
Abstract
Background
Study the pathological features, extent of treatment, and epidemiological distribution of laryngeal carcinoma among Egyptian female patients.
Results
The study population consisted of 34 female patients treated for laryngeal cancer at the Otolaryngology Department, Faculty of Medicine, Cairo University, between 2011 and 2017. The data were collected in a retrospective manner, based on the analysis of patients’ medical records. The mean age of the total cohort is 56.5 years. Twenty-six patients (76.5%) had supraglottic carcinoma, 7 patients (20.5%) had glottic carcinoma, and only 1 patient (3%) had subglottic tumor. The regional disease of the neck affected 18% of the patients. Ninety-one percent of the patients showed a moderate degree of tumor differentiation.
Conclusion
There may be important gender differences in laryngeal sub-site incidence for patients with laryngeal carcinoma.
Similar content being viewed by others


Background
Laryngeal carcinoma has long been described as a disease of chronic heavy smokers with long history of alcohol intake. Change in disease epidemiology trends has occurred to involve rapid rise in the incidence of the illness among female population. One report described the increase in laryngeal carcinoma among females to be tripled. Over 15 years, the male-to-female ratio has dropped from 5.6:1 to 4.5:1 [1].
In light of changing socials norms in the Egyptian population, the incidence of cigarette and water-pipe smoking has increased from 1.4 to 2.8% between 2005 and 2009. The increase in smoking habits comes to affect adolescent females rather than adult women [2].
Gender difference has also been claimed to affect the laryngeal unit where laryngeal carcinoma originates. A report described predominance of supraglottic tumors among females, while the glottis was the most common site for male patients [3].
Debate has been ongoing regarding the role of steroid sex hormone receptors distribution among normal larynx and laryngeal carcinoma specimens to explain this sub-site difference with some reports confirming the presence of this link suggesting a role for hormonal therapy in the treatment while others failed to agree with this finding [4, 5].
The aim of this study is to investigate the pathological features, extent of treatment, and epidemiological distribution of laryngeal carcinoma among Egyptian female patients
Methods
The medical records of Egyptian females diagnosed with laryngeal squamous cell carcinoma treated at tertiary care practice of the Otolaryngology Department, Faculty of Medicine, Cairo University, between 2011 and 2017 were retrospectively reviewed.
This study was approved by the ethical committee for scientific research at the Otolaryngology Department, Cairo University, and the approval carries the number: 21802R.
Patients with unavailable medical records or incomplete pathological characteristics from the available medical records were excluded from this study. Patients with pathology other than laryngeal squamous cell carcinoma were not candidates in this study. Of the 451 patients with laryngeal carcinoma, 36 patients were female. Two female patients with laryngeal adenoid cystic carcinoma were excluded from the study, and 34 female patients met the inclusion criteria.
The epidemiological distribution of the study cohort, i.e., the age and year of the diagnosis was discussed. All the pathological events (TNM staging, degree of differentiation, site of the primary tumor, subglottic invasion, thyroid cartilage invasion, extra-laryngeal spread, margin invasion, thyroid gland invasion, hostile pathological features “vascular invasion, peri-neural invasion and/or extra-capsular spread”) were incorporated into the analysis. For patients who had concurrent hemithyroidectomy or total thyroidectomy with the laryngectomy, the presence of a 2nd primary in the thyroid gland was determined from the final pathology report. The extent of surgical treatment of the study cohort (total or partial laryngectomy, concurrent total, or partial thyroidectomy and concurrent neck dissection) was reviewed.
Statistical methods
Data were coded and entered using the statistical package SPSS version 25 (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). Data was summarized using mean and standard deviation for quantitative variables and frequencies (number of cases) and relative frequencies (percentages) for categorical variables.
Results
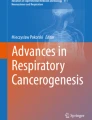
The medical records of this study consisted of 34 female patients with mean age 56.5 years (range: 34–75 years). Patients were sub-classified according to age groups, as shown in Fig. 1. There were 3 patients (8.8%) aged 30 to 39 years, 4 patients (11.7%) aged 40 to 49 years, 13 patients (38.2%) aged 50 to 59 years, 9 patients (26.5%) aged 60 to 69 years, and 5 patients (14.8%) aged 70 to 79 years.

Distribution of 34 female cases of laryngeal cancer according to age group
Of the total cohort (n = 34), 31 patients (91%) had moderately differentiated laryngeal carcinoma (grade 2), 2 patients (6%) had poorly differentiated laryngeal carcinoma (grade 3), and 1 patient (3%) had well differentiated laryngeal carcinoma (grade 1).
Twenty-six patients (76.5%) had supraglottic carcinoma, of whom 9 patients were stage III and 17 patients were stage IV; 7 patients (20.5%) had glottic carcinoma, of whom 3 patients were stage III and 4 patients were stage IV; and only 1 patient (3%) had stage IV subglottic tumor (Fig. 2).

Distribution of site of carcinoma by stage of disease
Primary treatment in this study varied between total laryngectomy (n = 28) and supra-cricoid partial laryngectomy (n = 6). Table 1 shows the distribution of primary treatment according to the tumor stage.
Total thyroidectomy was performed in 20% of patients (7/34), hemithyroidectomy was done in 62% of patients (21/34), and no thyroid surgery was needed in 6 patients (18%). On review of the pathological specimens in patients who underwent thyroid surgery with the primary treatment, six patients had direct thyroid gland invasion by squamous cell carcinoma (17.6%). Interestingly, two patients had incidental second thyroid malignancy, papillary thyroid carcinoma, and Hurthle cell carcinoma.
Bilateral neck dissection was performed in 7 patients, ipsilateral neck dissection was done in 18 patients, and management of the primary tumor only was performed in 9 patients. None showed distant metastases and six patients (18%) had neck metastases (2 patients with N1; 3 patients with N2b; and 1 patient with N2c). The six patients with neck metastases had the primary tumor in the supraglottic area (Table 2). Two of the remaining patients (n = 28) showed non-malignant features of lymph nodes, sarcoid granulomatous lymph nodes, and sinus histocytosis.
Discussion
The incidence rates of laryngeal carcinoma are considerably lower among the female patients [6,7,8,9]. We report 34 female patients—who met the inclusion criteria—with laryngeal carcinoma; 38.2% were in the fifth decade of life, and these results are in accordance with the report of Garham and Palmer [10].
In the majority of cases in this study, the tumor was supraglottic (76.5%), but in 7 patients (20.5%), the tumor was restricted to the glottic area and only 1 patient (3%) had a stage 4 subglottic laryngeal carcinoma. These results are consistent with the study of Kokoska and his colleagues which was conducted on 40 female patients [11] and in discordance to a previous study by Shvero and his colleagues who concluded that the glottic area is the most common laryngeal sub-site affected by the laryngeal carcinoma [12].
In the present report, supraglottic carcinoma constituted the most common site for laryngeal carcinoma in the study population. An epidemiological study conducted by Peller and associates described the demographic distribution of laryngeal carcinoma among the German population. The incidence of laryngeal carcinoma in the female population was 1652 during the period between 1998 and 2011. The main primary subset for tumor origin was the glottis (50%). Their findings come in accordance with the previously reported literature [12]. The incidence remained stable during the study period in contrast to the male population which showed decline starting 2006. This decline reflects the change in the smoking pattern among the German society; however, the relative stability of the disease incidence among female population calls for possible presence of other factors that may contribute to the disease incidence in females [13].
A recent study was conducted over 50 laryngectomy specimens to demonstrate the role of sex hormones in the development of laryngeal caner. This is stemmed from the notion that the larynx is a secondary sex organ that undergoes changes with puberty reflecting the presence of sex hormone receptors which play the role in the physiological changes of puberty. Estrogen receptor B and progesterone receptors were found to be significantly associated with poorly differentiated tumors and malignancies with lymphatic invasion. On the contrary, androgen receptors showed significantly lower expression in poorly differentiated tumors and cancers with lymphatic invasion. Estrogen receptors B and progesterone receptors were thus considered as markers of aggressive tumor biology [14].
Some of the distribution disparity between laryngeal sub-sites could be attributed to differences in smoking and drinking habits between men and women. It is possible that that the greater prevalence of supraglottic tumors in females is due to the influence of steroid hormones, but it is unclear at this time how this effect might be exerted.
Notwithstanding the tendency to high-grade tumors in the supraglottis, 91% of the female patients in this study showed a grade 2 laryngeal squamous cell carcinoma. This is reinforced with the results of Stephenson and his colleagues [3].
In disparity to this study that reported that the majority of female patients with laryngeal carcinoma presented with advanced stage laryngeal carcinoma; 22 patients (64.7%) presented with stage IV and 12 patients (35.5%) presented with stage III; another retrospective study of 96 laryngeal carcinoma female patients showed that 68.8% of the female patients presented in an early stage of the disease [11].
Stell in 1990 found that 50% of affected females developed neck metastasis, but in this study, we found only an 18% incidence, mostly from supraglottic carcinoma [15]. This may be explained by the fact that the majority of our cohort showed well to moderate degree of differentiation (grades 1 and 2).
The main limitation of the present analysis is the small sample size due to the rarity of the disease among women. Another important factor is that we were unable to obtain data regarding the social habits (smoking and alcohol intake) among the study population, highlighting the importance of preoperative documentation. As a consequence, we were also unable to report data about the survival rates and the prognosis.
The main strength of this study is that it reports the largest number of female patients reported in the Egyptian literature. Also, the study was conducted over a relatively adequate time range (7 years). Our population included patients with locally advanced laryngeal tumors only facilitating analysis and future comparison of gender differences affecting only this specified patient population.
Conclusion
Based on our results, the most common laryngeal sub-site affected by laryngeal carcinoma in Egyptian females is the supraglottis. There may be important gender differences in sub-site incidence for patients with laryngeal carcinoma. Despite having locally advanced disease, most patients showed moderate degree of tumor differentiation. Regional disease of the neck affected less than 20% of the patients.
We recommend that this study to be conducted separately with larger and dedicated studies. This study recommends that when designing and analyzing the results from clinical studies of laryngeal carcinoma, it may be significant to use stratification based on gender.
Availability of data and materials
All data generated or analyzed during this study had already been included in this manuscript. Patient’s case file was retrieved from the medical record section of the institution. The clinical data had been collected from the prospectively maintained computerized database and the case file. The follow-up status was updated from the above-mentioned manner.
References
Derienzo DP, Greenberg SD, Fraire AE (1991) Carcinoma of the larynx: changing incidence in women. Arch Otolaryngol Neck Surg 117(6):681–684. https://doi.org/10.1001/archotol.1991.01870180117023
El Awa F, Fouad H, El Naga RA, Emam AH, Labib S (2013) Prevalence of tobacco use among adult and adolescent females in Egypt. East Mediterr Health J 19(08):749–754. https://doi.org/10.26719/2013.19.8.749
Stephenson WT, Barnes DE, Holmes FF, Norris CW (1991) Gender influences sub-site of origin of laryngeal carcinoma. Arch Otolaryngol Head Neck Surg 117(7):774–778 http://archotol.jamanetwork.com/
Virolainen E, Tuohimaa P, Aitasalo K, Kyttä J, Vanharanta-Hiltunen R (1986) Steroid hormone receptors in laryngeal carcinoma. Otolaryngol Neck Surg 94(4):512–517. https://doi.org/10.1177/019459988609400419
Hagedorn HG, Nerlich AG (2002) Analysis of sex-hormone-receptor expression in laryngeal carcinoma. Eur Arch Oto-Rhino-Laryngol 259(4):205–210. https://doi.org/10.1007/s004050100400
Robin PE, Reid A, Powell DJ, McConkey CC (1991) The incidence of cancer of the larynx. Clin Otolaryngol Allied Sci 16(2):198–201
Stell PM (1990) Prognosis in laryngeal carcinoma: host factors. Clin Otolaryngol Allied Sci 15(2):111–119
Majszyk D, Bruzgielewicz A, Osuch-Wójcikiewicz E, Rzepakowska A, Niemczyk K (2019) Gender-related incidence, risk factors exposure and survival rates of laryngeal cancers – the 10-years analysis of trends from one institution. Polish Otolaryngol 73:6–10
Igissinov N, Zatoskikh V, Moore MA, Igissinov S, Aldiyarova G, Tokmurziyeva G, Valieva S, Alpeissova S, Sarsenova S (2013) Laryngeal cancer in Kazakhstan-ethnic, age and gender differences over time. Asian Pac J Cancer Prev 14(11):7033–7037
Graham MS, Palmer AD (2002) Gender difference considerations for individuals with laryngectomies. Contemp Issues Commun Sci Disord 29(Spring):59–67
Kokoska MS, Piccirillo JF, Haughey BH (1995) Gender differences in cancer of the larynx. Ann Otol Rhinol Laryngol 104(6):419–424
Shvero J, Hader T, Feinmesser R, Har-El G, Martin D, Marshak G, Segal K (1996) Laryngeal carcinoma in females. Eur J Surg Oncol (EJSO) 22(1):61–64
Peller M, Katalinic A, Wollenberg B, Teudt IU, Meyer JE (2016) Epidemiology of laryngeal carcinoma in Germany, 1998–2011. Eur Arch Otorhinolaryngol 273(6):1481–1487
Shoffel-Havakuk H, O'Dell K, Johns MM III, Reder L, Popova M, Halperin D, Feldberg E, Lahav Y (2020) The rising rate of nonsmokers among laryngeal carcinoma patients: are we facing a new disease? Laryngoscope 130(3):E108–E115
Stell PM (1990) Prognosis in laryngeal carcinoma: tumor factors. Clin Otolaryngol Allied Sci 15(1):69–81
Acknowledgements
None. This study was conducted using the available resources at Cairo University Hospitals. No author identifying information is present anywhere in the blinded manuscript.
Funding
This research did not receive any special grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
A M. E made substantial contributions to the conception or design of the manuscript and data collection. A A. N made substantial contributions to the data collection and manuscript writing and gave final approval of the manuscript version to be published. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study involved human subjects. All the procedures that involved human participants were performed in accordance with standards set by the Swedish Research Ethical Review Authority and with the 1964 Helsinki Declaration and its later amendments. This study was approved by the ethical committee for scientific research at the Otolaryngology Department, Cairo University, and the approval carries the number: 21802R. Consent to participate is not required since it is a retrospective study.
Consent for publication
Not applicable as our manuscript does not contain any individual person’s data in any form (including individual details, images, or videos).
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eltelety, A.M., Nassar, A.A. Analysis of the pathological characteristics of locally advanced laryngeal carcinoma in Egyptian females: 7-year review. Egypt J Otolaryngol 38, 37 (2022). https://doi.org/10.1186/s43163-022-00230-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00230-0