
Abstract
Introduction
Thyroid abscesses are a rare septic complication as the thyroid is innately resistant to infection.
Case presentation
Here, we present a case of a 49-year-old female with history of accidental ingestion of a fish bone, subsequent perforation of the esophagus, and thyroid abscess formation.
Management approach consisted of imaging of the gland followed by upper gastrointestinal endoscopy and surgical thyroidotomy with fish bone extraction.
Conclusion
In this case presentation, we highlight the pathophysiology behind thyroid abscess along with review of offered lines of management of this disease from imaging and procedures of diagnosis to treatment approach of source control by both surgical and conservative approach.
Similar content being viewed by others


Background
Thyroid abscesses are a rare pathology. In the literature, thyroid abscesses linked to suppurative thyroiditis represent only 0.1–0.7% of surgically treated thyroid pathologies [1] where the alimentary system is regarded as a source of thyroid abscesses. We report the etiology of thyroid abscess secondary to a perforating esophageal foreign body.
Case presentation
A 49-year-old female, known case of hypothyroidism on replacement therapy, presented to the emergency department with a 2-week history of progressive neck pain and swelling, associated with dysphagia to solid food. She claimed that her symptoms followed a history of choking on a fishbone.
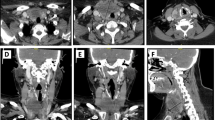
On physical examination, she was not in distress with normal vital signs. Local neck examination revealed a tender and diffusely enlarged right thyroid lobe with normal overlying skin and bilateral palpable mildly tender cervical lymphadenopathy. Laboratory tests revealed elevated white blood cell (WBC) count of 14.2 x 103/uL, C-reactive protein of 65.4 mg/L, and normal thyroid function. The patient was admitted with an initial diagnosis of esophageal perforation due to foreign body ingestion. Computed tomography (CT) of the neck with intravenous contrast was performed (shown in Figs. 1, 2, and 3) which revealed a linear foreign body (fishbone) in the right thyroid lobe and soft tissue enhancement with minimal fluid collection in the retropharyngeal space. Management consisted of infection control with intravenous antibiotics and evaluation of the airway/digestive system. Laryngoscopy revealed a normal pyriform fossa without signs of retropharyngeal collection. Esophagoscopy revealed grossly normal healed esophageal mucosa at the presumed site of foreign body penetration. Surgical exploration revealed congestion and edema of the thyroid tissue with a 2 × 1 cm pus cavity containing the foreign body (shown in Fig. 4) in the right thyroid lobe. Routine collar incision was performed to access the right thyroid lobe. After mobilization of the lobe, pus was drained, the fishbone was extracted, and thyroid gland tissue was preserved.

CT scan neck with right thyroid lobe foreign body with surrounding fluid collection

CT scan neck: liner foreign body resembling fish bone

CT scan neck: sagittal view of the foreign body within the fluid collection

Gross appearance of fish bone
The postoperative course was uneventful, and the patient was discharged on the second postoperative day with oral antibiotics. On follow-up after 1 month, she was asymptomatic with a healed wound.
Discussion
Perforation of the esophagus is a well-recognized entity with potentially serious morbidity estimated to be 12% [2] and mortality of 2.1% in a pooled analysis [3]. Its causes may be iatrogenic, traumatic, spontaneous, or foreign body ingestion. Foreign body ingestion in the adult population is less frequent than in the pediatric group [4], as majority are accidental and related to food. A slightly higher incidence of foreign body ingestion has been found in individuals with underlying psychiatric diseases or alcohol intoxication [5]. According to current statistics, the most common foreign bodies requiring intervention are meat and fish bones (54% and 39%, respectively) [6], and esophageal perforation due to ingestion of foreign bodies occurs in less than 1% of patients [4].
Perforations usually occur in correlation with esophageal anatomical constrictions, including of the cervical esophagus, which is the most common site of penetration, followed by the upper thoracic esophagus [7].
Although the alimentary tract constitutes a part of the neck, it is an uncommon source of thyroid pathology. The thyroid gland has unique anatomical and physiological characteristics, making it resistant to infection including a rich blood supply and lymphatic drainage, a high glandular content of iodine with bactericidal potential, and segregation of the gland due to total encapsulation from other structures of the neck [8]. Therefore, abscess formation is mainly attributed to suppurative thyroiditis [9]. Direct trauma from foreign bodies and extension from neighboring anatomical structures accounts for a minority of cases [10].
Laryngoscopy can play an essential role in the presence of acute symptoms of airway compromise secondary to impacted foreign bodies early in the disease course, or secondary to compression by infected swelling or established abscess later. In asymptomatic patients, laryngoscopy can be used as an adjunct tool to diagnose, localize, and evaluate the epiglottis and vocal cord preoperatively.
Esophagoscopy remains the mainstay diagnostic tool for esophageal perforation, with a sensitivity of 100% and specificity of 83% [11]; however, caution should be exercised in selected cases (e.g., an acute history of hours to days and poor patient general condition) as air insufflation can enlarge the perforation.
The latest guidelines for the management of esophageal perforation recommend emergent flexible endoscopy, preferably within 2 h or at latest within 6 h (Grade 1 B), to search for sharp-pointed objects, batteries, magnets, or other foreign bodies [12]. The period between perforation and esophagoscopy can affect the sensitivity and specificity of the test; a finding of grossly normal esophageal mucosa can be encountered after perforation secondary to the migration of the foreign body to the adjacent structures, which may necessitate further diagnostic modalities to reach a diagnosis.
Radiographs are useful for assessing the presence of foreign bodies, their location, or the development of complications. In a prospective single-center study on 358 adult patients with symptomatic fish bone foreign body impaction, the sensitivity of computed tomography (CT) was 90–100% and the specificity was 93.7–100% [13]. Current guidelines recommend CT scans in cases where perforation or other complications may require interventional endoscopy or surgery (Grade 1B) [12]. In this case, CT was the main modality for diagnosing the complication of thyroid abscess formation, along with assessment of the esophagus and evaluation of the presence of perforation. Additionally, CT scans are accurate in diagnosing other esophageal perforation complications such as mediastinitis or aortic/tracheal fistulas [14].
Management is guided toward the acute presentation or sequelae of the perforation, such as the formation of a thyroid abscess. Delays in management carry the risk of septicemia, retropharyngeal abscess, tracheal rupture, internal jugular vein thrombosis, vocal fold paralysis, and suppurative mediastinitis [15]. Management of thyroid abscesses in the literature has been recommended through case series and case reports, but no standardized treatment has been established, ranging from conservative management to total thyroidectomy. Source control is performed by draining the abscess through an incision made over the thyroid gland (thyrotomy). The disadvantage of this technique is that it leaves an inflamed thyroid gland near the source of the infection. However, resection of the diseased part of the thyroid gland is needed to prevent the inflamed gland tissue and pus material from extending to the recurrent laryngeal nerve, causing inflammatory neuritis, and subsequently vocal cord paralysis [16]. Aggressive management with total thyroidectomy has been reported as a treatment for thyroid abscess, although it is seldom used due to complications of hormonal deficiency and risk of recurrent laryngeal nerve injury.
Conclusion
Formation of thyroid abscess secondary to digestive tract entry point require a low threshold of work up that includes CT scan imaging as well as upper gastrointestinal endoscopy and laryngoscopy. This should be followed by prompt management that range from thyroid drainage up to total thyroidectomy. The intervention of choice remains an area of deliberation and are ultimately left to the surgeon’s decision, especially in such rare cases.
Availability of data and materials
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
References
Chen CY, Peng JP (2011) Esophageal fish bone migration induced thyroid abscess: case report and review of the literature. Am J Otolaryngol Head Neck Med Surg 32(3):253–255
Markar SR, Mackenzie H, Wiggins T et al (2015) Management and outcomes of esophageal perforation: a national study of 2,564 patients in England. Review. Am J Gastroenterol 110:1559–1566
Biancari F, D'Andrea V, Paone R, Di Marco C, Savino G, Koivukangas V, Saarnio J, Lucenteforte E (2013) Current treatment and outcome of esophageal perforations in adults: systematic review and meta-analysis of 75 studies. World J Surg 37(5):1051–1059
Menegaux F, Biro G, Schatz C, Chigot JP (1991) Thyroid abscess: apropos of 5 cases. Ann Med Interne (Paris) 142:99–102
Webb WA (1995) Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc 41:39
Libânio D, Garrido M, Jácome F, Dinis-Ribeiro M, Pedroto I, Marcos-Pinto R (2018) Foreign body ingestion and food impaction in adults: better to scope than to wait. United Eur Gastroenterol J 6(7):974–980
Goh BK, Tan YM, Lin SE et al (2006) CT in the preoperative diagnosis of fish bone perforation of the gastrointestinal tract. Am J Roentgenol 187:710–714
Herndon MD, Christie DB, Ayoub MM, Duggan AD (2007) Thyroid abscess: case report and review of the literature. Am Surg 73:725–728
Bhattacharrya S, Miller J, Ropper AH (2014) The case for case reports. Ann Neurol 76(4):484–486
Hazard JB (1995) Thyroiditis: a review—part I. Am J Clin Pathol 25:289–298
Horwitz B, Krevsky B, Buckman RF Jr, Fisher RS, Dabezies MA (1993) Endoscopic evaluation of penetrating esophageal injuries. Am J Gastroenterol 88(8):1249–1253
Chirica M, Kelly MD, Siboni S, Aiolfi A, Riva CG, Asti E et al (2019) Esophageal emergencies: WSES guidelines. World J Emerg Surg 14(1):26
Ngan JH, Fok PJ, Lai EC et al (1990) A prospective study on fish bone ingestion. Experience of 358 patients. Ann Surg 211(4):459–462
Young CA, Menias CO, Bhalla S et al (2008) CT features of esophageal emergencies. Radiographics 28(6):1541–1553
Boyd CM, Esclamado RM, Telian SA (1997) Impaired vocal cord mobility in the setting of acute suppurative thyroiditis. Head Neck 19:235–237
Myssiorek D, Lee J, Shikowitz M et al (2000) Immobile vocal fold secondary to thyroid abscess: a case eport. Ear Nose Throat J 79:453–455
Acknowledgements
None
Funding
None
Author information
Authors and Affiliations
Contributions
N.Z: data collection and data interpretation. A.S: study design. H.O: data interpretation and reviewer. A.Z: drafting. Y.T: reviewer. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was waived for this study in accordance with the Dubai Health Authority Research Committee policies. Informed consent was obtained from the patient.
Consent for publication
Written consent to publish obtained from the patient for his/her images and other clinical information to be reported in the journal. The patient informed that name and initial will not be published and due effort is made to conceal their identity.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
AlZarouni, N., Saber, A., Omar, H. et al. Thyroid abscess due to ingested fish bone, endoscopic, and surgical approach: a case presentation. Egypt J Otolaryngol 38, 163 (2022). https://doi.org/10.1186/s43163-022-00350-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00350-7