
Abstract
Background
Children with sensorineural hearing loss (SNHL) form a major chunk of the population with hearing difficulty. Since the auditory system is close to the vestibular system and shares the common fluid, the abnormality in the auditory system might impair the functioning of the vestibular system.
Main body of the abstract
The present systematic review aimed at studying the application of cervical and ocular vestibular evoked myogenic potential responses (cVEMP and oVEMP) during assessment and rehabilitation of children with SNHL with and without a cochlear implant. A systematic search was done across databases on cVEMP and oVEMP findings in children with SNHL. Out of 92 articles retrieved, 21 articles were found to be appropriate as per our inclusion criteria. Significant vestibular abnormality was seen in children with SNHL as shown on cVEMP and oVEMP test reports. The cVEMP and oVEMP abnormalities seen were more in children with SNHL using a cochlear implant. Pre- and post-implantation studies showed a significant reduction in measures of cVEMP and oVEMP after implantation.
Short conclusions
Studies in the last decade reported abnormal cVEMP and oVEMP response in children with SNHL with and without cochlear implantation. cVEMP and oVEMP response is also associated with poor motor development in children with SNHL. Thus, emphasis should be given to assessing vestibular functioning in children with SNHL to rehabilitate them early in life.
Similar content being viewed by others


Background
Sensorineural hearing loss (SNHL) is commonly seen as hearing loss due to the inner ear or the vestibulocochlear nerve damage. Literature review suggests SNHL accounts for 90% of reported hearing loss which is permanent and varies in severity from mild to profound hearing loss [1]. Recent studies reported the importance of studying the relationship between peripheral vestibular function and cochlear function, underlined by the fact that the cochlea and vestibular systems are anatomically, phylogenetically, and functionally related [2]. Hence, disturbances in cochlear function, which can result in SNHL, could accompany vestibular impairment because of sharing the membranous labyrinth of the inner ear with the vestibule. Prenatal, natal, or postnatal injury may cause damage to one or both the systems leading to SNHL [3,4,5].
Early detection of vestibular dysfunction in the pediatric population is important. If the vestibular dysfunction goes undiagnosed and untreated, this would result in significant motor impairment [6] and inability to maintain stable gaze [7], thus affecting their scholastic performance. Although a small proportion of these individuals with SNHL exhibit concurrent vestibular involvement, it is important to identify the impairment and rehabilitate them [8]. From birth onwards, auditory stimulation directs and intensifies visual orientation behavior in infants and the infant’s earliest responses to auditory stimuli include the visual-motor behavior of moving the eyes or head to localize sound. Therefore, it has been suggested that lack of early auditory input could contribute to motor delays in children with hearing impairment [9]. Several published reports also suggest the influence of vestibular dysfunction on the gross motor development of individuals with SNHL [10, 11]. One of the audiological tests to assess the functioning of the vestibular system is vestibular evoked myogenic potential (VEMP).
VEMP is a short latency electromyographic and neurophysiological assessment technique that can be recorded from various muscles in response to the acoustic stimulus [12, 13]. There are two types of VEMP, cervical VEMP (cVEMP) and ocular VEMP (oVEMP). oVEMP measures the functioning of the utricle and superior vestibular nerve whereas cVEMP measures the functioning of the saccule and the inferior vestibular nerve [14]. oVEMP is an excitatory myogenic response recorded mainly from the contralateral extraocular muscles [15]. cVEMP is an ipsilateral inhibitory response recorded from the sternocleidomastoid muscle [15]. VEMP recording is considered a simple and rapid method which is patient-friendly and easily implementable in a clinical setup [16]. Both cVEMP and oVEMP are found to be reliable tools in children [17,18,19].
The key to the management of children with SNHL is early diagnosis and early intervention which primarily includes amplification devices and cochlear implantation along with speech and language intervention to facilitate the child’s overall communication ability. Children with SNHL show vestibular system dysfunction as highlighted by the published reports. Many of the researchers have shown abnormal cVEMP and oVEMP results in children with SNHL [8, 20,21,22,23]. Reports also suggest vestibular dysfunction in children with SNHL using cochlear implants [24,25,26]. Since there are many published reports in the last decade highlighting the cVEMP and oVEMP results in children with SNHL, we aimed to compile all the reports relevant to children with SNHL with and without CI and VEMP results. This systematic review aims to explore the application of VEMPs during the assessment and rehabilitation of children with SNHL with and without CI.
Methods
Study design
We performed a systematic literature review of articles published on cVEMP and oVEMP in children with SNHL with and without cochlear implants (CI). A written study protocol was prepared following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [27].
Search strategy
We systematically performed a search in PubMed, Google Scholar, Wiley Online Library, and Google databases for the cVEMP and oVEMP data in the last 10 years (January 2010 to December 2020). The collective search strategy was incorporated and executed independently by both the researchers with no imposed data limits upon the search. In December 2020, a structured computerized search was performed. The keywords, phrases, and MeSH terms searched included the following: “cVEMP in Children with SNHL,” “oVEMP in Children with SNHL,” “cVEMP in Children using Cochlear implants,” and “oVEMP in Children using Cochlear implants.” The search was limited to articles published in English. Furthermore, articles with systematic review and meta-analyses on this topic helped us to identify additional articles, which got missed in our database search. Table 1 shows the number of articles retrieved on cVEMP and oVEMP in children with SNHL with and without CI.
Inclusion and exclusion criteria
The inclusion criteria included a sufficient and accurate description of pathologies, their clinical features, and VEMP recording. Studies performed on children up to the age of 18 years were only considered. The articles on cVEMP and oVEMP in children with SNHL with and without CI were included. The exclusion criteria included articles published before the year 2010, repeated studies or overlapping citations in databases, studies other than in children with SNHL, and test findings other than VEMP. All the articles considered had investigated cVEMP/oVEMP/both in children with and without CI.
Data extraction
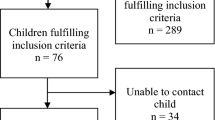
The literature search was independently conducted by both the reviewers. The articles collected by both the reviewers were analyzed for study design, participant’s characteristics, test measures used, and the result of the tests. The inclusion and the exclusion criteria were kept in mind before considering the articles for review, and in case of discrepancy in opinion between the reviewers, the full-text article was reviewed again by both the reviewers and a mutual decision was taken. Figure 1 shows the PRISMA flow chart of the literature review process considered in this study.

PRISMA flow chart of the literature review process
Ethical consideration
The study was approved by the Institutional Ethical Committee. Informed consent from the participants was not applicable as no human subjects were directly involved for this study as this is a review article.
Results
Overall, the primary search yields a total of 92 articles. Independent screening of abstracts and titles of the articles was performed. The inclusion and exclusion principles adopted in the study resulted in 21 articles for cVEMP and oVEMP. Some of the articles investigated both the cVEMP and oVEMP responses while others had either of the cVEMP or oVEMP responses.
cVEMP and oVEMP in children with SNHL
Many of the researchers have studied the characteristics of cVEMP and oVEMP in children with hearing loss [8, 20, 22, 28,29,30]. Table 2 shows the summary of the cVEMP and oVEMP studies on children with SNHL. Singh et al. recorded cVEMP response in 15 children with severe to profound hearing loss and 10 children with normal hearing [22]. Of the 15 children with SNHL, cVEMP response was absent in 2 (13%) of the individuals. The latencies of P13 and N23 responses did not show a significant difference whereas peak-to-peak amplitude showed a significant difference across the groups. Said showed absent cVEMP response bilaterally in more than 45% of children with SNHL, 12% in unilateral SNHL, and delayed cVEMP responses in 20% of individuals with SNHL [8]. The percentage of abnormal/absent cVEMP response was higher in children with a higher degree of SNHL compared to a lesser degree of hearing loss [8, 31]. cVEMP abnormality seen in children with profound SNHL varied from 56% in bilateral pathology to 16% for unilateral pathology. cVEMP responses are present for the lesser degree of hearing loss and are usually absent for the profound degree of SNHL. Zhou et al. in a retrospective study found 54% of the children with different degrees of SNHL to have abnormal cVEMP responses [28].
Xu et al. reported a response rate of 58.1% and 61.9% for oVEMP and cVEMP respectively in children with profound SNHL. There was a significant reduction in amplitude and elevation in the threshold of oVEMP and cVEMP in children with profound hearing loss compared to healthy children [29]. Researchers have also observed a significant difference in cVEMP response in children with severe-to-profound hearing loss with and without auditory neuropathy spectrum disorder [30, 32]. The study suggests a positive correlation between saccular dysfunction and ANSD in children with severe-to-profound hearing. Apeksha et al. reported the absence of cVEMP and oVEMP response in 27% of the children with severe-to-profound hearing loss [20]. Even though none of the children or their parents report difficulty in performing their daily living activity, the Fukuda stepping test and the Tandem gait test showed abnormal results suggesting a compromised balance system. Kegel et al. and Inoue et al. suggested a combination of rotatory chair testing and VEMP testing to be used for children with SNHL to predict the balance performance in them [10, 11].
Based on the above-mentioned studies, it is clear that a significant number of children with SNHL show vestibular system abnormality as shown in VEMP results. The VEMP abnormalities seen were reduction in amplitude of the peaks, prolongation in latencies of the peaks, and increase in the VEMP thresholds and the majority of the children showed complete absence of VEMP response [20, 21, 33]. Researchers believe that it is the anatomic compartmentalization of vestibular end organs and the cochlea that are likely to show an abnormality in both cochlear and vestibular function. It is because of the proximity of the structures that the saccule show more significant abnormality followed by utricle and the semicircular canals in individuals with SNHL [34, 35]. Some researchers also suggested more debilitating symptoms in individuals having both cochlear as well as vestibular damage compared to individuals with only cochlear damage [36]. Children who showed abnormal VEMP response also showed significantly delayed acquisition of head control and sitting and independent walking [10, 11]. Recent studies reported abnormal VEMP findings in most of the hearing-impaired children with no reported vestibular symptoms which may be due to the inability to report or describe the dizziness as they are too young to describe it [20]. Saccular impairment in isolation might not cause vestibular disturbances in children as the input from the impaired vestibular system might get compensated by the central component. Studies also suggest that the abnormality seen on cVEMP and oVEMP responses correlates well with the degree of hearing loss [8, 31].
cVEMP and oVEMP in children with SNHL using the cochlear implant
Several researchers have explored the functioning of the vestibular system in children with SNHL using CI using cVEMP and oVEMP responses. The majority of the published reports suggest an adverse effect of CI on the functioning of the vestibular system post-implant [23,24,25,26, 37]. Table 3 shows the summary of the cVEMP and oVEMP studies on children with SNHL using CI.
Xu et al. found the response rate of cVEMP and oVEMP to be 67.7% and 71% before the CI surgery in children with SNHL [23]. After 1 month of CI surgery, the response rate decreased to 32% and 12.9% respectively for cVEMP and oVEMP. For children in whom the cVEMP and oVEMP responses were recorded, the response showed a reduction in amplitude of peaks and elevation in thresholds suggesting significant damage to the vestibular system. In another study, VEMP response was abnormal in 60% of the children pre-operative and became 100% abnormal 6 months post-operative in the implanted ear [38]. In a group of children implanted unilaterally and planned to undergo contralateral implantation, Devroede et al. showed the presence of cVEMP response in 79% of the children pre-operatively and 62% post-operatively [39]. Thierry et al. reported normal VEMP response in six children, partial dysfunction bilaterally in four children, and asymmetrical vestibular function in two children pre-implantation. Post-implantation, six children had the same vestibular result; four children showed improvement in vestibular symptoms after surgery, and two children showed worsening of symptoms [26].
Imai et al. investigated the functioning of otolith organs before and after CI. cVEMP results showed an increase in asymmetry ratio in 5 out of 9 children 1 month postoperatively indicating deterioration in sacculo-collic response post-CI [25]. oVEMP results showed an increased asymmetry ratio for 10 out of 11 children with CI, indicating deterioration of utriculo-ocular response postoperatively. The majority of the researchers reported significant deterioration of cVEMP and/or oVEMP response in children with CI, except one of the studies [40]. Ajalloueyan et al. recorded cVEMP response in 27 children with severe to profound hearing loss [40]. The researchers reported no statistically significant difference in cVEMP response pre-post implantation.
Li et al. also observed otolith dysfunction in 35 children with CI, suggesting VEMP be one of the reliable tools to assess the functioning of otolith organs post-implantation [24]. Merchant et al. compared cVEMP and oVEMP elicited by air conduction and bone conduction stimuli to check the hypothesis that it is not the actual vestibular loss but the mechanical changes by the CI that leads to the absence of VEMP response in children with CI [37]. Bone-conduction VEMP response rate was higher than the air-conduction VEMP responses suggesting that it is the mechanical property of the peripheral system which gets altered with CI surgery and leads to an air-bone gap rather than the actual vestibular loss in children with CI [37]. Many researchers reported alteration in the intracochlear pressure and peripheral mechanics as the cause of the persistent air-bone gap in individuals with CI [41,42,43].
Researchers in the field have no clear justification for the effect of CI on the non-implanted side. Katsiari et al. reported either absent or abnormal VEMP responses after CI surgery on the non-implanted side of the children with SNHL [44]. Similarly, Psillas et al. also reported abnormal VEMP responses in the non-implanted ear of children with CI [38]. This finding may be supported by the hypothesis that the abnormal responses on the non-implanted side might be a consequence of abnormal input of the vestibular system on both sides. With the insertion of the CI electrodes in one ear, the vestibular input to the brain gets altered in the same ear and indirectly modifies the contralateral ear vestibular response. Despite abnormal VEMP findings seen in children with CI, none of the children reports dizziness or vertigo [20, 38]. This could be attributed to the capacity of the children to compensate for the peripheral vestibular loss by the process of central compensation.
The vestibular system is found to be at risk for damage following CI surgery because of the anatomical proximity of vestibular and cochlear systems [37]. The significant damage caused to the inner ear structures includes fibrosis in the vestibule, the collapse of the saccule, decrease in ganglion cells, inner ear hydrops, and scar tissues [34, 45]. Obeidat et al. reported otolith organs to be more affected than the semicircular canals [35]. Of the two otolith organs, the saccule is the most vulnerable site for damage following CI surgery than the utricle [34]. This is explained based on the proximity of the saccule to the cochlea where electrodes are inserted and can easily damage the saccule.
Conclusions
Most of the recent studies in the last decade reported abnormal cVEMP and oVEMP responses in children with SNHL. The functioning of the vestibular system gets even more impaired following CI surgery. This suggests that CI has a more negative impact on the functioning of the vestibular structures. Vestibular dysfunction seen in children with SNHL may slow down their motor development and thus can delay the motor milestones. So we must assess the child’s audio-vestibular system early in life to rehabilitate them early. It is also important that we screen all the children with SNHL for vestibular impairment irrespective of the degree and cause of SNHL.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SNHL:
-
Sensorineural hearing loss
- cVEMP:
-
Cervical vestibular evoked myogenic potentials
- oVEMP:
-
Ocular vestibular evoked myogenic potentials
- CI:
-
Cochlear implant
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- ANSD:
-
Auditory neuropathy spectrum disorders
References
Smith RJH, Bale JF, White KR (2005) Sensorineural hearing loss in children. Lancet 365:879–890. https://doi.org/10.1016/S0140-6736(05)71047-3
Rajendran V, Roy FG, Jeevanantham D (2013) A preliminary randomized controlled study on the effectiveness of vestibular-specific neuromuscular training in children with hearing impairment. Clin Rehabil 27:459–467. https://doi.org/10.1177/0269215512462909
Pajor A, Jozefowicz-Korczynska M (2008) Prognostic factors for vestibular impairment in sensorineural hearing loss. Eur Arch Otorhinolaryngol 265:403–407. https://doi.org/10.1007/S00405-007-0473-Z
Wilson WR, Byl FM, Laird N (1980) The efficacy of steroids in the treatment of idiopathic sudden hearing loss. A double-blind clinical study. Arch Otolaryngol 106:772–776. https://doi.org/10.1001/archotol.1980.00790360050013
Kaga K (1999) Vestibular compensation in infants and children with congenital and acquired vestibular loss in both ears. Int J Pediatr Otorhinolaryngol 49:215–224. https://doi.org/10.1016/S0165-5876(99)00206-2
Rine RM, Cornwall G, Gan K et al (2000) Evidence of progressive delay of motor development in children with sensorineural hearing loss and concurrent vestibular dysfunction. Percept Mot Skills 90:1101–1112. https://doi.org/10.2466/pms.2000.90.3c.1101
Braswell J, Rine RM (2006) Evidence that vestibular hypofunction affects reading acuity in children. Int J Pediatr Otorhinolaryngol 70:1957–1965. https://doi.org/10.1016/j.ijporl.2006.07.013
Said EA (2014) Vestibular assessment in children with sensorineural hearing loss using both electronystagmography and vestibular-evoked myogenic potential. Egypt J Otolaryngol 30:43. https://doi.org/10.4103/1012-5574.127203
Savelsbergh GJP, Netelenbos JB, Whiting HTA (1991) Auditory perception and the control of spatially coordinated action of deaf and hearing children. J Child Psychol Psychiatry 32:489–500. https://doi.org/10.1111/j.1469-7610.1991.tb00326.x
Kegel A, Maes L, Baetens T et al (2012) The influence of a vestibular dysfunction on the motor development of hearing-impaired children. Laryngoscope 122:2837–2843. https://doi.org/10.1002/lary.23529
Inoue A, Iwasaki S, Ushio M et al (2013) Effect of vestibular dysfunction on the development of gross motor function in children with profound hearing loss. Audiol Neurotol 18:143–151. https://doi.org/10.1159/000346344
Colebatch JG, Halmagyi GM, Skuse NF (1994) Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry 57:190–197. https://doi.org/10.1136/jnnp.57.2.190
Zhou G, Cox LC (2004) Vestibular evoked myogenic potentials. Am J Audiol 13:135–143. https://doi.org/10.1044/1059-0889(2004/018)
Manzari L, Tedesco A, Burgess AM et al (2010) Ocular vestibular-evoked myogenic potentials to bone-conducted vibration in superior vestibular neuritis show utricular function. Otolaryngol Neck Surg 143:274–280. https://doi.org/10.1016/j.otohns.2010.03.020
Rosengren SM, Kingma H (2013) New perspectives on vestibular evoked myogenic potentials. Curr Opin Neurol 26:74–80. https://doi.org/10.1097/WCO.0b013e32835c5ef3
Papathanasiou ES, Murofushi T, Akin FW et al (2014) International guidelines for the clinical application of cervical vestibular evoked myogenic potentials: an expert consensus report. Clin Neurophysiol 125:658–666. https://doi.org/10.1016/J.CLINPH.2013.11.042
Young Y-H, Chen C-N, Hsieh W-S et al (2009) Development of vestibular evoked myogenic potentials in early life. Eur J Paediatr Neurol 13:235–239. https://doi.org/10.1016/j.ejpn.2008.04.008
Erbek S, Erbek SS, Gokmen Z et al (2007) Clinical application of vestibular evoked myogenic potentials in healthy newborns. Int J Pediatr Otorhinolaryngol 71:1181–1185. https://doi.org/10.1016/j.ijporl.2007.04.007
Fuemmeler E, Rodriguez AI, Thomas M et al (2020) Vestibular evoked myogenic potential (VEMP) test-retest reliability in children. Otol Neurotol 41:e1052–e1059. https://doi.org/10.1097/MAO.0000000000002703
Apeksha K, Singh S, Rathnamala M et al (2020) Balance assessment of children with sensorineural hearing loss. Indian J Otolaryngol Head Neck Surg 73:12–17. https://doi.org/10.1007/s12070-020-01797-x
Bansal S, Sahni S, Sinha S (2013) Cervical and ocular vestibular evoked myogenic potentials in individuals with severe to profound hearing loss. J Hear Sci 3:56–63
Singh S, Gupta RK, Kumar P (2012) Vestibular evoked myogenic potentials in children with sensorineural hearing loss. Int J Pediatr Otorhinolaryngol 76:1308–1311. https://doi.org/10.1016/j.ijporl.2012.05.025
Xu X, Zhang XT, Zhang Q et al (2014) Ocular and cervical vestibular-evoked myogenic potentials in children with cochlear implant. Clin Neurophysiol 126:1624–1631. https://doi.org/10.1016/j.clinph.2014.10.216
Li X, Gong S (2020) The effect of cochlear implantation on vestibular evoked myogenic potential in children. Laryngoscope 130:E918–E925. https://doi.org/10.1002/lary.28520
Imai T, Okumura T, Ohta Y et al (2019) Effects of cochlear implants on otolith function as evaluated by vestibulo-ocular reflex and vestibular evoked myogenic potentials. Auris Nasus Larynx 46:836–843. https://doi.org/10.1016/j.anl.2019.03.011
Thierry B, Blanchard M, Leboulanger N et al (2015) Cochlear implantation and vestibular function in children. Int J Pediatr Otorhinolaryngol 79:101–104. https://doi.org/10.1016/j.ijporl.2014.11.002
Liberati A, Altman D, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700. https://doi.org/10.1136/bmj.b2700
Zhou G, Dargie J, Dornan B et al (2014) Clinical uses of cervical vestibular-evoked myogenic potential testing in pediatric patients. Medicine (Baltimore) 93:e37. https://doi.org/10.1097/MD.0000000000000037
Xu X, Zhang Q, Hu J et al (2015) The hidden loss of otolithic function in children with profound sensorineural hearing loss. Int J Pediatr Otorhinolaryngol 79:852–857. https://doi.org/10.1016/j.ijporl.2015.03.017
Emami SF, Farahani F (2015) Saccular dysfunction in children with sensorineural hearing loss and auditory neuropathy/auditory dys-synchrony. Acta Otolaryngol 135:1298–1303. https://doi.org/10.3109/00016489.2015.1076169
Selim E-ASM, El-Minawi MS et al (2012) Assessment of saccular function using cervical vestibular-evoked myogenic potentials in children with sensorineural hearing loss. Egypt J Otolaryngol 28:234–241. https://doi.org/10.7123/01.EJO.0000418053.78780.0C
El-Badry M, Samy H, Abdelkader R et al (2019) Cervical vestibular evoked myogenic potential in children with auditory neuropathy spectrum disorder of prelingual onset. Egypt J Ear Nose Throat Allied Sci 20:47–52. https://doi.org/10.21608/ejentas.2019.6389.1055
Jafari Z, Malayeri SA (2011) The effect of saccular function on static balance ability of profound hearing-impaired children. Int J Pediatr Otorhinolaryngol 75:919–924. https://doi.org/10.1016/j.ijporl.2011.04.006
Tien HC, Linthicum FH (2002) Histopathologic changes in the vestibule after cochlear implantation. Otolaryngol - Head Neck Surg 127:260–264. https://doi.org/10.1067/mhn.2002.128555
Obeidat FS, Bell SL, Julie E (2020) An exploration of vestibular function pre and post unilateral cochlear implantation. Cochlear Implants Int 21:281–291. https://doi.org/10.1080/14670100.2020.1774716
Schwab B (2011) Influencing factors on the vestibular function of deaf children and adolescents - evaluation by means of dynamic posturography. Open Otorhinolaryngol J 5:01–09. https://doi.org/10.2174/1874428101105010001
Merchant G, Schulz K, Patterson J et al (2020) Effect of cochlear implantation on vestibular evoked myogenic potentials and wideband acoustic immittance. Ear Hear 41:1111–1124. https://doi.org/10.1097/AUD.0000000000000831
Psillas G, Pavlidou A, Lefkidis N et al (2014) Vestibular evoked myogenic potentials in children after cochlear implantation. Auris Nasus Larynx 41:432–435. https://doi.org/10.1016/j.anl.2014.05.008
Devroede B, Pauwels I, Le Bon SD et al (2016) Interest of vestibular evaluation in sequentially implanted children: preliminary results. Eur Ann Otorhinolaryngol Head Neck Dis 133:S7–S11. https://doi.org/10.1016/j.anorl.2016.04.012
Ajalloueyan M, Saeedi M, Sadeghi M et al (2017) The effects of cochlear implantation on vestibular function in 1–4 years old children. Int J Pediatr Otorhinolaryngol 94:100–103. https://doi.org/10.1016/j.ijporl.2017.01.019
Chole R, Hullar T, Potts L (2014) Conductive component after cochlear implantation in patients with residual hearing conservation. Am J Audiol 23:359–364. https://doi.org/10.1044/2014
Raveh E, Attias J, Nageris B et al (2015) Pattern of hearing loss following cochlear implantation. Eur Arch Otorhinolaryngol 272:2261–2266. https://doi.org/10.1007/s00405-014-3184-2
Mattingly JK, Uhler KM, Cass SP (2016) Air-bone gaps contribute to functional hearing preservation in cochlear implantation. Otol Neurotol 37:1255–1262. https://doi.org/10.1097/MAO.0000000000001171
Katsiari E, Balatsouras DG, Sengas J et al (2013) Influence of cochlear implantation on the vestibular function. Eur Arch Otorhinolaryngol 270:489–495. https://doi.org/10.1007/s00405-012-1950-6
Licameli G, Zhou G, Kenna MA (2009) Disturbance of vestibular function attributable to cochlear implantation in children. Laryngoscope 119:740–745. https://doi.org/10.1002/lary.20121
Acknowledgements
Not applicable.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
KA and DD performed the independent systematic title and abstract search based on the selection criteria, collected the study data independently, and analyzed these data. DD was a major contributor in writing the manuscript. KA and DD both read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Obtained from the JSSISH ethical committee with reference No. JSSISH/2021/P8. Informed consent from the participants was not applicable as no human subjects were directly involved for this study as this is a review article.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Apeksha, K., Devananda, D. Cervical and ocular vestibular evoked myogenic potential in children with sensorineural hearing loss with and without cochlear implant: a systematic review. Egypt J Otolaryngol 38, 21 (2022). https://doi.org/10.1186/s43163-022-00214-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00214-0