H.As using gap-in-tone stimuli [6,7,8], and the authors of the studies examined the effects of amplification on the ACC. The results indicated that the ACC can be recorded reliably in individuals using HAs. Hence, this work is designed to study ACC in children using H.As in response to gap-in-tone stimulus. The aim is to provide an objective tool for assessment of temporal resolution ability in hearing aid users and explore how far ACC response parameters could be correlated to behavioral tests. This may be considered as an objective method for evaluating H.As performance in children independent of the abilities or degree of their cooperation.
Method
Research design: Cross-sectional study.
Participants
Sixty Arabic-speaking children participated in the present study. Their age ranged from 6 to 12 years. All children were collected from the Audiology Unit of Ain Shams University hospitals, ORL Department, Cairo, Egypt, over the period from September 2018 to December 2020.
Inclusion criteria are as follows:
-
The degree of hearing loss ranges from mild to moderately severe.
-
Regular use of binaural H.As for at least 1 year
-
Cooperative child, from whom reliable aided behavioral threshold could be obtained
-
Aided thresholds within long-term average speech spectrum
-
Average or above average intellectual quotient (IQ) based on psychometric evaluation
Methodology
MAIS questionnaire (Appendix 1.1)
The Arabic version of the Meaningful Auditory Integration Scale (MAIS) was applied in the research. It was standardized and developed by Kamal et al. [2].
It is a parent report scale (10 items). This parent-report scale was administered in an interview format. This technique avoided “leading” the parents to provide desired responses and also discouraged yes–no answers.
Answers were given by rating the frequency of the desired behaviors on a 5-point ranging from “never” (= 0) through “regularly” (= 4). As there were 10 items, the maximum total score was 40 points.
Aided psychophysical behavioral testing for temporal resolution
Auditory Fusion Test-Revised (AFT-R) is a measure of temporal resolution through determining the auditory fusion threshold in ms [9]. It consists of a series of pure tone presented in pairs. The inter-pulse interval (IPI) between each pair of tones increases and decreases in duration. The child was instructed to report either hearing one or two tones with each stimulus pair.
AFT-R had two subtests: Subtest 2, standard test (Appendix 1.2): it contains IPI that range from 0 to 40 ms and subtest 3, expanded test (Appendix 1.3): the test included only three frequencies (1000 Hz, 4000 Hz, and 250 Hz). The IPI ascended from 40 to 300 ms and then descended to 30 ms. Either subtest II or subtest III expanded and was done in sound field at 0° degree azimuth and 1 m apart from subject’s ear.
-
Aided acoustic change complex (ACC)
For ACC recording, gaps with different durations were introduced in a tone-burst stimulus “1000 Hz” by El-kholy et al. [6]. The tonal stimulus duration was 500 ms, whereas gap durations were ranging from 10 to 200 ms. Gaps generated with different durations including 200–150-120–100-90–80-70–60-50–40-20–10 ms with the reference point of 50-ms gap duration, according to the presence or absence of ACC response, were decreased or increased in duration to reach the gap detection threshold (GDT).
Gap “50-ms gap duration” was introduced at 350 ms from the onset (Fig. 1). This onset of change was decreased gradually by increasing the gap duration to be introduced at 300 ms from the onset with 150-ms gap duration and 250 ms from the onset at 200-ms gap duration. Upon decreasing onset of change, to be lower than 250 ms, no proper ACC response could be recorded, thus limiting the maximum gap duration to 200 ms; this could be attributed to the overlap between the onset and ACC peaks or failure to compensate the long refractory nerve periods [10].
-
Equipment: Bio-logic Navigator Pro AEP system (version.7.0.0) connected to a loudspeaker.
-
Recording technique: The stimuli were delivered through a loudspeaker connected by an external amplifier to the evoked potential equipment. The loudspeaker was set at 0 azimuth facing the patient 1 m apart. During ACC recording, the children were seated comfortably watching a muted cartoon movie to distract them and to ignore the stimuli presented.
-
Electrode montage: The active electrode was placed on the high forehead (Fz) referenced to the mastoid (Rt or Lt), and the ground electrode was placed on the low forehead (FPz).
-
The impedance was less than 5 KΩ.
-
The EEG data was digitized (sampling rate: 512 Hz). The responses were filtered between 0.1 and 100 Hz and amplified (1000 gain). Response analysis window was included — 100 ms pre-stimulus and 710 ms post-stimulus, total 800 ms. The number of accepted sweeps was 50.
-
Unaided ACC recording: The recording was done while the child took off his hearing aids. It resembled the aided ACC recording steps.
-
The replicated ACC waveforms (P1-N1-P2-N2) were collected for all children. The pattern of waveform morphology was determined followed by latency and amplitude measurements.

Example for gap in tone with 100-ms gap duration. a The silent gap was introduced at 350 ms from onset and lasted for 100 ms
Data analysis
-
Statistical analyses were performed using SPSS 16. The independent t-test was used to compare between two different (independent) groups, while ANOVA test was used to compare between > two different groups. Chi-square test was used to examine the relationship between two qualitative variables.
-
The Pearson correlation measures the strength of the linear relationship between two variables. A level of p < 0.05 was considered significant, while p < 0.01 was highly significant. A statistician helped in this study.
Results
Q1, 2, 8, and 9 showed that 4 “regularly” was the most frequent, whereas in Q4, 2 “occasionally” was the most frequent one.
Forty-eight children could get their GDT through subtest II, the remaining children failed, and only 5 children out of 12 got scores at subtest III. Table 1 showed highly statistically significant differences between low freq. thresholds and high freq. threshold in subtests II and III.
-
The ACC threshold.
-
ACC morphology.
The adult morphology (P1, N1, P2) was the dominant in aided condition, and the child morphology (P1, N2) was the dominant in unaided condition. However, there was no statistically significant differences.
The table showed highly statistically significant correlation with total score of questionnaire.
-
On the other hand, there was no statistically significant correlation between ACC gap detection thresholds with AFT-R thresholds.
Discussion
MAIS questionnaire was initially developed for parents and educators to evaluate the benefit obtained by children who were fitted with hearing aids or cochlear implants [1]. Kamal et al. [2] reported that MAIS was considered as a valid tool for evaluation of CI children after auditory training. They observed improvement of post training scores when compared with pre-training ones.
For instance, in the current work, the children got best scores (4/4) at Q1, 2, 8, and 9 (Fig. 2). Q1 and 2 reflect the child’s confidence in using the device; it is accepted and coincides with one of the inclusion criteria for the children to be regular user of H.As. Q8 and 9 reflect understanding of sounds, e.g., “to differ between human and non-human sounds,” and may be explained by duration of hearing aid fitting > 1 year besides the relatively old age of children which “range from 6 to 12 years.” Lower score (2/4) was dominant at Q4 which reflects awareness to sounds in background noise, and lower scores indicate that hearing-impaired children to some degree are facing challenges to listen in noise. Despite early amplification and seemingly sufficient levels of aided audibility, it can still not make up for the consequences posed by the sensorineural HL [11].

Column chart: the vertical axis represents the scores, and the horizontal one represents the items with their answers (5-point ranging from “never” (= 0) through “regularly” (= 4)
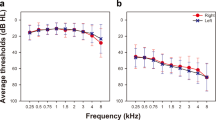
Individuals with hearing loss can detect gaps when sounds that do not have many temporal fluctuations are presented at higher levels as when they are presented through amplification [12]. In AF test, 48 children passed subtest II, and in the remaining 12 children, 5 only could pass subtest III, and GDTs were lower at low freq. (250 Hz) when compared with high freq. (Table 1 & Fig. 3). This is in discordance with Balen et al. [13]; they reported no significant differences across frequencies on population with normal or conductive hearing loss. This disagreement may be attributed to the type of hearing loss of the study group. A considerable variability in behavioral gap detection thresholds “behavioral GDT” among children was obtained ranging from 5 to 200 ms. This could be explained by the influence of hearing loss (with different degrees) that may impact GDTs. Nonetheless, another factor that was reported to have an influence is the age.

Column chart representing means of AFT thresholds at subset II (a) & III (b) across frequencies with better (lower) thresholds at lower frequencies
The aim of the 1st stage of ACC recording was to get the ACC-gap detection threshold (GDT) in aided and unaided conditions. Two children, while using their devices, were able to elicit ACC-GDT at 10-ms gap duration, while no one scored \(10 msec\) while removing their devices (the lowest ACC-GDT in unaided condition was 20 ms). These results suggest that speech recognition abilities of H.As users improved by signal processing of their devices, which is important in identifying small acoustic variations in speech signal over time, allowing the perception of speech. Figure 4a and b illustrates that the children while using their hearing aids gave a well-distributed pattern of ACC_GDT at gap duration with 50 ms and below, whereas after taking off their devices, the pattern was randomly distributed.

The ACC threshold of different gap-in-tone durations in aided (a) and unaided conditions (b), with tendency for well-distributed pattern at 50-ms gap-in-tone duration and below in aided condition
The aim of the second stage was further analysis of ACC parameters at 50 ms (morphology, latency, and amplitude). As regards morphology, the adult “P1-N1-P2” complex morphology was the dominant compared with child “P1 and N2” morphology (Fig. 5). This is in agreement with Small and Werker [10] who reported that the infant responses resemble the P1-N1-P2 complex recorded in adult participants in terms of the morphology of the waveforms, but they found that there were obvious differences in the relative prominence of the peaks and significantly prolonged latencies relative to the adults due to immaturity. However, in unaided condition, the P1 and N2 morphology was the dominant. Latency of ACC-P1 was shorter and reached significant difference with amplification (Table 2). This could be attributed to the amplification effect because it may improve neural representation of the speech signal in H.As users as reported by Jenkins et al. [14].

Illustrating the ACC “child-type” morphology in a male child, 7 years old, with moderately severe degree of hearing loss while using his hearing aids
There was a negative correlation between total scores of MAIS questionnaire and ACC-GDT (i.e., the higher the total score of MAIS, the better ACC-GDT) (Table 3), this result agrees with Aurélio et al. [15], those authors studied the value of MAIS questionnaire in hearing aid users, and they reported that all items of MAIS questionnaire showed improvement in the performance of children, either by objective or subjective measures, because of the regular use of their hearing aids. On the other hand, ACC to gap-in-tone thresholds showed no significant correlation with AFT thresholds. This is in agreement with Shalaby et al. [16] who concluded that ACC response parameters (lat. and amp.) had no correlation with behavioral measures in H.As users; on the other side, Abdel Maksoud et al. [17] concluded that ACC-GDT can predict psychophysical temporal resolution in young children or difficult to test population in CI users. The failure to find a significant relation between ACC-GDT and AFT-R test could be attributed to the relatively short stimulus used which might not be long enough to accommodate the neural refractory periods in the immature brain [10].
Conclusion
ACC to relatively short duration stimulus (500 ms), which is available in many equipments rather than long duration stimulus > 1 s, can successfully be recorded in hearing-impaired children either in aided or unaided conditions, it is preferable to use gap-in-tone stimulus with cutoff limits at 50 ms, ACC response parameters (detectability and P1 latency) can reflect the benefit from H.As which can help in evaluation of H.As “especially in young children and/or difficult to test subjects with the usual subjective measures,” and finally, ACC-GDT may add a predictive value to questionnaire scores which may help in case of inability of parents or caregivers to fulfill the entire questionnaire items.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Robbins AM, Renshaw JJ, Berry SW (1991) Evaluating meaningful integration in profoundly hearing impaired children. Am J Otolaryngol 12(Suppl):144–150.
Kamal N, Tawfik S, Bassiony S, Hazzaa N, Shalaby A, Omar P (2009) Efficacy of auditory processing training in cochlear implant children: a new approach [Doctoral thesis in Audiology]. Audiology Unit, ORL Department, Ain Shams University, Egypt.
Shabana M, Shalaby A, Dabbous A, Emara A (2009) The implication of peripheral hearing loss on temporal auditory processing in children [Doctoral thesis in Audiology]. Audiology Unit, ORL Department, Cairo University, Egypt.
Mourad M, Talaat M, Abdou R, Abdelkader G (2016) Performance of children with mild or moderate sensory hearing loss on central auditory tests. Egypt J Otolaryngol 32:298–305.
Martin BA, Boothroyd A (1999) Cortical, auditory, event-related potentials in response to periodic and aperiodic stimuli with the same spectral envelope. Ear Hear 20:33–44.
El-kholy W, Hassan D, Shafik N and Eltoukhy Y. (2020). Acoustic change complex (ACC) using speech and non-speech stimuli in normal hearing children. QJM: An International Journal of Medicine, Volume 113, Issue Supplement_1, March 2020, hcaa047.008, Published:05 May 2020.
Shalaby A, El-Kholy W, Hassan D. and Mohamed A. (2020). Relation between cortical auditory evoked potentials and behavioral auditory discrimination in cochlear implant children. QJM: An Internationa l Jour nal of Medicine, 2020, Vol. 113, Suppl.
Zhang VW, Ching TYC, Van Dun B, Bardy F, Ibrahim R, Wong C, Rance G, Chisari D, Sharma M and Dillon H.(2021): The relationship between the acoustic change complex and behavioural response of speech discrimination in infants and young children. Presented in 21th IERSAG “International Evoked Response Audiometry Study Group'” free online paper session.
McCroskey and Keith. (1996) Auditory Fusion Test-Revised. Auditec; St Louis, MO.
Small SA, Werker JF (2012) Does the ACC have potential as an index of early speech discrimination ability? A preliminary study in 4-monthold infants with normal hearing. Ear Hear 33:e59–e69.
McCreery RW, Walker EA, Spratford M, Oleson J, Bentler R, Holte L, Roush P (2015) Speech recognition and parent ratings from Auditory Development Questionnaires in children who are hard of hearing. Ear Hear 36(1):60S-75S.
Vishakha W. Rawool. (2006) The effects of hearing loss on temporal processing; part 3: addressing temporal processing deficits through amplification strategies.
Balen S, Bretzke L, Mottecy C, Liebel G, Boeno M, Gondim L (2009) Temporal resolution in children: comparing normal hearing, conductive hearing loss and auditory processing disorder. Braz J Otorhinolaryngol 75(1):123–129.
Jenkins KA, Fodor C, Presacco A, Anderson S (2017) Effects of amplification on neural phase locking, amplitude, and latency to a speech syllable. Ear Hear 39(4):810–824.
Aurélio FS, Silva SP, Rodrigues LB, Kuniyoshi IC, Botelho MSN (2012) Satisfaction of patients fit with a hearing aid in a high complexity clinic. Rev Bras Otorrinolaringol 78(5):69–77. https://doi.org/10.5935/1808-8694.20120011. (PMid:23108823).
Shalaby AA, El-Kabarity RH, Shafik NA, Abd-Alfattah M (2022) (2022) Evaluation of performance of hearing aid users using acoustic change complex (ACC) and behavioral measures. Int J Pediatr Otorhinolaryngol 161:111271. https://doi.org/10.1016/j.ijporl.2022.111271. (Epub 2022 Aug 12 PMID: 35988371).
Abdel Maksoud A, Bassiouny S, Abdel Rahman T, Hanafy KM (2022) Assessment of outcome measures after audiological computer-based auditory training in cochlear implant children. Int J Pediatr Otorhinolaryngol 160:111217.
Acknowledgements
Special thanks to the children and their parents for participation in the practical part of the research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
AS and WE initiated the stimuli (gaps in tone) to elicit ACC response, recommended the data analysis as regard ACC-GDT to be performed in two stages, and revised the result section. RE and NS revised the practical part of the research, analyzed and interpreted the patient data, and revised the manuscript. MA performed the practical part of the research and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Research Ethics Committee at (Ain Shams University) approved the study. The date of Research ethics committee approval was on 9/9/2018 (FMASU MD 285/2018. Informed written consent to participate in the study was provided by all participants' parents (as all children under 16).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
43163_2024_619_MOESM1_ESM.docx
Supplementary Material 1: Appendix 1.1. MAIS Questionnaire (Robbins et al.,1991). Appendix 1.2. AFT-R (subtest II) (McCroskey and Keith, 1996). Appendix 1.3. AFT-R (subtest III) (McCroskey and Keith, 1996).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shalaby, A.A., El-Kholy, W.AH., El-kabarity, R.H. et al. Acoustic change complex (ACC) as a new tool in assessment of hearing aid performance in children. Egypt J Otolaryngol 40, 59 (2024). https://doi.org/10.1186/s43163-024-00619-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-024-00619-z