
Abstract
Persistent postural-perceptual dizziness (PPPD) is a chronic functional vestibular disorder, not a structural or psychiatric condition, presented by one or more dizziness, unsteadiness, or non-spinning vertigo symptoms. These symptoms will worsen with upright posture, movements, and exposure to complex visual stimuli. PPDD may be precipitated by disorders that impair balance or induce vestibular symptoms, such as peripheral or central vestibular diseases, other medical conditions, or psychological illness The exact pathophysiological mechanism is unknown, and it might result from functional adjustments to the postural control systems—alterations in the way multisensory information are processed or the integration of spatial orientation and danger perception in the cortex. PPPD is usually associated with co morbidities like anxiety. Subtypes of PPPD are phobic postural vertigo, space and motion discomfort, visual vertigo, and chronic subjective dizziness. PPPD is diagnosed according to the diagnostic criteria of the Barany society. Physical examination and diagnostic investigation are not pathognomic to PPPD. Treatment approaches include patient counseling, vestibular rehabilitation therapy, cognitive behavioral therapy, and medications.
Similar content being viewed by others

Background
Persistent postural-perceptual dizziness (PPPD) is a syndrome that ties together important elements of chronic subjective dizziness (CSD), phobic postural vertigo (PPV), and related conditions. It represents a pervasive chronic malfunction of the brain and vestibular system. The illness is characterized as a long-term maladaptation to vestibular, physiological, or psychological issues that precipitated symptoms of vestibular dysfunction [1]. This disorder is named according to the key diagnostic criteria which are chronic dizziness, instability, and non-spinning vertigo that become worse with postural challenges and perceptual sensitivity to space-motion cues [2]. PPPD affects the daily life of the patients due to cognitive and emotional load resulting from self-disruption, perceived handicapping, and fears from the future; these factors should be identified as it affect the rehabilitation; and specific psychological support may be the way to successful treatment and better outcome [3].
Historical view
In the nineteenth century, three syndromes of dizziness and distress in moving environments associated with autonomic reactions, and fear and evading of provocative conditions were described by German physicians which are Platzschwindel (vertigo in a plaza or square), Platzangst (fear in a plaza or square), and Die Agoraphobie (fear of the marketplace). In the early twentieth century, as otology, neurology, and psychiatry became a separate specialty, Platzschwindel and Platzangst are no longer used, and agoraphobia was included in the psychiatric disorders. A century later, various syndromes of disorientation and motion sensitivity were described as supermarket syndrome, visually induced motion symptoms, and space phobia [4].
Epidemiology
The second most common diagnoses in dizziness clinics are (PPV) or (CSD), two conceptual forerunners of PPPD that account for about 20% of all patient presentations [5]. Long-term 3–12 months of follow-up studies for patients who experienced an acute or episodic attack of acute vestibular disease either with BPPV or vestibular neuritis showed that one patient out of four will experience persistent-postural instability like that seen in PPPD. Thus, PPPD incidence in this situation is substantially higher than is typically supposed [4]. According to Yang et al.’s findings [6], middle-aged females are more likely to develop PPPD.
Pathophysiological mechanisms
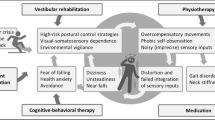
PPPD is brought on by attacks of vertigo or instability with vestibular, neurological, or psychological causes. These stimuli cause the overuse of visual cues for spatial orientation as well as the usage of high-demand postural control techniques. The adoption of high-demand methods in everyday posture, gait, and gaze control conditions evolves as a result of high levels of worry and attention surrounding the acute physical symptoms [7]. Postural control is preserved through interaction between three systems (vestibular, ocular, and somatosensory). When one of them is compromised, the other(s) takes over through processes referred to as sensory reweighting. To compensate for impaired vestibular function following acute vestibular insults, postural control quickly switches to rely on visual and/or somatosensory input [8, 9]. This switch is beneficial at first but should return to normal after the precipitant is removed or compensation has occurred. However, in PPPD patients with a high level of vigilance, this scenario persists resulting in a case of overreliance on the visual and somatosensory inputs to keep the postural stability. Consequently, this leads to exaggerated reactions to visual cues and physical movements [10]. The most frequent provocations of PPPD symptoms are ordinary situations that could be viewed as unpleasant or hazardous, such standing, walking, watching traffic, or sitting at a crowded restaurant. If PPPD patients are distracted, symptoms may momentarily lessen or briefly flare up without any apparent cause [1]. Even though the previously mentioned precipitating factors are responsible for the bulk of PPPD cases, on occasion, cases appeared to start without a clear cause which is confusing with neurodegenerative disorders [11]. Anxiety-related personality features and a family history of anxiety disorders may be potential risk factors for the development of PPPD [4]. In comparison to the control group, Yan et al. [6] found that PPPD had greater levels of anxiety, sleep problems, and neurotism.
Diagnostic criteria of PPPD
Based on the duration of symptoms, the international classification of vestibular disorders classifies illnesses and disorders as acute, episodic, or chronic, and PPPD may persist for months to years, so it is a chronic vestibular disfunction. PPPD is diagnosed by Bárány Society diagnostic criteria A-E below. The diagnosis can only be made if all five requirements are fulfilled [4].
-
A.
For 3 months or longer, the majority of days are characterized by dizziness, unsteadiness, or non-spinning vertigo.
-
1.
Symptoms may be prolonged in time and fluctuate in severity.
-
2.
It is not necessary for symptoms to be present throughout the day.
-
1.
-
B.
Persistent symptoms can happen without a clear cause, but can be provoked by standing or walking, moving actively or passively, exposure to complex visual stimuli.
-
C.
Disorders that induce vertigo, unsteadiness, dizziness, or balance issues, such as acute, episodic, or chronic vestibular diseases, other neurologic or medical conditions, or psychological distress, might trigger the disorder.
-
D.
Symptoms cause significant distress or functional impairment.
-
E.
Symptoms are not better explained by another disorder.
The following notes should be taken into consideration: (1) basic symptoms of PPPD are dizziness, unsteadiness, and internal or external non-spinning vertigo. (2) Patients should experience symptoms more than 15 days out of every 30 days. Most affected people have symptoms daily or almost daily. As the day goes on, symptoms usually get worse. (3) PPPD patients experience vestibular symptoms with very brief free intervals, momentary flare-ups of symptoms may happen spontaneously or in response to movement, and once the illness has fully manifested, symptoms persist without precipitating factors (4). Red flags in the diagnosis of PPPD commonly have a relatively acute onset which is related to the precipitating conditions. In most cases, patients experience transition of symptoms from acute to chronic symptoms, for example, the transition from acute rotatory vertigo to of vestibular neuritis to chronic unsteadiness of PPPD with no symptom free interval. When episodic precipitating events, such as vestibular migraine, are present, PPPD symptoms could disappear for a while before returning when the triggering event recurs, before settling into a predictable pattern.
Diagnostic dilemma occurs when the precipitating conditions are insidious disorders such as degenerative diseases of the nervous or vestibular systems, prospective follow-up and careful serial evaluation are needed to complete the diagnosis [1]. Another potential pitfall is the presence of comorbid disorders. The presence of other disorders, e.g., structural, and psychiatric disorders does not rule out PPPD. This disorder can co-occur with many of the conditions listed in its differential diagnosis, for instance, vestibular migraine and BPPV. They may also coexist with PPPD, causing repeated vertigo bouts in addition to the ongoing symptoms of PPPD. Functional dizziness can occur in structural gait abnormalities as Parkinson’s disease. Sensitivity to visually challenging settings when patients are seated clearly implies PPPD in this case [4]. Also panic and anxiety disorders can co-exist with PPPD as a cause or sequalae. They may also occur prior to the onset of PPPD without causing dizziness, but they get worse if PPPD is brought on by another ailment. In order to distinguish between overlapping etiologies, the timing of the vestibular symptoms and their accompanying symptoms should be taken into account [1].
Co-morbidities
Waterston et al. [11] reported vestibular abnormalities in the form of unilateral vestibular hypofunction and isolated otolith disorders in nearly half of PPPD patients. Vestibular migraine was the most frequent related vestibular disorder (25%); this finding might be explained by the impaired sensory processing and visual sensitivities in both PPPD and vestibular migraine. Psychological disorders such as anxiety and post-traumatic stress were reported in 42% of cases which is considered a high incidence. Anxiety may be a predisposing factor or a complication of PPPD [11]. Obsessive compulsive personality trait is usually observed PPV [12].
Subtypes of PPPD
PPV [13], CSD [14], visual vertigo (VV) [15], and space and motion discomfort (SMD) [16] may represent different conditions on a single, multifaceted clinical entity, or they may provide insight into potentially distinguishable PPPD subtypes (e.g., visually dominant subtype, posturally dominant subtype) [4]. These conditions share the same diagnostic criteria of PPPD with some differences between them.
-
1. PPV: a subtype of functional dizziness distinguished by dizziness and subjective imbalance during stance and gait but objectively normal neuro-otological testing. In PPV, despite the patients’ subjective perception of an imbalance, functional but insufficient postural control mechanisms are used to maintain balance. Changing postural symptoms are accompanied by fleeting perceptions of movement. Restricted standing mode, high-frequency postural sway, and musculoskeletal stiffness are just a few of the postural control modifications that occur as a result of anxiety-related increases in attention to posture control. Patients may exhibit symptoms of anxiety, depression, or obsessive–compulsive behavior [13].
-
2. CSD: persistent unsteadiness and non-vertiginous dizziness with motion sensitivity and visually challenging environments. CSD is similar in many ways to PPV but with more focus on physical rather than psychological symptoms [14]. Chronic symptoms usually last throughout the day and are aggravated by motion stimuli [4].
-
3. VV was recognized in patients after acute central or peripheral vestibular dysfunction with sensation of unsteadiness or dizziness in visually challenging situations, patients recover from the acute vestibular insult, but VV persists. VV results from the visual vestibular mismatch after the vestibular insult, patients develop visual dependence for spatial orientation [15].
-
4. SMD is a result of apprehension about spatial orientation and increased awareness of motion that is triggered in affected individuals by active or passive movement in visually challenging environment, e.g., grocery store, moving, or patterned objects (e.g., striped curtains [16]). Subjects with SMD usually have anxiety and somatosensory reliance for postural control [4].
Diagnosis
Clinical diagnostic criteria are used to make the diagnosis of PPPD. There are no pathognomonic signs of PPPD seen through a physical examination, laboratory test, or diagnostic imaging. Information from physical exams and clinically recommended diagnostic tests is helpful in deciding if PPPD is the most appropriate diagnosis either alone or in association with other disorders, when all PPPD criteria are met, positive examination or testing results indicate the presence of a precipitating condition or comorbidities [17]. Self-reported measures can help in the diagnosis and assessment of the severity of PPPD symptoms such as the Niigata PPPD Questionnaire (NPQ), which is a validated questionnaire to assess the severity of PPPD [18], the Situational Characteristics Questionnaire (SCQ) is used to diagnose VV [18]. Other measures that assess the psychological condition can be used like Hospital Anxiety and Depression scale, questionnaires to assess the perceived disability such as Dizziness Handicap Inventory also can be used. These measures can also be used in the follow-up of PPPD patients after vestibular rehabilitation and cognitive behavioral therapy. Although vestibular investigations are not necessary to determine the diagnosis of PPPD, they can be used to rule out or identify other underlying vestibular disorders. Many patients with primary anxiety disorders or vestibular migraine may have unremarkable findings in vestibular tests [11]. However, Söhsten et al. [19] reported that PPPD patients had significantly poorer sensory organization (SOT) scores in posturography than normal individuals on conditions 2–6, which may be explained by the abnormal postural strategies, somatosensory, and visual dependence that may occur in PPPD. In a study by Yagi et al. [20] on PPPD, no significant abnormalities were noted in conventional vestibular tests such as VEMP and upright subjective visual vertical (UP-SVV) test, and abnormalities were only reported in head tilt subjective visual vertical (HT-SVV) test. It is possible that PPPD patients’ hypersensitivity to neck somatosensory stimulation is the cause of their greater Head-Tilt Perception Gain (HTPG) levels. This theory would explain the traits of PPPD sufferers whose symptoms are aggravated by active or passive movement as perceived by vestibular, ocular, and somatosensory inputs [10]. Most recent, neuroimaging studies were done to investigate the central mechanism of PPPD. Gray matter (GM) in the cerebellum, multisensory vestibular cortices, visual cortex, and anxiety-related network was structurally altered, according to structural neuroimaging [21, 22]. Functional imaging during particular tasks or at rest has also shown abnormal functional activation and connectivity in the previously mentioned areas and in the parieto-insular vestibular cortex (PIVC) as well [22,23,24,25,26,27]. These studies offer strong proof of anatomical and functional abnormalities in the multimodal vestibular cortex in PPPD.
Differential diagnosis
The differential diagnosis of PPPD according to Stab et al. [4] includes (1) chronic sequelae of acute precipitants, such as uncompensated vestibulopathies after vestibular neuritis; (2) recurrent attacks of episodic precipitants, e.g., episodic vestibular disorders such as vestibular migraine; (3) ongoing manifestations of chronic precipitants (e.g., anxiety and depressive disorders); (4) chronic vestibular syndromes, e.g., bilateral vestibulopathy, neurodegenerative disorders; (5) post-concussive syndrome and autonomic disorders, e.g., postural orthostatic tachycardia syndrome that cause chronic dizziness; and (6) medical or psychiatric disorders that cause persistent unsteadiness or dizziness, and side effects of medications.
Treatment
PPPD may co-exist with other disorders that cause dizziness [1], and the co-existing balance disorders (e.g., BPPV, vestibular migraine) should be addressed either before or concurrently with PPPD therapy. A special concern should be attained to migraine. As vestibular rehabilitation may worsen migraine and/or PPPD symptoms which in turn will cause failure of the rehabilitation therapy. So, specialists recommended using prophylactic agents in low levels to treat migraine in patients requiring vestibular rehabilitation even if the migraine is not the main cause of the vestibular dysfunction. For expediting recovery from the maladaptive cycle that exacerbates PPPD, psychotherapies and other treatments that target anxiety-related symptoms and lifestyle-related disorders, like adequate sleep hygiene, physical activity, and a balanced diet, may be appropriate [28]. Treatment goal is symptom reduction toward handicap reduction and normalization of daily life. Accepting some amount of dizziness and the possibility of falling is necessary to prevent re-entry into cycles of fear and avoidance [29]. Treatment options for PPPD include patient counselling, vestibular rehabilitation, medications, and cognitive behavioural therapy (CBT) [1].
Counseling
First, patients must be informed about their condition, as understanding of the condition is crucial especially in functional disorders; persistent fears of missed disease, e.g., neurological disorder, tumors, or catastrophic consequences, e.g., fall and injury, can hinder recovery. Patients should be educated about the diagnosis of PPPD, possible underlying mechanisms, the maladaptive behaviours, the role of psychological condition, and treatment lines [29].
Vestibular rehabilitation
Patients should be encouraged to continue vestibular rehabilitation exercises parallel with other lines of treatment to improve balance and mobility, as well as to reduce motion-induced dizziness [11] through the use of habituation exercises and relaxation techniques. There are many different types of exercises that can be utilised in vestibular rehabilitation, from general activities like walking programmes to more specialized exercises like those employed in VV rehabilitation in the form of simulators, head mounted displays, and exercises employing patterned or stripped backgrounds [30]. Functional gait disorders, which can occasionally be brought on by PPPD, call for specialised exercises that combine distraction (dual task) methods with exercises that gradually restore normal gait, such as running and sliding [31]. Relaxation exercises such as breathing exercises and mindfulness can be used to aid in the desensitization of the dizziness-alert-anxiety cycle response [32]. Physical activities, (especially habituation and relaxation strategies), are likely to be beneficial for many PPPD patients, especially when combined with patient education and/or CBT [11]. Exposure to dynamic virtual-reality surroundings should be regarded as a useful supplement to vestibular rehabilitation programs for patients with peripheral vestibular and VV symptoms. Virtual reality technology provides long-term benefits and helps PPPD through controlled and flexible immersion [33].
Medications
Along with CBT, antidepressant medications such as tricyclic antidepressants, selective serotonin reuptake inhibitors (SSRIs), and serotonin and norepinephrine reuptake inhibitors, should be considered [11]. SSRIs alter and modify neural conduction via anxiety circuits and central vestibular neurons. With proper SSRI use, a reduction in symptoms can be obtained in up to 70% of individuals after approximately three months of treatment [34].
Cognitive behavioral therapy
CBT main goal is to refocus subjects on meaningful and valuable activities. This frequently entailed accepting a certain level of dizziness and anxiety. With the advent of the COVID-19 pandemic, CBT can be carried out via video telemedicine [11]. The components that should be included in the treatment program according to Popkiro et al. [29] are the following:
-
1. Psychoeducation: this fundamental component of CBT is critical and should begin as soon as the diagnosis is made, provided in introductory sessions that explain important aspects of pathophysiology. Patients may benefit from brochures, information fliers, or websites. In-session behavioral experiments and activities can also be used to explain characteristics like distraction.
-
2. Self-observation with guidance: the first step to break out the maladaptive behavioral cycles is self-observation with guidance on the physical, emotional, and psychosocial aspects. Patients are instructed on how to recognize abnormal postural control, e.g., rigid posture, visual reliance, body sway, and desensitization exercises can be used to reduce these behaviors.
-
3. Recognizing and analyzing one’s emotional and cognitive responses to dizziness can aid in lowering the level of fear arousal and pessimistic thinking. Relaxation techniques can be used for this purpose.
-
4. Psychosocial elements like social discomfort, avoidance, and safety attitudes should be recognized and assessed. These concerns can be addressed by exposure treatment in a variety of settings with a therapist or in group sessions. Waterston et al. [11] reported improvement in PPPD symptoms, handicap, avoidance behavior, and anxiety after CBT.
Conclusion
PPPD is a chronic functional vestibular disorder, not a structural or psychiatric condition, presented by one or more dizziness, unsteadiness, or non-spinning vertigo symptoms. These symptoms will worsen with upright posture, movements, and being exposed to challenging visual stimuli. The exact pathophysiological mechanism is unknown PPPD is diagnosed according to the diagnostic criteria of the Baranay society. Physical examination and diagnostic investigation are not pathognomonic to PPPD. Treatment approaches include patient counseling, vestibular rehabilitation therapy, cognitive behavioral therapy, and medications.
Availability of data and materials
Not applicable.
References
Popkirov S, Staab J, Stone J (2018) Persistent postural-perceptual dizziness (PPPD): a common, characteristic and treatable cause of chronic dizziness. Pract Neurol 18(1):5–13
World Health Organization, International Classification of Diseases, 11th edition beta draft version (ICD-11 beta), definition of persistent postural-perceptual dizziness. http://id.who.int/icd/entity/2005792829. Accessed 20 Jun 2015
Sezier A, Saywell N, Terry G, Taylor D, Kayes N (2019) Working-age adults’ perspectives on living with persistent postural-perceptual dizziness: a qualitative exploratory study. BMJ Open 9(4):e024326
Staab J, Eckhardt-Henn A, Horii A, Jacob R, Strupp M, Brandt T et al (2017) Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): consensus document of the committee for the Classification of Vestibular Disorders of the Bárány Society. J Vestib Res 27(4):191–208
Dieterich M, Staab JP, Brandt T (2016) Functional (psychogenic) dizziness. Handb Clin Neurol 139:447–68
Yan Z, Cui L, Yu T, Liang H, Wang Y, Chen C (2017) Analysis of the characteristics of persistent postural-perceptual dizziness: a clinical-based study in China. Int J Audiol 56(1):33–37
Dieterich M, Staab J (2017) Functional dizziness: from phobic postural vertigo and chronic subjective dizziness to persistent postural-perceptual dizziness. Curr Opin Neurol 30(1):107–113
Cousins S, Cutfield N, Kaski D, Palla A, Seemungal B, Golding J et al (2014) Visual dependency and dizziness after vestibular neuritis. PLoS ONE 9(9):e105426
Okumura T, Horii A, Kitahara T, Imai T, Uno A, Osaki Y et al (2015) Somatosensory shift of postural control in dizzy patients. Acta Otolaryngol 135(9):925–930
Staab JP (2020) Persistent postural-perceptual dizziness. In: Seminars in Neurology, Thieme Medical Publishers 40:130–137
Waterston J, Chen L, Mahony K, Gencarelli J, Stuart G (2021) Persistent postural-perceptual dizziness: precipitating conditions, co-morbidities and treatment with cognitive behavioral therapy. Front Neurol 12:795516
Wuehr M, Pradhan C, Novozhilov S, Krafczyk S, Brandt T, Jahn K et al (2013) Inadequate interaction between open-and closed-loop postural control in phobic postural vertigo. J Neurol 260:1314–1323
Brandt T (1996) Phobic postural vertigo. Neurology 46(6):1515–1519
Staab JP (2012) Chronic subjective dizziness. CONTINUUM: Lifelong Learning in Neurology 18(5):1118–1141
Bronstein A (1995) Visual vertigo syndrome: clinical and posturography findings. J Neurol Neurosurg Psychiatry 59(5):472–476
Jacob R, Lilienfeld S, Furman J, Durrant J, Turner S (1989) Panic disorder with vestibular dysfunction: further clinical observations and description of space and motion phobic stimuli. J Anxiety Disord 3(2):117–130
Teh CS, Iffah S, Prepageran N (2022) Persistent postural-perceptual dizziness: A multispecialty survey of clinician awareness and practices in Malaysia. Indian J Otol 28(1):32–40
Yagi C, Morita Y, Kitazawa M, Nonomura Y, Yamagishi T, Ohshima S et al (2019) A validated questionnaire to assess the severity of persistent postural-perceptual dizziness (PPPD): the Niigata PPPD questionnaire (NPQ). Otol Neurotol 40(7):e747
Söhsten E, Bittar RS, Staab J (2016) Posturographic profile of patients with persistent postural-perceptual dizziness on the sensory organization test. J Vestib Res 26(3):319–326
Yagi C, Morita Y, Kitazawa M, Nonomura Y, Yamagishi T, Ohshima S et al (2021) Head roll-tilt subjective visual vertical test in the diagnosis of persistent postural-perceptual dizziness. Otol Neurotol 42(10):e1618
Wurthmann S, Naegel S, Steinberg B, Theysohn N, Diener H, Kleinschnitz C et al (2017) Cerebral gray matter changes in persistent postural perceptual dizziness. J Psychosom Res 103:95–101
Cao Z, Liu X, Ju Y, Zhao X (2022) Neuroimaging studies in persistent postural–perceptual dizziness and related disease: a systematic review. J Neurol 269(3):1225–1235
Indovina I, Riccelli R, Chiarella G, Petrolo C, Augimeri A, Giofrè L et al (2015) Role of the insula and vestibular system in patients with chronic subjective dizziness: an fMRI study using sound-evoked vestibular stimulation. Front Behav Neurosci 9:334
Lee J, Lee E, Kim JS, Lee Y, Jeong Y, Choi B et al (2018) Altered brain function in persistent postural perceptual dizziness: a study on resting state functional connectivity. Hum Brain Mapp 39(8):3340–3353
Li K, Si L, Cui B, Ling X, Shen B, Yang X (2020) Altered spontaneous functional activity of the right precuneus and cuneus in patients with persistent postural-perceptual dizziness. Brain Imaging Behav 14:2176–2186
Li K, Si L, Cui B, Ling X, Shen B, Yang X (2020) Altered intra-and inter-network functional connectivity in patients with persistent postural-perceptual dizziness. Neuroimage Clin 26:102216
Na S, Im J, Jeong H, Lee E, Lee T, Chung Y et al (2019) Cerebral perfusion abnormalities in patients with persistent postural-perceptual dizziness (PPPD): a SPECT study. J Neural Transm 126:123–129
Seemungal BM, Passamonti L (2018) Persistent postural-perceptual dizziness: a useful new syndrome. Pract Neurol 18(1):3–4
Popkirov S, Stone J, Holle-Lee D (2018) Treatment of persistent postural-perceptual dizziness (PPPD) and related disorders. Curr Treat Options Neurol 20:1–11
Pavlou M, Lingeswaran A, Davies R, Gresty M, Bronstein A (2004) Simulator based rehabilitation in refractory dizziness. J Neurol 251:983–995
Nielsen G, Stone J, Matthews A, Brown M, Sparkes C, Farmer R et al (2015) Physiotherapy for functional motor disorders: a consensus recommendation. J Neurol Neurosurg Psychiatry 86(10):1113–1119
Thompson K, Goetting J, Staab J, Shepard N (2015) Retrospective review and telephone follow-up to evaluate a physical therapy protocol for treating persistent postural-perceptual dizziness: a pilot study. J Vestib Res 25(2):97–104
Zaidi S, Shafiabady N, Beilby J (2022) Persistent postural-perceptual dizziness interventions—an embodied insight on the use virtual reality for technologists. Electronics 11(1):142
Staab J, Ruckenstein M, Amsterdam J (2004) A prospective trial of sertraline for chronic subjective dizziness. Laryngoscope 114(9):1637–1641
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
A.S proposed the idea, collected and interpreted the data, and had written the original draft. N.N contributed to writing and reviewing the manuscript. The authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Moaty, A.S., Nada, N. Updates on persistent postural-perceptual dizziness (PPPD): a review article. Egypt J Otolaryngol 39, 131 (2023). https://doi.org/10.1186/s43163-023-00497-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-023-00497-x