
Abstract
Background
Tinnitus is the perception of sound when there is no external sound stimulus. Individuals with tinnitus may have altered neurological system corresponding to the auditory pathway. Therefore, central auditory processing abilities, which rely on the central auditory pathway, may be affected. This study reviewed the published studies regarding the impact of tinnitus on central auditory processing abilities.
Main text
A total of 3087 studies were identified, of which 18 fulfilled the eligibility criteria and were included in the review. The included studies scored good or fair in the quality assessment checklist. The review showed that individuals who had tinnitus with normal hearing sensitivity performed poorly on temporal resolution tests, speech perception in noise, localization, and auditory memory. However, temporal patterning and dichotic tests were not shown to be affected by tinnitus.
Conclusion
The audiologists involved in tinnitus assessment are recommended to include central auditory processing tests in routine evaluation for the early diagnosis and intervention for subjects with tinnitus.
Similar content being viewed by others
Background
Tinnitus is the perceived sensation of sound in the absence of a corresponding external acoustic stimulus [1]. Tinnitus sensations are usually acoustic, such as a buzzing, hissing, or ringing sound [2]. Tinnitus can be unilateral or bilateral, sometimes described as emerging within the head. The perceived sensation can be intermittent or have a pulsatile character. In the “neurophysiological model” of tinnitus [3], tinnitus results from the abnormal processing of a signal generated in the auditory system. This abnormal processing occurs before the signal is perceived centrally. This may result in “feedback,” whereby the annoyance created by the tinnitus causes the individual to focus increasingly on the noise, exacerbating the annoyance, and so a “vicious cycle” develops.
Main text
Studies have shown that tinnitus can impair various central auditory processing abilities [4,5,6,7,8,9,10,11,12,13,14,15]. Central auditory processing is complex and difficult to comprehend in detail. Central auditory processing disorder [(C)APD] is the name given to difficulties in the perceptual processing of auditory information in the central nervous system [16]. (C)APD covers a range of disorders that affect auditory analysis, although, typically, patients have normal auditory threshold sensitivity but difficulty identifying speech in background noise [17]. The deficits can be measured in terms of sound source localization, level discrimination; temporal patterning; temporal aspects (such as temporal integration, temporal discrimination, such as gap detection, temporal ordering/sequencing of rapid events, and temporal masking); and skill in word recognition in the presence of competing acoustic signals (such as dichotic listening) or understanding degraded speech [16]. A detailed assessment of the various processes that may be affected in individuals with (C)APD requires a comprehensive case history along with an appropriate test battery.
The auditory processing is affected by both auditory factor and cognitive factors [18]. Tinnitus is an auditory factor that can affect auditory processing [19]. Studies have shown that tinnitus affects speech perception in noise (SPIN) [6,7,8, 10, 14], temporal processing [5, 8, 9, 11, 20, 21], localization [22], working memory [5, 8, 9, 11, 20, 21], and even in those with normal hearing. A higher level of central auditory processing is needed for SPIN, temporal processing, auditory discrimination, etc. [4]. Speech comprehension difficulties are among the most common causes of tinnitus-related handicaps in many patients [23].
The cerebral imagery techniques have indicated abnormal activation in cortical structures, abnormal cortical excitation, and evidence for functional reorganization in tinnitus patients with normal hearing sensitivity [24]. This might affect central auditory processing abilities. However, the outcome of the studies is mixed, wherein few studies have shown a negative impact of tinnitus on auditory processing [7, 20, 21, 23], and few studies have shown no impact of tinnitus on auditory processing [15, 25, 26]. Therefore, there is a need to systematically review the studies on tinnitus’s effect on central auditory processing, which can help the clinician to modify assessment protocol in tinnitus individuals. Thus, the present study aimed to review the studies on tinnitus’s potential impact and interference on central auditory processing skills.
Methods
The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [27].
Eligibility criteria
The literature search was done for articles published after 2002. Experimental studies were chosen for systematic review, and the systematic reviews were excluded. The population of interest was individuals with tinnitus with normal hearing sensitivity. Articles that included populations with tinnitus existing with other audiological complaints were excluded. The experimental group should have at least 10 participants, with or without the control group. Articles published in any other language other than English language were not included in the review process.
Search strategy
The electronic databases, PubMed, Google Scholar, and the institutional repository of All India Institute of Speech and Hearing, were searched. The keyword used was as follows: 'tinnitus,' 'ringing in the ear,' 'buzzing in the ear,' 'humming in the ear,' 'auditory processing,' 'CAPD,' 'speech perception in noise, 'SPIN,' 'binaural interaction,' 'binaural integration,' 'dichotic listening,' 'temporal processing,' and 'auditory closure.' The keywords were combined with the Boolean search operators to search.
Study selection
After the database search, a three-step process was used to review all studies according to the eligibility criteria: title screening, reading the abstract, and reading the full text. The full text was retrieved for all potentially relevant records meeting the inclusion criteria or for insufficient information in the title and abstract to make a firm decision. Two review authors performed each key step independently for every record. A third author reviewed any discrepancies at each step, and a decision was made after discussion.
Quality assessment
Quality assessment of the included studies was done using the National Institute of Health Quality Assessment Tool for Case–Control Studies for Observational Cohort and Cross-Sectional Studies [28]. Each study was rated to assess the risk of bias. Each study was classified as good, fair, or poor based on the assessment score. Studies with good and fair scores were only included in the review process.
Results
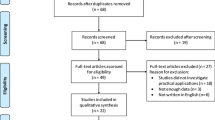
The process of search is represented in Fig. 1. A total of 3087 articles were obtained from the database search. The articles were exported to the Rayyan software [32] to identify and remove the duplicated articles, and 396 duplicates were removed. Title and abstract screening were carried out, and the full texts were screened to select the articles based on eligibility. After the screening process, 18 articles were included in the systematic review. The included studies are cross-sectional studies, prospective controlled studies, and prospective non-randomized clinical studies.

PRISMA flowchart for the selection process of articles in the review
Furthermore, nine out of the eighteen selected studies provided tinnitus pitch and loudness match results on the individuals with tinnitus. Nine studies included participants with both unilateral and bilateral tinnitus, while the remaining had either bilateral or unilateral tinnitus group. All studies except Sanches et al. [4] included information on tinnitus duration. The duration of tinnitus among the selected studies ranged from 3 months to 4 years. Ten studies assessed tinnitus severity using the Tinnitus Handicap Inventory (THI). Of the eighteen studies selected, none of the studies had information regarding the previous or ongoing treatment for tinnitus. Table 1 shows the tinnitus characteristics of the patients included in the various studies.
Studies on assessing temporal perception in individuals with tinnitus have used gap in noise (GIN), gap startle paradigm, gap detection test (GDT), temporal modulation transfer function (TMTF), amplitude modulation depth discrimination (AMDD), and amplitude modulation rate discrimination (AMRD). Four studies carried out the GIN test to assess the temporal resolution, and all the studies showed that the tinnitus group required longer gaps than the control group to identify [4, 5, 9, 21]. Similarly, two studies reported differences between the experimental and control group using the GDT [8, 11]. Fournier and Hébert [20] used the gap startle paradigm to assess temporal resolution. Results showed that participants with tinnitus displayed a stronger startle response than controls without tinnitus, as the tinnitus participants could not perceive the gap embedded in the stimulus. Similarly, Mohanapriya [31] reported poor depth discrimination abilities of the tinnitus group in the presence of noise, while the without noise condition did not show any significant difference between the groups. In contrast, Moon et al. [10] reported no significant difference in spectral ripple discrimination (SRD), temporal modulation detection (TMD), and Schroeder-phase discrimination (SPD) tests among individuals in the tinnitus and no tinnitus groups. For the rate discrimination experiment, the control group performed better than the experimental group in with and without noise conditions at 10- and 100-Hz modulation rates, whereas at 40-Hz modulation rate, there was no significant difference between the groups in the without noise condition [33]. Furthermore, no significant difference was seen between the control and the tinnitus group for temporal sequencing task [5, 9, 11].
Speech perception abilities in tinnitus individuals were assessed using Mandarin speech in noise (MSPIN), Korean version of hearing in noise test (K-HINT), reception threshold for speech (RTS), QuickSIN, speech recognition threshold (SRT), and speech in noise testing Leuven Intelligibility Sentence Test (LIST). In a study where SPIN was assessed using MSPIN, it was noted that the control group had significantly higher scores than the experimental group in high and low predictability list scores [7]. Ryu et al. [14] assessed speech perception using K-HINT, RTS (quiet) and signal-to-noise ratio (SNR) RTS in a quiet environment, and SNR in various noise conditions. Results showed that the scores were significantly poorer in the tinnitus group than in the control group, regardless of whether the noise came from the front, right, or left. QuickSIN results revealed that tinnitus participants had significantly poorer speech-in-noise performance (5 dB SNR) in the left ear than in the right ear, and at 10–25 dB SNR conditions, there was no significant between-group difference [8, 15]. Speech-in-noise testing using LIST was done by Gilles et al. [6], where the tinnitus subjects had significantly worse SRT scores compared to non-tinnitus subjects for sentences embedded in steady-state noise and for sentences embedded in 15-Hz AM noise. Similar results were reported by Moon et al. [10], where the tinnitus-affected ears (TEs) showed poorer SRTs than the non-tinnitus ears (NTEs). Overall, all the studies showed that the tinnitus group either required high SNR or the speech perception was affected compared to the control group.
In this review, three studies tested auditory memory using the reading span test, digit forward span, digit backward span, ascending span test, and descending span test. Kondli, Amruthavarshini, and Prashanth [30] reported that individuals with tinnitus had poor backward span, ascending span, and descending span tasks but not the forward digit span. Furthermore, the reading span test revealed that the reading span of the tinnitus group was significantly shorter than that of the control group [13]. Scores on dichotic auditory verbal memory test (DAVMT), and randomized dichotic digit test (RDDT), showed no significant differences between the tinnitus and control group [29].
Ravirose, Thanikaiarasu, and Prabhu [12] assessed discrimination abilities through duration discrimination test (DDT), difference limen for intensity (DLI), and difference limen for frequency (DLF). Results showed a significant increase in DDT, DLI, and DLF thresholds at the tinnitus frequency compared to half an octave above and below the matched frequency in individuals with tinnitus.
An et al. [22] studied localization through sound localization test (SLT) at 30-degree resolution for a total of 180° on the horizontal plane in front of the listener at a distance of 1 m. The results showed that the mean total error score (TES) was significantly greater in the tinnitus group than in the control group. Regarding stimulus frequency, no significant difference was seen for the tinnitus group. In the control group, mean TES values were significantly higher for 4 and 8 kHz than for 0.25 and 1 kHz. There was no significant difference in the scores between the right tinnitus group, the left tinnitus group, and the bilateral tinnitus group. Also, TES was higher for stimulus presented from the side of the tinnitus than the opposite side. There was no correlation between tinnitus pitch and TES and between tinnitus loudness and TES. A summary table of the selected articles is given in Table 2.
Discussion
The present review aims to study tinnitus’ effect on central auditory processing abilities. Eighteen articles were shortlisted after extensive review. The majority of the articles showed that individuals with tinnitus had affected central auditory processing, which was seen in terms of poor temporal processing [4, 5, 8, 9, 11, 20], poor auditory memory [13, 30], and reduced SPIN [7, 8, 10, 14]. The anatomical and physiological defects in the central auditory nervous system’s neural structures result in tinnitus perception and impair central auditory processing abilities.
Studies reported that temporal resolution was affected in individuals with tinnitus, assessed using the GIN test and TMTF [4, 5, 8, 9, 11, 20]. Boyen et al. [34] postulated that the reason for poor gap detection could be that ongoing tinnitus masks the gap, resulting in impaired gap detection and modulation function. Also, physiologically, detecting silence gaps in noise requires precise processing of the temporal structure of the sound stimulus [33]. The difference in the GIN test performance between patients with and without tinnitus shows dysfunction in the central auditory system in patients with tinnitus [35].
It has also been reported that there is hyperactivity in cortical and thalamic structures in tinnitus patients [36]. This can lead to neural changes at the higher auditory structures, reorganizing the tonotopic map. These neural changes are thought to alter the temporal processing abilities of individuals with tinnitus. Good performance in auditory temporal resolution requires precise neuronal firing, which can be impaired in individuals with tinnitus [5, 9]. However, studies on temporal sequencing using duration pattern test (DPT) and frequency pattern test (FPT) found no difference between the clinical and control groups [9]. This could be attributed to the insensitivity of the tests used to assess temporal ordering (sequencing) to the abnormalities of structures below the auditory cortex [1].
Studies also report tinnitus interferes with SPIN [7, 8, 10, 14]. Studies have shown that tinnitus patients had aberrant links between the limbic and auditory systems, suggesting that tinnitus might originate in the central auditory system rather than the cochlea. Changes in cortical plasticity might account for tinnitus and associated symptoms which affect speech perception [24, 37]. Studies have also reported that tinnitus may affect the central auditory system as “a central masker” that interrupts speech perception [10].
The present systematic review also showed that auditory memory was affected in individuals with tinnitus [13, 30]. Attention resources may be disrupted or depleted due to negative thoughts due to tinnitus, continual orienting to tinnitus [13], and increased self-focused and somatic attention [38], which can cause poor auditory memory. Individuals with tinnitus, for whom annoyance is generally linked with tinnitus, have been shown to perform poorly compared to others for whom tinnitus is not annoying. Hence, the attention toward the auditory stimulus would be reduced [39]. Few studies reported no difference between the mild tinnitus and the control groups in individuals with normal hearing in the divided auditory attention and verbal auditory memory [29]. This indicates that the severity of tinnitus has a differential effect on auditory memory.
Studies on the effect of tinnitus on dichotic listening are sparse [11]. These studies have shown no difference in dichotic listening among tinnitus and no tinnitus groups. However, Cuny et al. [40] reported that tinnitus modifies the normal left-hemisphere specialization in the dichotic listening test. The reason could be that tinnitus modifies the organization of cerebral function. Tinnitus has also been shown to interfere with sound localization ability [22]. The interference is worse when the sound originates from the same side as the tinnitus because the tinnitus reduces interaural level difference [22].
Furthermore, it was noted that THI was used predominantly to measure tinnitus severity across studies. In addition, most studies have not reported tinnitus characteristics such as pitch and loudness (n = 9). It is felt that standardization of assessment protocols and reporting of results could overcome these problems. The details of the tinnitus rehabilitation are missing, as these would have affected the auditory processing test results; hence, a detailed pre- and post-assessment report are needed. The sample size of the individual studies included in the review ranged from 9 to 40 participants per group.
Furthermore, most of the studies did not perform a power analysis. With a low sample size, the generalizability of the individual study results to the tinnitus population becomes debatable. Hence, the results of this review could stand as preliminary evidence for an auditory processing deficit in individuals with tinnitus. Thus, the present systematic review concludes that temporal resolution, speech perception in noise, and working memory are the most affected skills in individuals with tinnitus and normal hearing.
Conclusion
Central auditory processing is affected in individuals with tinnitus in terms of difficulty in understanding speech in noise, temporal processing, localization, and auditory memory. The assessment of central auditory processing abilities should be routinely included for individuals with tinnitus. Further studies are needed with large sample size and various degrees of tinnitus severity to assess various central auditory processing abilities.
Availability of data and materials
Not applicable.
Abbreviations
- (C)APD:
-
Central auditory processing disorder
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- GIN:
-
Gap in noise
- PTA:
-
Pure-tone audiometry
- M:
-
Males
- F:
-
Females
- GDT:
-
Gap detection test
- MDT:
-
Modulation detection test
- DLF:
-
Difference limen for frequency
- DLI:
-
Difference limen for intensity
- SPIN:
-
Speech perception in noise
- THI:
-
Tinnitus Handicap Inventory
- SD:
-
Standard deviation
- DPT:
-
Duration pattern test
- MSPIN:
-
Mandarin speech in noise
- TLS:
-
Tinnitus loudness scale
- UTG:
-
Unilateral tinnitus group
- BTG:
-
Bilateral tinnitus group
- TMTF:
-
Temporal modulation transfer function
- DDT:
-
Duration discrimination test
- FPT:
-
Frequency pattern test
- DLT:
-
Dichotic listening test
- REA:
-
Right ear advantage
- DPOAE:
-
Distortion product otoacoustic emissions
- DAVMT:
-
Dichotic auditory verbal memory test
- RDDT:
-
Randomized dichotic digit test
- SLT:
-
Sound localization test
- TES:
-
Total error score
- ES:
-
Error score
- K-HINT:
-
Korean version of hearing in noise test
- RTS:
-
Reception threshold for speech
- SNR:
-
Signal-to-noise ratio
- SRD:
-
Spectral ripple discrimination test
- TMD:
-
Temporal modulation detection test
- SPD:
-
Schroeder-phase discrimination test
- SRT:
-
Speech recognition threshold
- TE:
-
Tinnitus-affected ears
- NTE:
-
Non-tinnitus ears
- NIT:
-
Noise-induced tinnitus
- LIST:
-
Leuven intelligibility sentence test
- AMRD:
-
Amplitude modulation rate discrimination
- AMDD:
-
Amplitude modulation depth discrimination
References
Han BI, Lee HW, Kim TY, Lim JS, Shin KS (2009) Tinnitus: characteristics, causes, mechanisms, and treatments. J Clin Neurol (Korea) 5(1):11–19. https://doi.org/10.3988/jcn.2009.5.1.11
Langguth B, Kreuzer PM, Kleinjung T, De Ridder D (2013) Tinnitus: causes and clinical management. Lancet Neurol 12(9):920–930. https://doi.org/10.1016/S1474-4422(13)70160-1
Jastreboff PJ (2007) Tinnitus retraining therapy. Prog Brain Res 166:415–423. https://doi.org/10.1016/S0079-6123(07)66040-3
Sanches SGG, Samelli AG, Nishiyama AK, Sanchez TG, Carvallo RMM (2010) GIN test ( gaps-in-noise ) in normal listeners with and without tinnitus. Pró-Fono Revista de Atualização Científica 22(3):257–262. https://doi.org/10.1590/S0104-56872010000300017
Gilani VM, Ruzbahani M, Mahdi P, Amali A, Khoshk MHN, Sameni J, Yazdi AK, Emami H (2013) Temporal processing evaluation in tinnitus patients: results on analysis of gap in noise and duration pattern test. Iran J Otorhinolaryngol 25(73):221
Gilles A, Schlee W, Rabau S, Wouters K, Fransen E, Van de Heyning P (2016) Decreased speech-in-noise understanding in young adults with tinnitus. Front Neurosci 10:1–14. https://doi.org/10.3389/fnins.2016.00288
Huang C-Y, Lee H-H, Chung K-C, Chen H-C, Shen Y-J, Wu J-L (2007) Relationships among speech perception, self-rated tinnitus loudness and disability in tinnitus patients with normal pure-tone thresholds of hearing. ORL 69(1):25–29. https://doi.org/10.1159/000096713
Jain C, Sahoo JP (2014) The effect of tinnitus on some psychoacoustical abilities in individuals with normal hearing sensitivity. Int Tinnitus J 19(1):28–35. https://doi.org/10.5935/0946-5448.20140004
Jain S, Dwarkanath VM (2016) Effect of tinnitus location on the psychoacoustic measures of hearing. Hear Bal Comm 14(1):8–19
Moon IJ, Won XJH, Kang HW, Kim XDH, An Y, Shim XHJ (2015) Influence of tinnitus on auditory spectral and temporal resolution and speech perception in tinnitus patients. J Neurosci 35(42):14260–14269. https://doi.org/10.1523/JNEUROSCI.5091-14.2015
Raj-Koziak D, Gos E, Szkiełkowska A, Panasiewicz A, Karpiesz L, Kutyba J, Skarzynski H, Skarzynski PH (2022) Auditory processing in normally hearing individuals with and without tinnitus: assessment with four psychoacoustic tests. Eur Arch Otorhinolaryngol 279(1):275–283. https://doi.org/10.1007/s00405-021-07023-w
Ravirose U, Thanikaiarasu P, Prabhu P (2019) Evaluation of differential sensitivity for frequency, intensity, and duration around the tinnitus frequency in adults with tonal tinnitus. J Int Adv Otol 15(2):253–256. https://doi.org/10.5152/iao.2019.6698
Rossiter S, Stevens C, Walker G (2006) Tinnitus and its effect on working memory and attention. J Speech Lang Hear Res 49(1):150–160. https://doi.org/10.1044/1092-4388(2006/012)
Ryu IS, Ahn JH, Lim HW, Joo KY, Chung JW (2012) Evaluation of masking effects on speech perception in patients with unilateral chronic tinnitus using the hearing in noise test. pp 1472–1476
Tai Y, Husain FT (2019) The role of cognitive control in tinnitus and its relation to speech-in-noise performance. J Audiol Otol 23(1):1–7. https://doi.org/10.7874/jao.2018.00409
Lauter JL (1999) Central auditory processing. Curr Opin Otolaryngol Head Neck Surg 7(5):274–281. https://doi.org/10.1097/00020840-199910000-00011
Moore DR, Rosen S, Bamiou DE, Campbell NG, Sirimanna T, James Bellis T, Chermak G, Weihing J, Musiek F, Dillon H, Cameron S (2013) Evolving concepts of developmental auditory processing disorder (APD): a British Society of Audiology APD Special Interest Group “white paper.” Int J Audiol 52(1):3–13. https://doi.org/10.3109/14992027.2012.723143
Martin JS, Jerger JF (2005) Some effects of aging on central auditory processing. J Rehabil Res Dev 42(4 SUPPL. 2):25–44. https://doi.org/10.1682/JRRD.2004.12.0164
Diges I, Simón F, Cobo P (2017) Assessing auditory processing deficits in tinnitus and hearing impaired patients with the auditory behavior questionnaire. Front Neurosci 11:187. https://doi.org/10.3389/fnins.2017.00187
Fournier P, Hébert S (2013) Gap detection de fi cits in humans with tinnitus as assessed with the acoustic startle paradigm : does tinnitus fi ll in the gap ? Hear Res 295:16–23. https://doi.org/10.1016/j.heares.2012.05.011
Sanches SGG, Sanchez TG, Carvallo RMM (2010) Influence of cochlear function on auditory temporal resolution in tinnitus patients. Audiol Neurootol 15(5):273–281. https://doi.org/10.1159/000272939
An Y-H, Lee LH, Yoon SW, Jin SY, Shim HJ (2012) Does tinnitus affect the sound localization ability? Otol Neurotol 33(5):692–698
Vielsmeier V, Kreuzer PM, Haubner F, Steffens T, Semmler PRO, Kleinjung T, Schlee W, Langguth B, Hoare DJ, Wise KJ (2016). Speech comprehension difficulties in chronic tinnitus and its relation to hyperacusis 8;1–8. https://doi.org/10.3389/fnagi.2016.00293
Reyes SA, Salvi RJ, Burkard RF, Coad ML, Wack DS, Galantowicz PJ, Lockwood AH (2002) Brain imaging of the effects of lidocaine on tinnitus. Hear Res 171(1–2):43–50. https://doi.org/10.1016/S0378-5955(02)00346-5
Campolo J, Lobarinas E, Salvi R (2013) Does tinnitus «fill in» the silent gaps? Noise Health 15(67):398–405. https://doi.org/10.4103/1463-1741.121232
Zeng FG, Richardson M, Turner K (2020) Tinnitus does not interfere with auditory and speech perception. J Neurosci 40(31):6007–6017. https://doi.org/10.1523/JNEUROSCI.0396-20.2020
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Academia and Clinic Annals of Internal Medicine Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Ann Intern Med 151(4):264–269
National Institutes of Health (NIH). Study quality assessment tools. National Heart, Lung, and Blood Institute. Available online:https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Shakarami S, Rouzbahani M, Mahdavi ME, Hosseini AF (2015) Auditory attention and memory in normal hearing individuals with and without tinnitus. Aud Vestib Res 24(4):201–209
Kondli M, Amruthavarshini N, Prashanth P (2019) Assessment of auditory working memory in normal hearing adults with tinnitus. Eur Arch Otorhinolaryngol 277(5):47–54. https://doi.org/10.1007/s00405-019-05658-4
Mohanapriya (2020) Amplitude modulation discrimination in individuals with normal hearing sensitivity having tinnitus. An Unpublished Dissertation, Mysuru: University of Mysuru
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A (2016) Rayyan — a web and mobile app for systematic reviews. Syst Rev 5:210. https://doi.org/10.1186/s13643-016-0384-4
Musiek FE, Shinn JB, Jirsa R, Bamiou DE, Baran JA, Zaida E (2005) GIN (gaps-in-noise) test performance in subjects with confirmed central auditory nervous system involvement. Ear Hear 26(6):608–618. https://doi.org/10.1097/01.aud.0000188069.80699.41
Boyen K, Başkent D, van Dijk P (2015) The gap detection test: can it be used to diagnose tinnitus? Ear Hear 36(4):e138-145. https://doi.org/10.1097/AUD.0000000000000156
Eggermont JJ, Roberts LE (2004) The neuroscience of tinnitus. Trends Neurosci 27(11):676–682. https://doi.org/10.1016/j.tins.2004.08.010
Noreña AJ, Eggermont JJ (2003) Changes in spontaneous neural activity immediately after an acoustic trauma: implications for neural correlates of tinnitus. Hear Res 183(1–2):137–153. https://doi.org/10.1016/S0378-5955(03)00225-9
Lockwood AH, Salvi RJ, Coad ML, Towsley ML, Wack DS, Murphy BW (1998) The functional neuroanatomy of tinnitus: evidence for limbic system links and neural plasticity. Neurology 50(1):114–120. https://doi.org/10.1212/wnl.50.1.114
Newman CW, Wharton JA, Jacobson GP (1997) Self-focused and somatic attention in patients with tinnitus. J Am Acad Audiol 8(3):143–9
Andersson G, McKenna L (2006) The role of cognition in tinnitus. Acta Otolaryngol 126(SUPPL. 556):39–43. https://doi.org/10.1080/03655230600895226
Cuny C, Che S, Bougeant J, Koenig O (2004) Investigation of functional hemispheric asymmetry of language in tinnitus sufferers. Neuropsychology 18(2):384–392. https://doi.org/10.1037/0894-4105.18.2.384
Acknowledgements
Not applicable.
Funding
No funding was received to assist with the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
SS was involved in concept development, study selection, analysis of the results, interpretation, and writing the manuscript; VV was involved in concept development, study selection, analysis of the results, interpretation, and writing the manuscript; CJ was involved in concept development, study selection, analysis of the results, interpretation, and writing the manuscript; and all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
S., S., Vinod, V. & Jain, C. Central auditory processing abilities in individuals with tinnitus and normal hearing sensitivity: a systematic review. Egypt J Otolaryngol 39, 126 (2023). https://doi.org/10.1186/s43163-023-00494-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-023-00494-0