
Abstract
Background
The vestibular system can perceive sound at high intensity levels. The recording of vestibular evoked myogenic potentials (VEMPs) is one of the clinical techniques that capture the vestibular system when activated by sound. In healthy individuals, it has been demonstrated that VEMP thresholds are lower when using low-frequency stimuli, particularly 500 Hz tone burst. Aging affects frequency tuning, causing shift to higher frequencies.
Methods
This study was cross-sectional, which included 80 normal healthy individuals. Each participant in the study were subjected to cervical vestibular evoked myogenic potential (cVEMP) testing using air and bone conduction as a mode of stimulation. The following cVEMP parameters were assessed: cVEMP inter-frequency peak amplitude ratio (FAR): the ratio of peak-to-peak amplitude between 500 Hz and 1000 Hz in the same ear (1000 Hz/500 Hz FPA). Also, rectified FAR is a method of normalizing the amplitude of the VEMP response to the degree of muscle contraction as determined by EMG.
Results
There were differences among the 5 age groups that were statistically different regarding FAR and rFAR of cVEMP when using air and bone conduction stimuli.
Conclusion
In this study, we provided age norms for frequency amplitude ratio (FAR) (1000/500 Hz) of cVEMP using AC and BC stimuli. Participants above the 50 years age group showed significantly larger FAR and rectified FAR than the younger age groups in both the cVEMP. Air and bone conduction stimuli yielded similar FAR results and can be both used in testing.
Similar content being viewed by others


Background
The vestibular system can perceive sound at high intensity levels. The recording of vestibular evoked myogenic potentials (VEMPs) is one of the clinical techniques that capture the vestibular system when activated by sound [1]. There are two types of VEMP: cervical and ocular. The cervical type was first mentioned by Colebatch et al. [2]. Cervical VEMP (cVEMP) is recorded when the saccule otolith organ is stimulated causing activation of the descending vestibulo-spinal pathways [3]. A response is recorded in form of a positive peak around 13 ms latency and a negative peak around 23 ms latency which is called the saccular reflex [4]. Ocular VEMP (oVEMP) is produced from the utricle otolith organ with the ascending vestibular pathways being activated. A negative peak at 10 ms is the required response to confirm the contraction of inferior oblique muscle, which is the source of oVEMP response and the utricular reflex [5].
The VEMP test has been used to test clinically the otoliths organs, especially the saccule which is supplied by inferior branch of vestibular nerve. Non-identification of VEMP waves were found in several pathologies such as vestibular neuritis, idiopathic bilateral vestibulopathy, and Meniere’s disease.
VEMP amplitude relation between both ears is relatively symmetrical in normal persons [6]. Interaural amplitude asymmetry ratio (IAR) is affected in healthy individuals due to aging. Above the age of 60, threshold increases with amplitude reduction; also, response might be missing on one side. Below 60, the range of amplitude asymmetry ratios is less than 35% [7].
The results of Kumar et al. [8] found that, when compared to young and middle-aged individuals, there is a considerable difference in latency and amplitude in older adults. Hence, age should be considered while interpreting VEMP results. In Egypt, a study done on the Egyptian population by Shabana et al. [9] confirms a large age-related elevation in cVEMP thresholds and a considerable prolongation of P13 latencies.
For VEMP generated by air conduction (AC), the typical preferred stimulus frequency ranges from 500 to 1000 Hz [10]. However, with bone conduction (BC) stimulation, VEMP thresholds are obtained at a hearing level that is approximately 30–40 dB lower than that obtained with AC stimulation [11].
It has been proven that VEMP responses are more responsive to low frequencies in normal subjects, whereas compared to other frequencies, a 500-Hz tone burst can elicit greater amplitudes, lower thresholds, and a higher response rate for both oVEMP and cVEMP. Aging affects frequency tuning, causing shift to higher frequencies [12].
The elevated impedance caused by endolymphatic hydrops (EH) is one hypothesis that suggests a potential explanation for the frequency specificity of VEMP [13]. The elevation in frequency specificity could be explained by the possibility that EH makes the inner ear more rigid and, as a result, reduces low-frequency transmission. This effect explains why persons with Meniere’s disease have a reduced sensitivity at 500 Hz. But one must proceed with caution because it is known that healthy aging results in similar frequency shifts [14].
Rectified (FAR) is a technique for adjusting the VEMP response’s amplitude to the EMG-measured intensity of muscular contraction. This is done to take into account any asymmetry in the strength of the sternocleidomastoid muscle contraction on one side compared to the other, which may affect how much of an amplitude difference there is between the two sides. cVEMP amplitude is significantly influenced by muscle contraction [15]. It is challenging to evaluate and compare studies that did not adjust cVEMPs for muscular contraction since they infrequently assess muscle contractions between groups.
Rationale
It has been established that Meniere’s disease alters cVEMP’s frequency response. Therefore, while assessing frequency tuning, age norms are necessary. To the best of our knowledge, no research has been done in Egypt to establish normative values for the cVEMP’s frequency amplitude tuning properties across age ranges.
Aim of the study
The purpose of the study is to evaluate cVEMP characteristics and the inter-frequency amplitude ratio as they relate to aging (frequency tuning), using 500 and 1000 Hz and using air and bone conduction stimuli (i.e., to obtain age-related normative data), as well as to show if there was any difference in frequency tuning between air and bone conduction of cVEMP.
Methods
Subjects
This study was a cross-sectional type that included 80 normal healthy individuals without medical history of any diseases and not complaining of any ear, hearing, or balance problems. They were collected from those performing the preoccupation assessment at the audiology clinic, and healthy relatives of patients, and volunteers from medical personnel in the clinic, after taking their consent for participation in the study. The research was ethically approved by the University Research Ethics committee.
Inclusion criteria:
Normal healthy young and older adult individuals of both genders were divided into different age groups: 20–29 years, 30–39 years, 40–49 years, 50–59 years, and ≥ 60 years.
Exclusion criteria:
-
Conductive hearing loss
-
Facial anomalies, 3rd nerve palsy
-
Neck problems hindering the testing (e.g., absence of one or both sternocleidomastoid muscles)
-
Patients with other peripheral or central vestibular disorder
-
Patients with other neurological, psychiatric, or significant medical disorders
Methods
The following procedures will be carried out on study participants.
-
1)
Full history taking
-
2)
Otoscopic examination for both ears
-
3)
Basic audiologic evaluation [16]
-
a)
Pure tone audiometry
-
Pure-tone air conduction thresholds obtained from 250 Hz to 8 kHz, and
-
Pure-tone bone conduction thresholds will be obtained at 500 Hz, 1 kHz, 2 kHz, and 4 kHz.
-
-
b)
Speech audiometry including the following: speech recognition threshold, word recognition score using Arabic words [17]
-
c)
Tympanometry using the conventional 226-Hz probe tone and acoustic reflex threshold testing
-
4)
Cervical vestibular evoked myogenic potential (cVEMP) testing, using special equipment:
-
Electrode montage
After cleaning the skin with a gel, the active (non-inverting) (positive) electrode was placed on the middle of the sternocleidomastoid (SCM) muscle, followed by the inverting (reference) (negative) electrode on the upper part of the sternum (suprasternal notch), and the ground electrode was placed on the forehead. Less than 5 KOhms of electrode impedance were maintained. The subjects were advised to tighten the muscle by tucking their chins over to the opposite shoulder during runs of acoustic stimulation and to relax between the runs to prevent fatigue, throughout the test, which was conducted with them sitting erect. For low noise levels during cVEMP recordings, the rectified EMG was measured.
-
Stimulus and recording parameters
Stimuli were tone bursts at two different frequencies (500 Hz and 1000 Hz) will be used. Air-conducted stimuli using ER-3A insert earphones and bone-conducted stimuli using clinical bone vibrator (B71) will be used, with rise time 1 ms, fall time 1 ms, and plateau 2 ms duration, presented monaurally at intensity of 100 dBnHL for AC and 60 dBnHL for BC. Stimulus rate was 5 Hz. A 30–2000 Hz filter was used to get at least 60 sweeps. The analytical window had a 50-ms time limit. To assure repeatability, averaged signals were acquired twice. P13-N23 biphasic response presence or absence was used to determine whether VEMP responses were present or absent. The cVEMP parameters that were assessed are as follows:
-
Inter-aural amplitude asymmetry (difference) ratio at 500 Hz, latencies of P13, N23, and P13-N23 peak amplitude
-
Inter-aural amplitude asymmetry (difference) ratio at 1000 Hz, latencies of P13, N23, and P13-N23 peak amplitude
-
Calculating the cVEMP inter-frequency peak amplitude ratio (FAR): the ratio of peak amplitude between 500 Hz and 1000 Hz in the same ear (1000 Hz/500 Hz FPA)
-
Equipment
-
1.
Sound insulated cabin (Ampisilence E)
-
2.
Audiometer: Itera II (Madsen Corporation, USA), calibrated according ISO standards. TDH 39 and bone vibrator radio-ear B71 were used
-
3.
Tympanometer: Zodiac 901 (Madsen Corporation, USA), calibrated according ISO standards
-
4.
Evoked potentials system: Neuro-Audio v10.1 (Neurosoft Ltd, Russia)
Statistical analysis methods and technique
The SPSS version 21 data analysis software will be used. Quantitative data will be provided as mean, standard deviation, median, and interquartile range, while qualitative data will be presented as numbers and percentages. Significant results will be determined using both parametric and nonparametric tests (chi-square, Student t test and McNemar test). The threshold for significance was fixed at p = 0.05 or less.
Sampling technique
Convenient sample of patients coming to hospital with the inclusion and exclusion criteria will be assigned to the study, till reaching total sample size calculated.
Sample size
We used the clinical sample size calculator for analytical study, with a 0.05 alpha error and power of the study 0.80. To calculate the minimal sample size needed to detect the effect of age and stimulus type on the frequency tuning and amplitude asymmetry ratio of the cervical vestibular evoked myogenic potentials, according to the literature, for patients aged 18 to 65 years old, the P1 and N1 latencies mean values were 6.63 ± 2.88 ms in younger patients and 9.67 ± 3.15 ms in older patients (19). The sample size calculated is 80 patients.
Results
The study included 80 normal healthy adult individuals: 40 of them were males and 40 were females, with a mean age of 44.65 years ± 15.97 (ranging from 20 to 85 years). Subjects were grouped into 5 groups according to age:
-
Group 1: 16 individuals, whose age ranged from 20–29 years
-
Group 2: 16 individuals, whose age ranged from 30–39 years
-
Group 3: 16 individuals, whose age ranged from 40–49 years
-
Group 4: 16 individuals, whose age ranged from 50–59 years
-
Group 5: 16 individuals, whose age was ≥ 60 years
All study participants exhibited auditory reflex thresholds that were within normal limits and bilateral type (A) curve tympanograms that showed normal middle ear pressure. The research groups’ means (X), standard deviations (S.D), and ranges of ages (in years) are shown in Table 1. The gender distribution of the study groups is shown in Table 2. Regarding gender distribution, there was no statistically significant difference (p > 0.05) between them. In group 5, only 5/16 subjects were above 70 years. The distribution of cVEMP response above 70 years is shown in Fig. 3.
There were differences among the study groups regarding the response rates of cVEMP air conduction at 500 Hz and 1000 Hz in both ears that were statistically significant. All participants in groups 1, 2, and 3 had a cVEMP response compared to others in group 4 and group 5. Figure 1 shows the cVEMP air conduction (AC) traces at 1000 Hz and 500 Hz in the five age groups.

cVEMP air conduction (AC) traces at 1000 Hz and 500 Hz in the 5 age groups
Regarding the response rates of cVEMP bone conduction at 500 Hz, there were no detectable significant changes between the study groups. However, a difference that was statistically significant was present among the study groups regarding the response rates of cVEMP bone conduction at 1000 Hz, where all participants in groups 1, 2, and 3 had present cVEMP response at 1000 Hz, compared to others in group 4 and group 5. Figure 2 shows the cVEMP bone conduction (BC) traces at 1000 Hz and 500 Hz in the five age groups.

cVEMP bone conduction (BC) traces at 1000 Hz and 500 Hz in the 5 age groups. In group 5, only 5/16 subjects were above 70 years. The distribution of cVEMP response above 70 years is shown in Fig. 3
Regarding FAR and rFAR of cVEMP air, there were statistically significant differences among the five age groups (Table 3).
Regarding FAR and rFAR of cVEMP bone, there were statistically significant differences across the five age groups (Table 4).
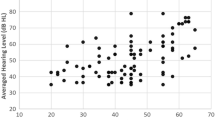
Age and all air conduction cVEMP metrics correlated with statistical significance (p < 0.05) at 500 and 1000 Hz in both ears of the study participants except between age and the amplitude and the rectified amplitude in both ears at 1000 Hz. The significant correlation was an inverse correlation regarding amplitude (Table 5).
There was a statistically significant (p < 0.05) correlation between age and all bone conduction cVEMP parameters at 500 and 1000 Hz in both ears of the study participants except between age and the amplitude of right ear at 1000 Hz and age and the right FAR and rFAR. The significant correlation was an inverse correlation regarding amplitude (Table 6).
Discussion
There were 80 healthy, normal adult participants in this study—40 men and 40 women. According to age, the participants were split into 5 groups, each with 16 members: Group 1 (20–29 years), group 2 (30–39 years), group 3 (40–49 years), group 4 (50–59 years), and group 5 (> 60 years). All study participants exhibited auditory reflex thresholds that were within normal limits and bilateral type (A) curve tympanograms that showed normal middle ear pressure. The purpose of this study was to evaluate cVEMP parameter changes caused by aging, especially inter-frequency amplitude ratio (frequency tuning), using 500 and 1000 Hz and using air and bone conduction stimuli (i.e., to obtain age -related normative data) and to show if there was any difference in frequency tuning between air and bone conduction of VEMP.
In the current study, the absence of VEMP response was found mainly in participants above 50 years old and was more obvious in participants more than 60 years old, including those > 70 age years old: above 70 years showed 40%, 60%, 80%, and 80% of cVEMP losses for AC at 500 Hz, 1000 Hz, and BC at 500 Hz and 1000 Hz respectively (Fig. 3). So, we cannot depend on cVEMP results for diagnoses in elderly population.

The distribution of cVEMP AC and BC response, at 500 and 1000 Hz, above 70 years
Up until the age of 50–60, a healthy persons’ cVEMP response is stable [18]. The cVEMP response begins to decline at the age of 60, when thresholds rise and amplitudes fall [19]. The cVEMP amplitude in particular is thought to be a sensitive indicator for aging of the vestibular organs.
The five vestibular organs contain only type I and type II hair cells. In individuals with age above 85 years, most research documented a decrease in the total density and number of those two types of cells [20]. Also, otoconia decrease in number and volume.
Additionally, Scarpa’s ganglion’s number of ganglion cells begins to drop at the age of 30 [21]. The vestibular nerve does not show a change in the number of fibers; however, it starts showing amyloid bodies (pathologic protein aggregates) which affects the nerve’s thickness.
In this study, cVEMP air and bone conduction were more commonly elicited at 500 Hz than at 1000 Hz. cVEMPs at 500 Hz were elicited in 72 (90%) and 75 (94%) using air and bone conduction, respectively, in comparison to 71 (89%) and 65 (82%) at 1000 Hz using air and bone conduction respectively.
Based on the results of this work, 500 Hz is the best stimulation frequency for the cVEMP, which was in accordance with Fu et al. [22]. The majority of participants still had the best frequency at 500 Hz, even if only a small number of middle-aged people demonstrated that 1000 Hz was the ideal frequency.
VEMP parameters differences among the studied groups (correlation with age)
Frequency amplitude ratio (FAR) of cVEMP using AC and BC stimuli
Other researchers showed that tone bursts were more effective than clicks at generating both cVEMPs and oVEMPs [23, 24]. Response to AC tone bursts between 500 and 1000 Hz resulted in the highest recorded values of the cVEMP and oVEMP amplitudes [25,26,27,28]. Five hundred and 1000 Hz were the ideal frequencies that produced the highest cVEMP amplitudes [29].
In this study, the norms for frequency amplitude ratio (1000/500 Hz) of cVEMP using AC and BC stimuli in different age groups were provided. Between the right and left ears, there were no statistically significant differences, regarding the FAR or rectified FAR cVEMP, using either AC or BC stimuli in all groups of the study (p > 0.05), so the right ear values are provided here.
cVEMP—FAR
-
AC
In the current study, the rectified FAR of cVEMP using AC stimuli increased with age: the normal subjects’ rFAR values range varied from about 0.59 to 0.83 for subjects from 20 to 29 years of age, 0.53 to 0.77 for 30 to 39 years, 0.56 to 0.79 for 40 to 49 years, 0.88 to 1.18 for 50 to 59 years, and 0.67 to 1.06 for normal subjects > 60 years (Table 3).
-
Effect of age on cVEMP air conduction FAR
Participants in the 50–59 years age group had a significantly higher mean of FAR and rectified FAR than those in the 20–29 years age group (Fig. 4). As age increased, FAR and rectified FAR of cVEMP air conduction in both ears significantly increased (Table 5).

cVEMP air conduction FAR and r FAR of the right and left ears of the 5 age groups in this study. There were no statistically significant differences between the right and left ears cVEMP air conduction FAR or rectified FAR of the any of the 5 age groups in this study (p > 0.05)
In agreement with this study, Piker et al. [12] discovered that older people’s cVEMP tuning switched to higher frequencies causing that FAR seemed to be higher among the elderly. They came to the conclusion that, depending on the age group, the optimal frequency to trigger VEMPs may not be 500 Hz.
Asian participants’ responses to tone burst frequencies of 250, 500, 1000, and 1500 Hz on cVEMP waveforms were examined by Fu et al. [22]. The optimal frequency for cVEMP was 500 Hz. Todd et al. [30] found the largest cVEMP responses were produced by air conduction tone burst stimuli between 400 and 800 Hz and observed saccular resonance at 600 Hz.
-
BC
In the current study, the rectified FAR of cVEMP using BC stimuli increased with age: the normal subjects’ FAR values range varied from about 0.52 to 0.77 for subjects from 20 to29 years of age, 0.49to 0.88 for 30 to 39 years, 0.46 to 0.65 for 40 to 49 years, 0.47 to 0.70 for 50 to 59 years, and 0.71 to 1.26 for normal subjects > 60 years (Table 4).
-
Effect of age on cVEMP bone conduction FAR
Participants from (50 to 59 years of age) showed significantly larger rectified FAR than participants from (20 to 39 years of age) (Fig. 5). And as age increased, FAR and rectified FAR cVEMP bone conduction in both ears increased (Table 6).

cVEMP bone conduction FAR and r FAR of the right and left ears of the 5 age groups in this study. There were no statistically significant differences between the right and left ears cVEMP bone conduction FAR or rectified FAR of the any of the 5 age groups in this study (p > 0.05)
According to Miyamoto et al. [31], healthy subjects’ optimal BC cVEMP frequencies are in the range of 250 Hz. The response was highest for stimulus frequencies of 200 to 400 Hz, according to Sheykholeslami et al. [32].
-
AC- versus BC- cVEMP FAR
In any of the five study groups, there were no statistically significant variations in the air and bone conduction FAR of cVEMP in either ear.
Using frequencies ranging from 250 to 2000 Hz, Welgampola et al. [33] demonstrated the frequency tuning capabilities of cVEMP in both air and bone conduction. The tuning curve for air conducted tones had peaks between 500 and 1000 Hz and a sharp decline at 250 Hz. In contrast, the maximum amplitudes of bone conducted VEMP occurred at 250 Hz.
At higher frequencies, the otolithic membrane attenuates hair bundle displacement and functions as a low-pass filter. Extrastriolar hair cells capture phase information from stimuli at frequencies lower than 100 Hz, which enhances the VEMP response more than information obtained from stimuli at higher frequencies (as high as 1 kHz). Additionally, at lower frequencies compared to higher frequencies, the VEMP response more closely resembles the stimulus carrier [30].
The response of VEMP to frequencies differently has been used in research, particularly using 500/1000 Hz amplitude ratio in identifying Meniere’s disease [34]. They noted that (1) a rise in this ratio indicated an increase in the saccule’s sensitivity to 500 Hz, and (2) a drop in this ratio indicated an increase in the saccule’s sensitivity to 1000 Hz. Due to the increased sensitivity of VEMP to higher frequencies in affected MD patients compared to unaffected controls, we could use this ratio to distinguish between them.
However, we should put in mind that aging also affects frequency sensitivity of VEMP (Piker et al., 2013), and aging should be accounted for in further studies.
Additionally, Piker et al. [12] found evidence of a possible association between age group and frequency response for the cVEMP, suggesting that older persons may tune less accurately. Dudman [35] observed a decrease in susceptibility to 500 Hz tone bursts in aged individuals. Atabek [36] found that in the group of older people, the 1000 Hz tone burst stimulus elicited the largest cVEMP amplitude in comparison to both 500 Hz and 750 Hz, even if there were not yet statistically significant differences.
Decreased sensitivity and reactivity of the degenerating high-frequency responsive otolith afferents are more directly responsible for the decline in peripheral vestibular function than simply hair cell aging [37]. The vestibular ganglion cells and their neurons, along with the big, myelinated fibers, are the sites where majority of the age-related alterations take place.
Conclusion
-
1.
The rate VEMP response loss was different across different age groups. Thus, interpretation of VEMP should be supplemented by each lab’s normative data.
-
2.
In the elderly population, VEMP results may not be so helpful in diagnoses because of high VEMP loss rate.
-
3.
cVEMP is more commonly elicited at 500 Hz than at 1000 Hz, using either air or bone conductions.
-
4.
Using bone conduction cVEMP at 1000 Hz is more commonly elicited.
-
5.
Participants above the 50 years age group showed significantly larger FAR and rectified FAR than the younger age groups in both of cVEMP’s modes of stimulation.
Recommendation
Age should be accounted for when using cVEMP. Further studies should be considered for oVEMP testing. Also, significant evidence for use of frequency tuning in Meniere’s disease was reported; this should be further investigated.
Availability of data and materials
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
22 February 2023
A Correction to this paper has been published: https://doi.org/10.1186/s43163-023-00398-z
References
Luecke VN, Buchwieser L, Zu Eulenburg P, Marquardt T, Drexl M (2020) Ocular and cervical vestibular evoked myogenic potentials elicited by air-conducted, low-frequency sound. J Vestib Res 30(4):235–247
Colebatch JC, Halmagyi GM, Skuse NF (1994) Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry 57:190–197
Rosengren SM, Welgampola MS, Colebatch JG (2010) Vestibular evoked myogenic potentials: past, present and future. Clin Neurophysiol 121(5):636–651
Gürkov R, Flatz W, Louza J, Strupp M, Krause E (2011) In vivo visualization of endolymphatic hydrops in patients with Ménière’s disease: correlation with audiovestibular function. Eur Arch Otorhinolaryngol 268(12):1743–1748
Kantner C, Gürkov R (2012) Characteristics and clinical applications of ocular vestibular evoked myogenic potentials. Hear Res 294:55–63
Maheu M, Alvarado-Umanzor JM, Delcenserie A, Champoux F (2017) The clinical utility of vestibular-evoked myogenic potentials in the diagnosis of Ménière's disease. Front Neurol 8:415 1-5
Colebatch JG, Rosengren SM, Welgampola MS (2016) Vestibular-evoked myogenic potentials. Handb Clin Neurol 2016(137):133–155
Kumar K, Bhat JS, Sequeira NM, Bhojwani KM (2015) Ageing effect on air-conducted ocular vestibular evoked myogenic potential. Audiol Res 5(2):121
Shabana M, Hassan M, El-Manawee SH, El-Kilany N (2016) Cervical vestibular evoked myogenic potential: its age-related changes. Adv Arab Acad Audiovest J 3(2):51–57
Chihara Y, Iwasaki S, Fujimoto C, Ushio M, Yamasoba T, Murofushi T (2009) Frequency tuning properties of ocular vestibular evoked myogenic potentials. Neuroreport 20(16):1491–1495
Håkansson B, Jansson KF, Tengstrand T, Johannsen L, Eeg-Olofsson M, Rigato C, Dahlström E, Reinfeldt S (2018) VEMP using a new low-frequency bone conduction transducer. Med Devices (Auckl) 11:301–312
Piker EG, Jacobson GP, Burkard RF, McCaslin DL, Hood LJ (2013) Effects of age on the tuning of the cVEMP and oVEMP. Ear Hear 34(6):65–73
Jerin C, Berman A, Krause E, Ertl-Wagner B, Gürkov R (2014) Ocular vestibular evoked myogenic potential frequency tuning in certain Menière’s disease. Hear Res 310:54–59
Zhang AS, Govender S, Colebatch JG (2012) Tuning of the ocular vestibular evoked myogenic potential (oVEMP) to air- and bone-conducted sound stimulation in superior canal dehiscence. Exp Brain Res 22(3):51–64
Noij KS, Herrmann BS, Rauch SD, Guinan JJ Jr (2017) Toward optimizing vestibular evoked myogenic potentials: normalization reduces the need for strong neck muscle contraction. Audiol Neurootol 22:282–291
Møller MB (1994) Audiological evaluation. J Clin Neurophysiol 11(3):309–318
Soliman SM (1976) Speech discrimination audiometry using Arabic phonetically-balanced words. Ain Shams Med J 27:27–30
Li C, Layman AJ, Carey J, Agrawal Y (2015) Epidemiology of vestibular evoked myogenic potentials: data from the Baltimore longitudinal study of aging. Clin Neurophysiol 126:2207–2215
Maleki M, Jafari Z, Zarrinkoob H, Akbarzadeh Baghban A (2014) Effect of aging on saccular function. Med J Islam Repub Iran 28:117
Walther LE, Westhofen M (2007) Presbyvertigo-aging of otoconia and vestibular sensory cells. J Vestib Res 17:89–92
Park JJ, Tang Y, Lopez I, Ishiyama A (2001) Age-related change in the number of neurons in the human vestibular ganglion. J Comp Neurol 431:437–443
Fu W, Han J, He F et al (2021) Effect of stimulus frequency on air-conducted vestibular evoked myogenic potentials. J Int Adv Otol 17(5):422–425
Chihara Y, Iwasaki S, Ushio M, Murofushi T (2007) Vestibular-evoked extraocular potentials by air-conducted sound: another clinical test for vestibular function. Clin Neurophysiol 118(12):2745–2751
Rosengren SM, Govender S, Colebatch JG (2011) Ocular and cervical vestibular evoked myogenic potentials produced by air- and bone-conducted stimuli: comparative properties and effects of age. Clin Neurophysiol 122(11):2282–2289
Murnane OD, Akin FW, Kelly KJ, Byrd S (2011) Effects of stimulus and recording parameters on the air conduction ocular vestibular evoked myogenic potential. J Am Acad Audiol 22(7):469–480
Node M, Seo T, Miyamoto A, Adachi A, Hashimoto M, Sakagami M (2005) Frequency dynamics shift of vestibular evoked myogenic potentials in patients with endolymphatic hydrops. Otol Neurotol 26(6):1208–1213
Rauch SD, Zhou G, Kujawa SG, Guinan JJ, Herrmann BS (2004) Vestibular evoked myogenic potentials show altered tuning in patients with Meniere’s disease. Otol Neurotol 25(3):333–338
Winters SM, Berg IT, Grolman W, Klis SF (2012) Ocular vestibular evoked myogenic potentials: frequency tuning to air-conducted acoustic stimuli in healthy subjects and Ménière's disease. Audiol Neurootol 17(1):12–19
Welgampola MS, Colebatch JG (2001) Characteristics of tone burst-evoked myogenic potentials in the sternocleidomastoid muscles. Otol Neurotol 22(6):796–802
Todd NP, Rosengren SM, Colebatch JG (2009) A utricular origin of frequency tuning to low-frequency vibration in the human vestibular system? Neurosci Lett 451(3):175–180
Miyamoto A, Seo T, Node M, Hashimoto M, Sakagami M (2006) Preliminary study on vestibular-evoked myogenic potential induced by bone-conducted stimuli. Otol Neurotol 27(8):1110–1114
Sheykholeslami K, Habiby Kermany M, Kaga K (2001) Frequency sensitivity range of the saccule to bone-conducted stimuli measured by vestibular evoked myogenic potentials. Hear Res 160(1-2):58–62
Welgampola MS, Rosengren SM, Halmagyi GM, Colebatch JG (2003) Vestibular activation by bone conducted sound. J Neurol Neurosurg Psychiatry 74(6):771–778
Maxwell R, Jerin C, Gürkov R (2017) Utilisation of multi-frequency VEMPs improves diagnostic accuracy for Meniere’s disease. Eur Arch Otorhinolaryngol 274:85–93
Dudman KP (2022) cVEMP frequency tuning in adults aged 60 and above: a systematic review. CUNY Academic Works
Atabek P (2020) Effects of age and middle ear resonance on the frequency tuning of the cVEMP, p 16 Dissertations, 2020-current
Colebatch JG, Govender S, Rosengren SM (2013) Two distinct patterns of VEMP changes with age. Clin Neurophysiol 124:2066–2068
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
AD was a key contributor to the analysis, interpretation, and drafting of the manuscript. AD contributed significantly to the idea of the work. ZB has significantly influenced how the work is designed. SH made significant contributions to the manuscript’s writing and data collection. HH made significant contributions to the data analysis, writing, and editing of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Participants gave their informed consent once the study received ethical approval from Cairo University’s Research Ethics Committee (code: MS-328-2022u) and was revised.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: the name has been updated.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dabbous, A.O., El Bohy, Z., Helal, S. et al. Age effects on frequency amplitude ratio of cVEMP. Egypt J Otolaryngol 39, 28 (2023). https://doi.org/10.1186/s43163-023-00377-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-023-00377-4