
Abstract
Introduction
Auditory training (AT) exercises as the main part of auditory rehabilitation have emerged as a promising method for enhancing auditory perception and communication skills in individuals with hearing impairments or difficulties in auditory processing. Through AT, the central auditory nervous system (CANS) undergoes changes that optimize neural circuits, resulting in improved auditory perception. Auditory-evoked potentials (AEPs), including the auditory brainstem responses (ABRs) and cortical auditory-evoked potentials (CAEPs), offer objective measurements of neural responses and serve as valuable biomarkers to assess the effectiveness of AT.
Methods
For this systematic review, we conducted a comprehensive search in multiple databases, including MEDLINE (via PubMed), Science Direct, Web of Science, and SciELO, up until August 18, 2023. There were no study type restrictions or limitations on publication time. Following a careful assessment of the article quality and their alignment with the inclusion and exclusion criteria, a total of 25 articles were selected for inclusion in this study.
Results
Based on the findings of the reviewed studies, it has been reported that AT exercises lead to an increase in the amplitude of waves in both brainstem and cortical AEPs, with the exception of P1 and N2 waves. Furthermore, it has been observed that the latency of these responses decreases following AT.
Conclusion
The application of brainstem and cortical AEPs as objective electrophysiological tools holds promise in assessing the effectiveness of AT exercises and confirming the selected approach for AT.
Similar content being viewed by others


Background
Auditory training (AT) exercises have garnered significant attention within the audiology field as a promising method to enhance auditory perception and improve communication skills in individuals who have hearing impairments or difficulties with auditory processing. AT is an intentional and methodical presentation of sounds that aims to help individuals discern perceptual distinctions among those sounds. It involves the use of strategies to develop or restore auditory perception, which plays a crucial role in linguistic and phonemic processing necessary for understanding speech [1, 2].
AT is typically administered either formally or informally. Formal training employs recorded stimuli delivered through a computer or CD player, allowing for more control over the difficulty of the training. Some formal training approaches utilize a computer-based auditory training (CBAT) method. On the other hand, informal training is generally less concerned with controlling the stimuli and may involve face-to-face presentations rather than recorded stimuli. Informal training often takes place in homes or schools and may utilize age-appropriate words, sentences, or nonverbal stimuli [3].
There is a growing body of evidence demonstrating the benefits of AT in the rehabilitation of individuals with hearing impairments, central auditory processing disorder (CAPD) [4], autism spectrum disorder (ASD) [5], language and learning difficulties [6], and cognitive decline in the elderly [7]. AT has shown promising results in improving auditory perception and communication skills in these populations. Furthermore, this intervention has the potential to enhance their overall quality of life by enabling better speech comprehension and communication abilities.
The central auditory nervous system (CANS) undergoes behavioral perceptual improvements and neurophysiological alterations as a result of AT. These changes indicate the transfer of acquired skills and the plasticity of the nervous system, which adapts to meet the demands of the auditory environment. Through AT, the neural circuits are optimized by increasing the involvement of neurons, modifying neural temporal synchronicity, and augmenting synaptic connections. These mechanisms contribute to the refinement and enhancement of the physiological processes underlying auditory perception and processing [8, 9].
Auditory-evoked potentials (AEPs) are objective tests that offer valuable insights into the central auditory pathways and can serve as potential biomarkers for sensory processing. Additionally, AEPs play a crucial role in monitoring the effectiveness of auditory rehabilitation and can be utilized to objectively assess treatment or training outcomes. By providing quantitative data, AEPs enable the evaluation and comparison of participants at different time points, allowing for a comprehensive analysis of their progress. One noteworthy measure of improvement is the decreased latency of AEPs, which is considered a neurophysiological manifestation of neuronal plasticity [9, 10].
AEPs serve as indicators of the neural responses involved in processing complex sounds, representing the activity within various regions of the auditory pathway, including both the brainstem and cerebral structures. AEPs originating from the brainstem encompass the auditory brainstem responses (ABRs) and the auditory brainstem response to complex sounds (cABR), which reflects the encoding of speech characteristics in the rostral brainstem auditory network.
The ABR is a noninvasive method that captures stimulus-locked, synchronous electrical events from the scalp. It consists of seven peaks, with peaks I, III, and V being commonly observed and used for auditory threshold estimation and diagnostic purposes [11].
The cABR provides valuable insights into how the brainstem represents important aspects of the speech signal. The cABR consists of two distinct elements: the onset response (V-A complex), and the frequency-following response (FFR), which includes waves C, D, E, and F. The FFR reflects the brainstem’s encoding of the fundamental frequency and harmonic structure of complex stimuli, and the wave O marks the stimulus offset [12].
In addition, cortical auditory-evoked potentials (CAEPs) such as P1, N1, P2, N2, and P3 waves arise from the auditory cortex and other associated cortical areas. The presence of CAEPs indicates that the brain has detected the acoustic signal [1]. Passive cortical AEPs, such as P1, N1, P2, and N2, occur within 300ms of a sound’s onset and are believed to represent electrical activity in different cortical areas involved in auditory processing [13]. The P3 component, on the other hand, reflects the process of attention and perception of unique acoustic features during CAEP testing [10].
Combined, brainstem and cortical AEPs offer a valuable tool for comprehending the neural representation of sounds and neuroplasticity following aural rehabilitation, including interventions such as AT, across different levels of the auditory system [14, 15].
Selecting the appropriate method for AT is crucial and can result in optimized outcomes and improvements in auditory processing abilities. This aspect requires particular attention, especially in children with hearing impairments, as effective AT significantly impacts the development of auditory skills and, ultimately, communication abilities. Several studies have reported findings on modified AEPs post-AT interventions, illustrating neuroplastic changes in the CANS following successful AT. Regrettably, professionals in audiology and related fields nowadays lack enthusiasm for conducting electrophysiological assessments as part of their AT procedures. In our systematic review, we seek to summarize past research findings and discuss the alterations in brainstem and cortical AEPs in both normal hearing and hearing-impaired children and adults after AT exercises. We also aim to highlight the significance of incorporating electrophysiological assessment in evaluating the effectiveness of AT interventions and in formulating successful strategies for AT.
Main text
Search strategy
In this review study, we conducted systematic searches in MEDLINE (via PubMed), Science Direct, Web of Science, and SciELO databases and performed a manual search in the Google Scholar database until August 18, 2023. We prioritized a comprehensive approach without limitations on time or study type to ensure a thorough analysis of the available literature. Although we regrettably did not have access to ProQuest, Scopus, and Cochrane Library databases, we made significant efforts to ensure our search encompassed relevant sources.
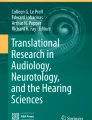
Two independent reviewers meticulously conducted online database searches, adhering to the rigorous Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [16]. The search strategy applied is presented in Fig. 1, based on the PRISMA flow diagram. To ensure transparency and accountability, the protocol of this review has been registered and assigned the PROSPERO ID: CRD42023463138 in the PROSPERO international prospective register of systematic reviews.

Flow chart of systematic search and article selection
We developed the PECO framework by aligning it with our research question and the inclusion and exclusion criteria outlined for our study. This framework guided us in conducting a systematic search for articles. Our search focused on studies that investigated the alterations in brainstem and cortical AEPs following AT interventions. Specifically, we looked for studies that either compared AEP changes between a group undergoing AT and a control group or examined changes within the same group before and after AT sessions. We chose not to target a specific age group with keywords, as we decided to evaluate the changes in AEPs across both children and adults.
During the article search phase, we used various keywords to cover different aspects of AT interventions, such as “auditory training,” “audiologic rehabilitation,” “listening training,” and “auditory processing training”. We also used specific keywords like “cortical auditory-evoked response,” “cortical auditory-evoked potential,” “P1-N1-P2,” “auditory-evoked potential,” “auditory-evoked response,” “auditory brainstem-evoked response”, and “auditory brainstem response” to target articles related to cortical and brainstem AEPs. By utilizing the advanced search features available, we aimed to comprehensively identify articles that covered both fields and provided valuable insights into the effects of AT on AEPs.
Inclusion and exclusion criteria
This review will encompass a range of study types, including randomized controlled trials, cross-sectional studies, case-control studies, and cohort studies, in order to provide a comprehensive analysis. To be eligible for inclusion, articles must meet specific criteria. These criteria include publication in reputable English-language journals, containing relevant indicators related to the research topic and presenting original research on the effects of different types of AT on brainstem or cortical AEPs after inversion. We exclusively included articles that involved the evaluation of human participants in their studies.
Conversely, articles such as letters to editors, book chapters, review guidelines, meeting abstracts, editorials, various review articles and meta-analyses, dissertations and research protocols, animal studies, studies that evaluated AEPs following musical training, and studies with unclear or irrelevant results were excluded from consideration.
We excluded book chapters and review articles as they did not present original research findings relevant to our research question. Additionally, non-English articles were omitted due to language proficiency constraints, which hindered our ability to assess the quality of these articles. However, we did not exclude studies that employed stimuli in languages other than English during their electrophysiology assessment. Furthermore, studies that reported results on AEPs other than our specified target AEPs, such as the auditory middle latency responses and auditory steady-state responses, were also excluded.
Data extraction and quality assessment
We used EndNote software (version X7, Thomson Reuters, 2014) to remove duplicate articles and evaluate the suitability of article titles and abstracts in relation to the study topic. Articles that did not meet the criteria based on title alone, and subsequently based on both title and abstract, were excluded from further analysis.
During the subsequent phase, the full texts of the selected articles were subjected to a quality assessment using the Joanna Briggs Institute (JBI) checklists. The final analysis involved a careful examination of the study’s purpose, methodology, results, and conclusions. Only articles and studies that met the inclusion and exclusion criteria were included in the data extraction stage. Both authors independently conducted these steps, and any discrepancies or disagreements were addressed through discussions or, if needed, by seeking the opinion of a third expert. By adhering to rigorous quality assessments and fostering consensus among the reviewers, our aim is to ensure the reliability and validity of the selected articles.
We utilized Excel software for data extraction purposes. The information extracted consisted of various relevant details, including the name of the first author, publication year, study location, participant count and age, study type, details regarding the type and duration of AT sessions, characteristics of stimuli used for recording potentials, and the reported changes observed in AEPs following AT. In the result section, these extracted details will be presented and analyzed.
Results
Literature search
After conducting a thorough search in the databases, we obtained a total of 310 articles, which were imported into the EndNote software for subsequent analysis. Among these articles, 27 duplicates were identified and removed automatically, resulting in 283 articles remaining for further screening. During the screening process, 177 articles were excluded based on their titles as they were deemed unrelated to the research topic. Additionally, after evaluating both the titles and abstracts, another 58 articles were excluded for being unrelated. Subsequently, the full texts of the remaining 48 articles were carefully examined for eligibility evaluation.
Out of the articles that remained, 2 were excluded as they were focused on animal studies, and another 2 were excluded because they were not written in English. Furthermore, 5 articles were excluded as they were review studies, theses, research protocols, or book chapters. We excluded one study that encompassed participants with unilateral hearing loss because of inconsistencies related to hemispheric lateralization and plasticity in the ipsilateral pathway. Two studies were eliminated because they involved participants with cochlear implants, attributing the exclusion to the impact of pre and post-operative factors on the results of AT. Additionally, 4 articles were excluded as they did not examine the changes resulting from AT exercises. Furthermore, 7 articles were excluded as their results were not relevant to the subject of the study or were unclear. Finally, the remaining 25 studies were included for the analysis of results.
Study characteristics
Table 1 presents the extracted information related to the study after assessing the quality of the chosen articles by the authors. We structured the results table according to the age group and hearing status of the participants. The segregation between adults and children was done because alterations in AEPs in young individuals may be influenced by neuroplasticity during their developmental maturation, whereas in adults, changes in these potentials are primarily associated with neuroplasticity resulting from AT.
The selected articles span from 2001 to 2023 and include 3 case reports and 21 clinical trials, out of which 13 were controlled and featured a control group for comparison. All of the reviewed experiments in this study had a combined total of 430 participants who participated in AT sessions. These participants were of various age groups and included children, young adults, and elderly individuals.
The analyzed studies employed different techniques of AT with a broad duration range stretching from 30 min to more than 50 h, conducted through multiple sessions across several months. Various AT methods utilized in the included studies encompass “acoustically controlled auditory training”, “auditory training with vocal duets,” “voice onset time (VOT) differentiation,” “computerized auditory training,” “Earobics,” “Treinamento musical auditivo,” and additional approaches.
Different recording devices were employed, and the stimuli utilized in the recordings included click stimuli, tonal stimuli, and speech stimuli (such as vowels, CVs, and sentences), delivered at intensities between 70 and 85 dB. Additionally, in eight experiments, the oddball paradigm was utilized as a method of transmitting stimuli to elicit responses.
Brainstem auditory-evoked potentials (ABR-cABR)
Out of the total experiments reviewed, 10 have documented the modifications in brainstem-originated AEPs. In the ABR-related articles, one study illustrated a decline in wave I absolute latency and shortening of inter-peak latencies I–III, III–V, and I–V [29], and the other one demonstrated a decrease in the latency of all waves [24]. Furthermore, one experiment recorded an increase in wave V amplitude [9], and the other study suggested no variation in ABR waves before and after AT [34].
Regarding the reports involving cABR, a total of two studies observed reduced latencies for all cABR components [19, 26], while one study noticed an increase in peak C amplitude [17], and one study reported a decrease in peak C latency [22], and another one observed decreased latency for peak E [18]. Additionally, one of the studies documented an increase in V-A complex amplitude and decreased latencies for V, A, and C waves following AT sessions [11].
Cortical auditory-evoked potentials (P1-N1-P2-N2)
Out of the studies examined, a total of 19 reported changes in cortical AEPs after completing AT. Two studies indicated a decrease in P1 amplitude following the exercise [6, 32], two studies signaled reduced P1 latency [22, 25], and seven studies observed an increased N1-P2 amplitude [13, 23, 27, 28, 30,31,32]. Moreover, two studies reported reduced P2-N2 latency [10, 20], one study recorded an increased amplitude and decreased latency of the P1-N1-P2 complex [9], and two studies mentioned decreased N2 amplitude and latency due to AT [6, 22]. One study indicated a decrease in N1-P2 latency following the exercises [22].
Event-related potentials (P3)
Out of all the experiments, four cases indicated an increase in P3 amplitude after AT [2, 21, 22, 29], while six cases presented reduced P3 latency [8, 10, 20, 22, 28, 33]. Lastly, only one study found no significant difference in CAEPs after completing AT exercises [34].
Discussion
AT can be administered through various methods, including face-to-face sessions and computer-based programs. It aims to enhance a range of auditory skills such as detection, discrimination, identification, and comprehension. Different stimuli, such as syllables, words, phrases, and sentences, are used to train these auditory skills, leading to overall improvement [35]. For children with hearing loss who undergo cochlear implantation or use hearing aids, AT is crucial and should commence as soon as sound transmission becomes possible through interventions.
AT is known to induce neural plasticity, and the organization of the auditory cortex is closely linked to auditory experiences. Evidence of experience-based plasticity in school-age children suggests that electrophysiological measures like AEPs can be utilized to establish the relationship between neural properties and changes in auditory behavior resulting from training [11, 36].
Brainstem AEPs enable the evaluation of synchronized neural activity in response to sounds at the subcortical level, offering valuable insights into the experience-dependent plasticity occurring within this subcortical domain [11]. AT has shown the potential to rewire the biological processing in the auditory brainstem by promoting an increase in synaptic connections within the CANS. This suggests that AT can have a significant impact on the neural circuitry involved in auditory processing at the brainstem level [11].
The majority of the studies found that AT exercises led to improvements in the brain’s response to sound. These improvements were seen in the form of reduced latency and increased amplitude of the AEPs originating from the brainstem. The increase in amplitude could be attributed to the enhanced speed, strength, and reliability of the brainstem’s response to auditory stimuli, particularly speech. The decrease in latency suggests that there may be improved synchronization in how the brainstem nuclei respond to acoustic stimuli, leading to a better correlation between the stimulus and the brain’s response [11].
CAEPs is a method used to evaluate the cortical activities of the brain, specifically its ability to discriminate, integrate, and pay attention to auditory stimuli. This assessment involves the functioning of various cortical auditory pathways, including the primary auditory cortex and associative cortical areas [10].
The majority of the studies reviewed, reported significant alterations in CAEPs. These changes encompassed a reduction in latency for all components of CAEP, including P1, N1, P2, N2, and P3 waves. Additionally, there was an observed increase in the amplitude of the N1-P2 complex (or the amplitude of the P2 wave), which appears to be the most frequently reported change in the literature. Conversely, there was a decrease in the amplitude of the P1 and N2 waves, which aligns with the normal maturation process of these responses. Another noteworthy finding in these studies was an increase in the amplitude of the P3 wave and a decrease in its latency.
The observed reductions in latencies and increases in amplitudes of cortical AEPs provide compelling evidence for improved processing of acoustic signals following AT. These positive changes can be attributed to several factors, including heightened neuronal responsiveness to auditory stimuli, enhanced neural synchrony, and strengthened connections within the neural networks involved in auditory processing [9]. The increase in amplitude, particularly in the P3 wave, following AT, indicates improved neural firing synchrony and enhanced attention, and it has also been associated with neural plasticity [33]. The gradual decrease in latencies is likely attributed to the gradual improvement in neural transmission speed, which can be influenced by changes in myelination and an increase in synaptic synchronization in response to auditory stimulation [25].
Among the six studies involving participants with hearing loss, one was a case report, one was a clinical trial without a control group, and four were randomized controlled trials. The pattern of AEP changes was consistent among studies involving populations with normal hearing and those with hearing impairments. In these studies, where participants received hearing aids, there is a potential for bias, as the increased amplitudes of AEPs could be a consequence of improved audibility facilitated by the hearing aids.
In the mentioned studies, researchers endeavored to reduce bias in the results, ensuring that any contrasts in AEP amplitudes between the two groups were attributed to AT. To establish homogeneity between the groups, various measures were implemented in the studies. For instance, participants were selected with an equivalent duration of hearing deprivation prior to receiving hearing aids, matching ranges of aided auditory thresholds, and consistent average daily hours of hearing aid usage.
Eleven studies involved adults in their research population. In adults, alterations in AEPs result from neuroplasticity induced by AT, whereas in children, changes in AEPs also involve neuroplasticity associated with maturation. However, the pattern of AEP changes following AT was similar in both children and adults.
Brainstem and early cortical AEPs correspond to bottom-up auditory processing, while late cortical AEPs, influenced by memory and attention (N2, P3), are associated with top-down auditory processing [15]. Bottom-up processing involves gathering sensory information from the external environment to construct perceptions according to the current sensory inputs [37]. In contrast, top-down processing involves interpreting incoming information based on past knowledge and experiences [38].
The findings from the included studies indicated changes in both brainstem and cortical AEPs after AT. This suggests that assessing these AEPs could be valuable for examining improvements in both top-down and bottom-up auditory processing.
Finally, considering the observed changes in brainstem and cortical AEPs resulting from AT exercises, such as reduced latency and increased amplitude of the waves aligning with the maturation pattern, it can be concluded that this objective electrophysiological evaluation serves as a practical tool to assess the efficacy and validate the chosen method for AT. This is particularly important during early childhood, as it is a critical period for the development of auditory and language systems, as well as communication skills in children. It is hoped that experts in this field will increasingly recognize the value of this tool and utilize it more frequently as part of their practice.
We refrained from conducting a meta-analysis due to the heterogeneity of studies, which included various age groups and diverse AT methods implemented over different durations. One limitation of our study is that we were unable to search certain databases due to lack of access, which could result in missing some relevant studies for our review. Future research endeavors could involve comparing the impact of various AT methods on the neuroplasticity of the CANS by assessing AEPs. Additionally, there is potential to compare the changes in AEPs following AT across different age groups.
Conclusion
Previous studies have reported changes in brainstem and cortical AEPs as a result of AT exercises. These alterations typically lead to an increase in the amplitudes of both brainstem and cortical responses, with the exception of P1 and N2 waves. Additionally, there is a decrease in the latencies of brainstem and cortical AEPs. The outcomes were consistent across both children and adults, as well as among individuals with normal hearing and those with hearing impairments, indicating neuroplasticity in the CANS following AT, potentially enhancing both bottom-up and top-down auditory processing. As a result, it is evident that electrophysiological assessment of brainstem and cortical AEPs is valuable for evaluating CANS alterations and enhanced auditory processing post-AT and this evaluation can validate the efficacy of the chosen AT method.
Availability of data and materials
The datasets used in this study can be obtained from the corresponding author upon making a reasonable request.
References
Nassar AAM, Bassiouny S, Abdel Rahman TT, Hanafy KM (2022) Assessment of outcome measures after audiological computer-based auditory training in cochlear implant children. Int J Pediatr Otorhinolaryngol 160:111217
Castan ATM, Luiz CBL, Gil D (2017) Acoustically controlled auditory training in an adult after traumatic brain injury. Revista CEFAC. 19:126–34
Weihing J, Chermak GD, Musiek FE (2015) Auditory Training for Central Auditory Processing Disorder. Semin Hear 36(4):199–215
Bronus K, El Refaie A, Pryce H (2011) Auditory training and adult rehabilitation: a critical review of the evidence. Global J Health Sci 3(1):49–63
Bettison S (1996) The long-term effects of auditory training on children with autism. J Autism Dev Dis 26(3):361–74
Hayes EA, Warrier CM, Nicol TG, Zecker SG, Kraus N (2003) Neural plasticity following auditory training in children with learning problems. Clin Neurophysiol 114(4):673–84
Moore DR, Amitay S (2007) editors. Auditory training: rules and applications. Seminars in hearing; Copyright© 2007 by Thieme Medical Publishers, Inc., New York
Alonso R, Schochat E (2009) The efficacy of formal auditory training in children with (central) auditory processing disorder: behavioral and electrophysiological evaluation. Braz J Otorhinolaryngol 75(5):726–32
Gopal KV, Schafer EC, Mathews L, Nandy R, Beaudoin D, Schadt L et al (2020) Effects of auditory training on electrophysiological measures in individuals with autism spectrum disorder. J Am Acad Audiol. 31(2):96–104
Alcântara YB, Toledo WWF, de Lima KR, Carnaúba ATL, Chagas EFB, Frizzo ACF (2022) Changes in cortical auditory evoked potentials in response to auditory training in elderly hearing aid users: a pilot study. PLOS Glob Public Health. 2(5):e0000356
Krishnamurti S, Forrester J, Rutledge C, Holmes GW (2013) A case study of the changes in the speech-evoked auditory brainstem response associated with auditory training in children with auditory processing disorders. Int J Pediatr Otorhinolaryngol 77(4):594–604
Chandrasekaran B, Kraus N (2010) The scalp-recorded brainstem response to speech: neural origins and plasticity. Psychophysiol 47(2):236–46
McArthur GM, Atkinson CM, Ellis D (2010) Can training normalize atypical passive auditory ERPs in children with SRD or SLI? Dev Neuropsychol. 35(6):656–78
Bidelman GM (2015) Towards an optimal paradigm for simultaneously recording cortical and brainstem auditory evoked potentials. J Neurosci Methods. 241:94–100
Hall JW (2007) New handbook of auditory evoked responses. Pearson Boston, Boston
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 372:n71
Russo NM, Nicol TG, Zecker SG, Hayes EA, Kraus N (2005) Auditory training improves neural timing in the human brainstem. Behav Brain Res 156(1):95–103
Filippini R, Befi-Lopes DM, Schochat E (2012) Efficacy of auditory training using the auditory brainstem response to complex sounds: auditory processing disorder and specific language impairment. Folia phoniatrica et logopaedica : official organ of the International Association of Logopedics and Phoniatrics (IALP). 64(5):217–26
Ramezani M, Lotfi Y, Moossavi A, Bakhshi E (2021) Effects of auditory processing training on speech perception and brainstem plastisity in adolescents with autism spectrum disorders. Iran J Child Neurol. 15(1):69–77
Melo Â, Mezzomo CL, Garcia MV, Biaggio EPV (2018) Computerized auditory training in students: electrophysiological and subjective analysis of therapeutic effectiveness. Int Arch Otorhinolaryngol. 22(1):23–32
Santos A, Joly-Pottuz B, Moreno S, Habib M, Besson M (2007) Behavioural and event-related potentials evidence for pitch discrimination deficits in dyslexic children: improvement after intensive phonic intervention. Neuropsychologia. 45(5):1080–90
Madruga-Rimoli CC, Sanfins MD, Skarżyński PH, Ubiali T, Skarżyńska MB, Colella Dos Santos MF (2023) Electrophysiological testing for an auditory processing disorder and reading performance in 54 school students aged between 8 and 12 years. Med Sci Monit 29:e940387
Talebi H, Moossavi A, Lotfi Y, Faghihzadeh S (2015) Effects of vowel auditory training on concurrent speech segregation in hearing impaired children. Ann Otol, Rhinol, and Laryngol 124(1):13–20
Silva TR, Dias FAM (2014) Effectiveness of training auditory in plasticity of central auditory system: case report. Revista CEFAC. 16:1361–9
Thabet MT, Said NM (2012) Cortical auditory evoked potential (P1): a potential objective indicator for auditory rehabilitation outcome. Int J Pediatr Otorhinolaryngol 76(12):1712–8
Anderson S, White-Schwoch T, Choi HJ, Kraus N (2014) Partial maintenance of auditory-based cognitive training benefits in older adults. Neuropsychologia. 62:286–96
Tremblay KL, Ross B, Inoue K, McClannahan K, Collet G (2014) Is the auditory evoked P2 response a biomarker of learning? Front Syst Neurosci. 8:28
Tremblay K, Kraus N, McGee T, Ponton C, Otis B (2001) Central auditory plasticity: changes in the N1–P2 complex after speech-sound training. Ear and hearing. 22(2):79–90
Picinini TdA, Sperança S, Pereira LD (2021) Acoustically controlled binaural auditory training with vocal duets: assessment and effectiveness. Clinics 76:e2085
Wisniewski MG, Ball NJ, Zakrzewski AC, Iyer N, Thompson ER, Spencer N (2020) Auditory detection learning is accompanied by plasticity in the auditory evoked potential. Neuroscience Letters. 721:134781
Tremblay KL, Shahin AJ, Picton T, Ross B (2009) Auditory training alters the physiological detection of stimulus-specific cues in humans. Clin Neurophysiol 120(1):128–35
Tremblay KL, Kraus N (2002) Auditory training induces asymmetrical changes in cortical neural activity. J Speech, Lang Hear Res: JSLHR. 45(3):564–72
Gil D, Iorio MCM (2010) Formal auditory training in adult hearing aid users. Clinics. 65(2):165–74
Santos RBF, Marangoni AT, Andrade ANd, Prestes R, Gil D (2014) Effects of auditory training in individuals with high-frequency hearing loss. Clinics 69(12):835–40
Olson AD (2015) Options for Auditory Training for Adults with Hearing Loss. Semin Hear 36(4):284–95
Rochette F, Bigand E (2009) Long-term effects of auditory training in severely or profoundly deaf children. Ann N Y Acad Sci 1169(1):195–8
Gibson JJ (1966) The senses considered as perceptual systems. Houghton Mifflin, Boston
Gregory R (1970) The intelligent eye. Weidenfeld and Nicolson, London
Acknowledgements
All the authors wish to thank all children and their parents who participated in this research.
Funding
The research was not sponsored by any public, commercial, or non-profit entities.
Author information
Authors and Affiliations
Contributions
Conceptualization and supervision: FH; Methodology: AHM and FH; Investigation: AHM and FH; Writing the original draft, review, and editing: AHM and FH.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study did not necessitate ethics approval.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hajimohammadi, A., Heidari, F. Monitoring the Efficacy of Auditory Training through Changes in Brainstem and Cortical Auditory Evoked Potentials: A Systematic Review. Egypt J Otolaryngol 40, 95 (2024). https://doi.org/10.1186/s43163-024-00606-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-024-00606-4