
Abstract
Background
The computed tomography (CT) details of the dimensions of the trachea and the subglottic area are not fully covered in the literature, so it is important to build up a database for the CT measurements of that area. Preoperative details of the trachea are crucial prior to any approach or procedure involving the trachea. So, the aim of this study was to determine the different dimensions of the trachea and subglottic area by computed tomography (CT).
Methods
From 100 CTs of the trachea acquiring the axial images via the multiplanar reformates for all subjects to get the delicate details measuring the transverse diameter (width) and the anteroposterior diameter (depth) of the trachea and subglottic area.
Results
The mean tracheal width was 15.5 ± 2.1 mm (range = 11.5–21.7), and its mean anteroposterior diameter was 16.56 ± 2.77 mm (range = 11.8–25.1), while the mean width of the subglottic area was 15.1 ± 1.86 mm (range = 12.3–21.1), and its mean anteroposterior diameter was 17.75 + 2.76 (range = 12.9–25.2). All the dimensions of the trachea and the subglottic area were found significantly smaller in female than males. There was positive correlation between anteroposterior and transverse diameters of the trachea with the subglottic area with more tendency for more subglottic area dimension with increase tracheal dimensions and vice versa.
Conclusion
The current work updates the CT knowledge about the tracheal and subglottic area dimensions enhancing the surgeons, anesthetist, and radiologists data and orientation of the tracheal dimensions and could aid effective and safe tracheolaryngeal surgery.
Similar content being viewed by others

Background
The trachea is a single tube continues down from of the larynx at the sixth cervical vertebra to the fifth thoracic vertebra where it bifurcates into left and right main bronchi [1].
The dimensions of the trachea are important and should be known because it is crucial for diagnosis, tracheal resection, transplantation, stenting, intubation, and endoscopic operations. Almost studies had investigated and focused on the glottic area [2], the thyroid cartilage [3], the subglottic area [4, 5], and asymmetric measurements [6]. But, some essential dimensions of the trachea and cricoid cartilage are mostly lacking in the literature.
In addition to the variations in the tracheal dimensions between individuals of the same age group, in different age groups and in different gender [7,8,9,10,11,12,13], there is broad variations in the described tracheal dimensions by different authors and in different textbooks from different regions and in different journals [14, 15]. Gray’s anatomy by Standring states that the external transverse diameter of the adult trachea is 20 mm in male and 15 mm in female; lumen has an average transverse diameter of 12 mm [15], while in the textbook Principles of Surgery, Schwartz mentioned that the trachea has a 18 mm anteroposterior diameter and 23 mm transverse diameter [14]. Therefore, there is an increasing demand for measuring the tracheal dimensions in different individuals with real accurate measurement of tracheal dimension in different ethnic groups particularity preoperatively.
Bu, it is hard to measure the trachea dimensions via the fiberoptic evaluation because difficulty to tolerate it with the patient, it does not permit adequate absolute measurements. In addition, some distortion of the fiberoptic image could occur depending on the width of the angle and the distance from the instrument to the tracheal lumen and on the used endoscopic system itself.
Thus, the computed tomography (CT) evaluation appears to be a fast and applicable tool to measure the tracheal dimensions beside CT advantages of identifying the important anatomical landmarks, relations to the surrounding structures, and diagnosis and assessing the disease extension in order to get correct diagnosis, assessment, and a safe and sound surgical outcome.
Hence, the current study was designed to measure the dimensions of the trachea and subglottic area using the CT to add data that could help the tracheal and neck surgery, especially the endoscopic approach and intubation.
Methods
This retrospective work was performed on 100 CTs of trachea at the Otorhinolaryngology departments from January 2022 and June 2023. Informed written consent was obtained from included subjects, and the work was approved by the University IRB.
Patients less than 18 years old, history of surgery or trauma in the trachea, larynx and/or neck, congenital anomalies, and/or malignancies were excluded.
CT scans were done for the enclosed subjects by a 64 slices CT scan (Light speed volume VCT, GE medical system, Milwaukee, WI, USA). The protocol of 64 slices MDCT was performed via a detector width of 0.625 mm, a 1.5-mm sections width, and a 0.5-mm interval reconstructions. 130 kV and 150 mA/sec with 1.5 s scan time.
The subjects were scanned in supine position with axial images covering the trachea and the larynx using a high-resolution algorithmic rule to improve the appearing delicate detail.
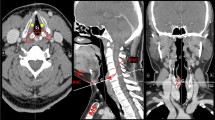
Films were revised in the routine standardized mode to avoid missing any detail. The transverse (width) and the antero-posterior (depth) dimensions were measured along the axial plane for the trachea at the level of the thyroid gland and for the subglottic region at the cricoid cartilage level (Fig. 1).

Measurements of the dimensions of the trachea (A) and the subglottic area (B)
Using the SPSS (version 25; Inc., Chicago, IL, USA), the data was statistically analyzed considering P-value significance when less than 0.05.
Results
Within the included 100 CTs for 48 males (48%) and 52 females (52%), the mean age was 43.4 years (range = 19 to 61).
The mean transverse diameter (width) of the trachea was 15.5 ± 2.1 mm (range = 11.5–21.7) that was significantly more in males (16.67 ± 2.13 mm, range: 12.8 to 21.7) than in females (14.5 ± 1.5 mm, range = 11.5–17.2) (t = 8.3296, p < 0.0001) (Table 1).
The mean anteroposterior diameter of the trachea was 16.56 ± 2.77 mm (range = 11.8–25.1) that was significantly more in males (mean = 17.7 ± 2.4 mm, range = 13.6–25.1) than in females (mean = 15.5 ± 2.5 mm, range = 11.8–22.2) (t = 6.3482, p < 0.0001).
The mean width (transverse diameter) of the subglottic area was 15.1 ± 1.86 mm (range = 12.3–21.1) that was significantly more in males (16.4 ± 2.46 mm, range 13.2–21.1) than in females (14.4 ± 1.7 mm, range = 12.3–17.2) (t = 2.4585, p < 0.0148) (Table 1). The mean anteroposterior diameter of the subglottic area was 17.75 + 2.76 (range = 12.9–25.2) and was significantly more in males (mean = 18.9 + 2.8, range = 14.5–25.2) than in females (mean = 16.7 + 2.25, range = 12.9–20.9) (t = 6.9599, p < 0.0001).
So, all the dimensions of the trachea and the subglottic area were found significantly smaller in female than males (Table 1).
There was strong positive correlation between transverse diameter (width) of the trachea and width of the subglottic area. Thus, there is a tendency for more tracheal width with increase width of the subglottic area (and vice versa) (R = 0.7837, P < 0.00001).
There was also a strong positive correlation between anteroposterior diameter of the trachea and that of the subglottic area (R = 0.6859, P < 0.00001).
Discussion
Measuring the dimensions of the trachea and the subglottic area helps the surgeons and anesthesiologist to conduct some maneuvers like endotracheal intubation and diagnostic and therapeutic endoscopic procedures with skill, less risk, and perfection. Though the studies measuring these tracheal dimensions are sparse [8,9,10, 12] and not correlate the measures with those of subglottic area, and some was done on cadavers [12, 16] that is appeared to be completely different from measurement in the living subjects.
The obtained endoscopic laryngeal images do not give adequate absolute measurement of the subglottic area because of the fairly wide depth of field for laryngeal endoscope with large distances variations between the endoscope to the are through out the examination, causing varied area and distance measuring. There is a well-significant distortion of the images dependent on the angle between the endoscope and the subglottic area beside the distortion of the endoscopic system itself (referred to as barrel shaped distortions) [17]. In addition to effect of the endotracheal tube if under general anaesthesia.
Thus, CT imaging has become one of the gold standards for assessment of the larynx and trachea with good quality images of the cartilages besides its benefit as a standard method for evaluation of most laryngotracheal and neck lesions particularity malignancy and trauma [18]. Thus, the purpose of the current study was to determine the different dimensions and measurements of the trachea and subglottic area by CT.
In the current study, the mean transverse diameter (width) of the trachea was 15.5 ± 2.1 mm (range = 11.5–21.7). The mean anteroposterior diameter (depth) of the trachea was 16.56 ± 2.77 mm (range = 11.8–25.1). The mean width of the subglottic area was 15.1 ± 1.86 mm (range = 12.3–21.1). The mean anteroposterior diameter of the subglottic area was 17.75 + 2.76 (range = 12.9–25.2). In accordance to previous studies, all the dimensions of the trachea and the subglottic area were found significantly smaller in female than in males.
There was a strong positive correlation between width of the trachea and width of the subglottic area. Thus, there is a tendency for more tracheal width with increase width of the subglottic area (and vice versa) (P < 0.00001).
Munguia, in a cadaver study, reported anteroposterior diameter was 18 ± 3 mm (range = 14–25) and transverse diameter was 19 ± 2 mm (range = 16–23) [18]. Mahajan et al., in a cadaver study, reported a mean anteroposterior dimension of 16.07 mm, and a mean transverse diameter was 18.1 mm [19]. The difference from our study mostly attributed to that study was done on cadavers.
Chunder et al. [20] recorded that the external transverse tracheal diameter (external width) was 19.5 mm and anteroposterior diameter (depth) was 13.5 mm at the junction of middle and upper thirds of trachea in male human. These larger measurements because they measure the external diameter while here we measured the internal diameter of the trachea because the tracheal wall has a thickness of 1 to 3 mm.
Solanki and Zarana [21] measured anteroposterior and transverse diameters of trachea on 28 cast of trachea prepared by luminal cast plastination, and reported mean AP diameter was 17 mm (range 11.6–22.5), and mean transverse diameter was 17.8 mm (range 14.2–21 mm). Hampton et al. [21] reported that transverse diameter of trachea was 17.5 ± 2.6 mm.
The variation in dimensions in the current study from previous studies may be attributable to genetic, culture, or ethnic differences and environmental or geographical alteration. Alterations may happen in the tracheal dimensions such as tracheomalacia or tracheobronchomegaly where there is tracheal widening or in tracheobronchopathia where there is tracheal narrowing [19]. So, the data of these human trachea measurements is really helpful in such conditions as well as in conduction of endotracheal intubation in both therapeutic and diagnostic applications.
The absolute dimensions of the trachea and the subglottic area could be measured by CT with advantages of easy, computerized, and accurate measurements without admission of any instruments in the airway that may disturb it or cause discomfort to the patients and without need to apply any local anesthesia or any procedure through the airway.
Knowledge of tracheal and subglottic measurements has an important meaning for surgeon and anesthetist. However, a simple and reliable method allowing collecting reference values and measurements for the trachea and the subglottic area has not yet been fully described.
To deal with resection and reconstruction of the subglottic area and tracheobronchial tree, measuring the dimensions of these areas is very crucial. In addition, knowledge of diameters of trachea and the subglottic area aids the clinician selecting the suitable tracheostomy tube size in emergency situations and in correct choice of endotracheal tube. Accurate anatomical variations knowledge is necessary to know pathophysiology, diagnosis, and treatment of various airway diseases [19]. The CT gives accurate measurements of the trachea and the subglottic areas in a fast and easy way beside the advantages of clear details of any tracheolaryngeal trachea and neck anatomical variations or pathological lesions.
Conclusion
The current work updates the CT knowledge about the tracheal and subglottic area dimensions enhancing the surgeons, anesthetist, and radiologists’ data and orientation of the tracheal dimensions and could aid effective and safe tracheolaryngeal surgery.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CT:
-
Computed tomography
References
Drevet G, Conti M, Deslauriers J (2016) Surgical anatomy of the tracheobronchial tree. J Thorac Dis 8(Suppl 2):S121–S129
Hirano M, Kurita S, Kiyokawa K, Sato K (1986) Morphological study in excised human larynges. Ann Otol Rhinol Laryngol 95:576–581
Friedrich G, Kainz J (1988) Morphometrie des kehlkopfes an horizontalschnitten. Laryngol Rhinol Otol 67:269–274
Carter DR, Meyers AD (1978) The anatomy of the subglottic larynx. ORL J Otorhinolaryngol Relat Spec 86:279–283
Randestad A, Lindholm C, Fabian P (2000) Dimensions of the cricoid cartilage and the trachea. Laryngoscope 110(11):1957–1961
Hirano M, Kurita S, Yukizane K, Hibi S (1989) Asymmetry of the laryngeal framework: a morphologic study of cadaver larynges. Ann Otol Rhinol Laryngol 98:135–140
Moore KL, Dalley AF, Agur AMR (2014) In: Clinically oriented anatomy, 7th edn. Lippincott Williams and Wilkins, Philadelphia, p 104
Shaik Z, Ramulu V, Hanimann KS (2016) A study on anatomical dimensions of bronchial tree. Int J Res Med Sci 4(7):2761–2765
Kim IKS, Lim JM, Chai OH, Han EH, Kim HT, Song CH (2015) Morphomettric study of trachea in Korean. Korean J Phys Anthropol 28(4):185–195
Sharma N, Khan GA, Pandit R (2017) A cadaveric study of length of trachea in Nepalese population of various age groups. J Univ Coll Med Sci 5(1):17–21
Kamel KS, Lau G, Stringer MD (2009) In vivo and in vitro morphometry of the human trachea. Clin Anat 22:571–579
Munguia DA (2011) Tracheal dimensions in the Mexican population. Cir 79(6):505–510
Wani TM, Buchh B, AlGhamdi FS, Jan R, Tumin D, Tobias JD (2018) Tracheobronchial angles in children: three dimensional computed tomography based measurements. Paediatr Anaesth 28(5):463–467
Schwartz SI, Rusch VW, Ginsberg RJ (1999) Chest wall, pleura, lung and mediastinum. Principles of Surgery, 7th edn. McGraw-Hill, p 764
Standring S (2008) Gray’s anatomy, 40th edn. W.B. Saunders company, Philadelphia, pp 989–1007
Peppard R, Bless D (1990) A method for improving measurement reliability in laryngeal videostroboscopy. J Voice 4:280–285
Clarós P, Sobolewska AZ, Domenech-Claros A, Claros-Pujol A, Pujol C, Claros A (2019) CT-based morphometric analysis of professional opera singers’ vocal folds. Journal of Voice, J Voice 33(4):583.e1-583
Chunder R, Nandi S, Guha R, Satyanaryana N (2010) A morphometric study of human trachea and principal bronchi in different age groups in both sexes. Nepal Med Coli J 12(4):207–214
Mahajan S, Mahajan A, Lalit M, Verma P (2022) Morphometry of adult human trachea and its clinical implications: a cadaveric study in Northern India. J Clin Diagn Res 16(7):AC01–AC05
Solanki S, Zarana A (2015) Morphometric analysis of human trachea in adult Gujrat region by luminal cast plastination. J Res Med Den Sci 3(3):235–237
Hampton T, Armstrong S, Russell WJ (2000) The left main bronchus. Anaesth Intensive Care 28:540–542
Acknowledgements
None.
Funding
The authors declare no financial support or interest to this study.
Author information
Authors and Affiliations
Contributions
MWE suggested and developed the research idea; reviewed literature; interpretation, and analysis of collected data; tabulated data; wrote the manuscript; assisted in preparing the tables and figure; and approved the submitted version. AE took the IRB approval; helped in keeping the record of patients’ information, interpretation, and analysis of collected data; assisted in writing methods and revising the written manuscript; prepared the tables, and approved the submitted version. MO reviewed literature; assisted in interpretation and analysis of collected data; assisted in preparing the tables; and approved the submitted version. MAM developed the research idea, reviewed the written manuscript, assisted in preparing tables, kept the record of patients’ information, prepared tables, revised the manuscript critically for important intellectual content, and approved the submitted version. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed written consent was signed by all subjects to share in the study after explanation of its purposes. Zagazig University Hospitals IRB approval was obtained.
Consent for publication
The patients included in this research gave written informed consent to publish the data contained within this study. No patient was less than 16 years old were included in this study.
Competing interests
Dr Mohammad Waheed El-Anwar is a co-author of this study and a Co-Editor of the journal. He has not been involved in handling this manuscript during the review process. The rest of the authors have no conflict of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Anwar, M.W., El-Hussiny, A., Osman, H. et al. Tracheal and subglottic dimensions: a computed tomography cross section study of adult population. Egypt J Otolaryngol 40, 25 (2024). https://doi.org/10.1186/s43163-024-00588-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-024-00588-3