
Abstract
Background
Glucose-6-phosphate dehydrogenase (G6PD) deficiency, an X-linked disorder that is more common in males, is the most prevalent blood enzyme deficiency, affecting 5% of the population worldwide. Its prevalence in Saudi Arabia varies greatly from one region to another (4.7% to 12%), and no related data are available for the country’s Al-Qassim region.
Methods
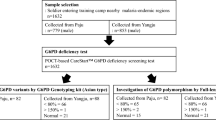
This was a retrospective medical record-based study. Eligible patients were those who visited Dr. Sulaiman Al-Habib Hospital in Al-Qassim, Saudi Arabia, between June 2021 and November 2022, and underwent the test for G6PD enzyme deficiency. The study sample consisted of (n = 313) randomly selected Saudi patients. G6PD enzyme activity was evaluated using spectrophotometry.
Results
The prevalence of G6PD deficiency was 2.9%. The proportion of male patients (100%) was significantly higher than that of female patients. 88.9% of patients with G6PD deficiency experienced episodes of acute hemolysis and reported a history of favism, whereas 77.8% of the patients had a family history of favism.
Conclusion
The prevalence of G6PD deficiency was low in Al-Qassim region of Saudi Arabia.
Similar content being viewed by others


Introduction
Glucose-6-phosphate dehydrogenase (G6PD) plays a key role in oxidative stress [1]. The most prevalent blood enzymatic deficiency, impacting millions of people globally, is G6PD deficiency. Some studies estimated that G6PD deficiency affects about 5% of the world’s population, with the highest prevalence of the disease in ethnicities originating from malaria-endemic regions including the Mediterranean region, Middle East, Asia, and Africa. According to growing epidemiological evidence, patients with G6PD deficiency are protected from severe malaria. This could be because G6PD deficiency causes more oxidative stress in red blood cells, which could make it difficult for parasites to reproduce [2, 3]. G6PD deficiency in erythrocytes is an X-linked recessive disorder that results in hemolytic anemia, affecting males more often than females. Females who are homozygous or phenotypically deficient heterozygotes (due to lyonization) can have mild symptoms but are mostly asymptomatic [4, 5]. Hemolytic episodes are mostly induced by certain drugs or the consumption of certain foods, such as fava beans [5, 6].
G6PD deficiency can be diagnosed through various ways, such as a screening test using a qualitative enzyme assay (a fluorescent spot test), quantitative assays measuring the activity of the G6PD enzyme using spectrophotometry, or genetic molecular testing using polymerase chain reaction (PCR) to confirm the diagnosis [2]. Several mutations have been described for the G6PD gene, some of which have different impacts on enzymatic activity and result in various clinical manifestations in patients [6, 7]. Hemolytic anemia and jaundice are the most frequent manifestations in the neonatal [8, 9]. In order to prevent future hemolytic episodes, it is essential to educate patients about unsafe diets and medications. The key to managing G6PD deficiency is avoiding oxidative stress, such as exposure to specific medications or consumption of specific foods including fava beans. Although most acute hemolysis is self-limited, it can occasionally be so severe that a blood transfusion is required. G6PD deficiency is among the most prevalent genetic hematological disorders in the Middle East and particularly in Saudi Arabia [10]. Saudi Arabia is a large country with a population of approximately 35 million people, and continuous investigations are needed to monitor the prevalence of G6PD deficiency [10]. The prevalence of G6PD deficiency in Saudi Arabia varies regionally. G6PD deficiency rates of 12% in Riyadh, 17% in Dammam, and 4.7% in Taif were demonstrated in some studies conducted in Saudi Arabia [3, 10, 11]. This indicates a wide variation in the prevalence of G6PD deficiency between regions and countries. Studying the prevalence of G6PD deficiency in Al-Qassim region of Saudi Arabia is currently of interest. Therefore, the present study aimed to assess the prevalence of G6PD deficiency in Al-Qassim region of Saudi Arabia.
Methods
Patients and study design
This retrospective study utilized the medical record data of 313 patients screened for G6PD deficiency in inpatient and outpatient settings at a private hospital (Dr. Sulaiman Al-Habib Hospital) in Al-Qassim region of Saudi Arabia. According to the General Authority for Statistics 2020, the region's population is estimated to be 1.4 million. The study was carried out in January 2023. The test was administered to those for whom it was indicated, and everyone was included, including males and females who visited the hospital between June 2021 and November 2022. The inclusion criteria were randomly chosen male and female Saudi patients who underwent G6PD testing for G6PD activity (using the UDI kit, Dammam, Saudi Arabia), using a quantitative photometric system (UV/kinetic), and results reported in terms of units of enzyme activity per gram of hemoglobin. The normal expected values are 5.0–16.4 U/gHb. The following indications for ordering the test were a history of neonatal jaundice; unexplained Coombs negative hemolytic anemia; a strong family history of G6PD deficiency; or prior administration of certain medications with a high risk of G6PD deficiency. There were no sex, age, or body mass index limitations. Patients with malignancies or other hematological disorders were excluded from the study.
A 6 ml venous blood sample was extracted in tubes with anticoagulants, such as ethylenediamine tetraacetic acid (EDTA), heparin, or acid-citrate-dextrose (ACD), and processed within 24 h of collection. The medical files of the recruited patients were retrieved, and data related to demographic characteristics, G6PD level, complete blood count (CBC), hemolysis workup (lactate dehydrogenase (LDH), bilirubin, and peripheral blood film), and clinical findings were obtained. Patients with low G6PD levels were contacted by phone for more detailed information. According to WHO sex-based criteria, anemia is described as a hemoglobin level lower than 130 g/L for men and lower than 120 g/L for women.
The ethical approval was obtained from the Research Ethics Committee of the Al Habib Research Center, Saudi Arabia (study number # RC23.01.02). All personal information collected, including the participants’ names, were kept confidential. The study participants' consent waiver was due to using completely de-identified data with no associated risk to the participants. All procedures performed and patient confidentiality were in compliance with the ethical standards of the institution, the National Research Committee in KSA, and the Helsinki Declaration.
Statistical analysis
The Statistical Package for Social Sciences, version 26 (SPSS, IBM, TX, USA) was utilized for analyzing the data. Data were examined for accuracy and missing information. Frequencies are reported for categorical variables. A contingency table was created for the whole sample. Subsequently, the analysis was limited to patients with G6PD deficiency. The proportions by age and sex were compared and contrasted using Chi-square statistics (significance p < 0.05). Finally, the laboratory, morphological, and clinical characteristics were displayed in tabular form.
Results
A total of 313 patients were included in the current study: 180 males (57.5%) and 133 females (42.5%). Most were infants (83.7%) or adults older than 16 years old (14.1%). All patients were Saudi as shown in Table 1. A total of 56 patients were excluded because they were non-Saudi.
The prevalence of G6PD deficiency was 2.9%, and males were the only affected sex (5% vs. 0%, p = 0.011). Moreover, the prevalence of G6PD deficiency varied by age group as the age group of 1–16 years had the highest prevalence followed by the 16 + age group and infants (5.7%, 4.5%, and 1.1%, respectively) (Table 2).
All patients with G6PD deficiency, except one, demonstrated laboratory evidence of hemolysis, as displayed in Table 3, including low hemoglobin levels and high levels of lactate dehydrogenase, reticulocyte count, and total bilirubin.
88.9% of the patients had a personal history of favism, while 77.8% had a family history of favism. Chronic diseases were present in only 22.2% of the cases, and asthma was the only reported chronic disease. Hemolytic crisis and jaundice were present in 88.9% of the patients, as illustrated in Table 4.
Discussion
G6PD deficiency is among the most common enzymatic deficiencies in Saudi Arabia. Among the 313 patients screened in the current study, 2.9% were diagnosed with G6PD deficiency. G6PD deficiency was observed only in males. G6PD deficiency is more common among males because it is an X-related genetic disorder [7, 9].
G6PD deficiency occurs in a wide range of ethnic groups worldwide. It has been found in as many as 28% of people in southwestern Nigeria, 1–10% of Indians, 20–30% of Greeks, 1–17% of Saudi Arabians, and 5.5% of people in South China [12, 13]. Even in Saudi Arabia, the prevalence of G6PD deficiency varies from region to region. Alqahtany revealed that the prevalence of G6PD deficiency was 12% in randomly chosen samples in Riyadh City [3]. Alharbi et al. reported a frequency of G6PD deficiency of 4.7% in healthy male Saudi blood donors from Taif [11]. Al-Ali et al. demonstrated the highest percentages of G6PD deficiency among the populations of the Eastern Province of Saudi Arabia in Al-Qatif (45.9%) and Al-Hassa (36.5%) [14]. G6PD deficiency was found in 0.78% of blood donors in Riyadh, as per Alabdulaali et al. [15]. In the current study, the prevalence of G6PD deficiency was relatively low (2.9%), when compared to other previous studies carried out in KSA. This could be explained by the fact that the diagnostic test utilized was a fluorescent spot test, which has been demonstrated to have low sensitivity to measure G6PD activity at intermediate levels. Thus, it can miss a significant proportion of G6PD deficiency at intermediate levels when compared to spectrophotometry, which is the gold standard for diagnosing G6PD deficiency [16]. Moreover, studies that found the deficiency rate to be less than 5% included samples from blood donors. It is worth mentioning that blood donors undergo rigorous screening before donating and blood is only collected from healthy donors. However, a different sampling strategy and recruitment from different hospitals would result in a better representation and greater sample variation, hence giving a different result. As in the present study, the majority (73.7%) of the recruited patients were infants and from one hospital only.
G6PD deficiency is characterized by the destruction of red blood cells, leading to increased hemoglobin catabolism and a reduction in blood hemoglobin levels, followed by increased activity in the bone marrow, reticulocyte count, bilirubin, and lactate dehydrogenase levels [17,18,19]. In the current study, 88.9% of patients with G6PD deficiency experienced hemolytic crises. It has been reported that the most common type of G6PD deficiency mutation in Saudi Arabia is the Mediterranean type, resulting in severe hemolysis [20]. Patients were found to have an increase in the percentage of reticulocytes, total bilirubin levels, blood lactate dehydrogenase levels, and clinical jaundice. Only one patient, despite having a low G6PD level, did not have any signs of hemolytic anemia. This could be explained by the fact that the G6PD gene has more than 180 different known mutations, and these variants have diverse impacts on enzymatic activity, resulting in various clinical manifestations in patients [21]. In the current study, 88.9% of patients with G6PD deficiency, or 2.6% of all enrolled patients, experienced favism. This is a low prevalence when compared to a previous study conducted by Almutairi in Dammam which reported a prevalence of favism among 17% of all enrolled patients [10, 22]. Despite having a smaller sample size (182) compared to that in the current study (313), a higher prevalence of favism was reported. This can also be explained by the nature of the study, as the study conducted by Almutairi utilized online surveys to collect data while the current study collected data from patients visiting hospitals.
Hemolytic crises were reported in 88.9% of the patients. Initially, favism was a term utilized for describing hemolytic crises followed by the ingestion of fava beans. However, it is currently utilized for describing G6PD deficiency [10, 22]. Favism was reported in 88.9% of patients with G6PD deficiency, and a family history of favism was reported in 77.8%.
In the present study, we investigated the prevalence of G6PD deficiency in Al-Qassim region of Saudi Arabia and the frequency of hemolysis in patients with G6PD deficiency. We also compared the prevalence with that in other studies. However, the current study has some limitations. For instance, it is very difficult to extrapolate the results to the entirety of Saudi Arabia because the study was retrospective and patients were recruited from only one region. On the other hand, it is the first study of its kind to be conducted in Al-Qassim region, and it utilized quantitative assays (spectrophotometry) to measure the activity of the G6PD enzyme, which is more sensitive than a qualitative enzyme assay (fluorescent spot test).
Conclusions
The prevalence rate of glucose-6-phosphate dehydrogenase (G6PD) deficiency is relatively low (2.9%) in Al-Qassim region of Saudi Arabia. Most of the patients (88.9%) experienced hemolytic crisis, jaundice, reduced hemoglobin levels, and reticulocytosis. Future research is needed to identify the prevalence of G6DP in the general population and determine whether routine G6PD level testing should be performed on all newborns to facilitate early detection and management.
Availability of data and materials
All data and materials used in this current study are available from the corresponding author on reasonable request.
References
Cantú-Reyna CJ, Santos-Guzmán H, Cruz-Camino DL, Vazquez Cantu R, Gómez-Gutiérrez JJ, Góngora-Cortéz A et al (2019) Glucose-6-Phosphate dehydrogenase deficiency incidence in a Hispanic population. J Neonatal Perinatal Med 12(2):203–207
DelFavero JJ, Jnah AJ, Newberry D (2020) Glucose-6-Phosphate Dehydrogenase Deficiency and the Benefits of Early Screening. Neonatal Netw 39(5):270–282
Qahtany, A. and F.S. Abdullah, Recent trends of glucose-6-phosphate dehydrogenase deficiency among Saudi population in Riyadh city. Biosci. j.(Online), 2019: p. 1979–1984.
Sarkar A, Rohilla M, Kumari S (2022) Concurrence of glucose-6-phosphate dehydrogenase deficiency in pregnancy. J Obstet Gynaecol 42(5):747–750
Luzzatto L, Nannelli C, Notaro R (2016) Glucose-6-Phosphate Dehydrogenase Deficiency. Hematol Oncol Clin North Am 30(2):373–393
Frank JE (2005) Diagnosis and management of G6PD deficiency. Am Fam Physician 72(7):1277–1282
Cappellini MD, Fiorelli G (2008) Glucose-6-phosphate dehydrogenase deficiency. Lancet 371(9606):64–74
Celik HT, Gunbey C, Unal S, Gumruk F, Yurdakok M (2013) Glucose-6-phosphate dehydrogenase deficiency in neonatal hyperbilirubinaemia: Hacettepe experience. J Paediatr Child Health 49(5):399–402
Kaplan M, Hammerman C (2011) Neonatal screening for glucose-6-phosphate dehydrogenase deficiency: biochemical versus genetic technologies. Semin Perinatol 35(3):155–161
Almutairi MKO, Alsayyid AAH, Abo El-Fetoh NM (2018) Glucose-6-Phosphate Dehydrogenase Deficiency (G6PD) (Favism) in Dammam, Eastern Province of Saudi Arabia. EgyptJ Hosp Med 70(5):713–717
Alharbi KK, Khan IA (2014) Prevalence of glucose-6-phosphate dehydrogenase deficiency and the role of the A− variant in a Saudi population. J Int Med Res 42(5):1161–1167
May J, Meyer CG, Großterlinden L, Ademowo OG, Mockenhaupt FP, Olumese PE et al (2000) Red cell glucose-6-phosphate dehydrogenase status and pyruvate kinase activity in a Nigerian population. Tropical Med Int Health 5(2):119–123
Gupte, S.C., A. Shaw, and K. Shah, Hematological findings and severity of G6PD deficiency in Vataliya Prajapati subjects. JAPI, 2005. 53.
Al-Ali A (1996) Common G6PD variant from Saudi population and its prevalence. Ann Saudi Med 16(6):654–656
Alabdulaali MK, Alayed KM, Alshaikh AF, Almashhadani SA (2010) Prevalence of glucose-6-phosphate dehydrogenase deficiency and sickle cell trait among blood donors in Riyadh. Asian J Transfus Sci 4(1):31
Halim, S.A., R. Bahar, W.Z. Abdullah, and E. Mohamad, Performance Comparison between Conventional Fluorescent Spot Test and Quantitative Assay in Detecting G6PD Deficiency.
Kaplan M, Wong RJ, Stevenson DK (2018) Hemolysis and Glucose-6-Phosphate Dehydrogenase Deficiency-Related Neonatal Hyperbilirubinemia. Neonatology 114(3):223–225
Karafin MS, Fu X, D’Alessandro A, Thomas T, Hod EA, Zimring JC et al (2018) The clinical impact of glucose-6-phosphate dehydrogenase deficiency in patients with sickle cell disease. Curr Opin Hematol 25(6):494–499
Motulsky AG (1972) Hemolysis in glucose-6-phosphate dehydrogenase deficiency. Fed Proc 31(4):1286–1292
Warsy AS, El-Hazmi MA (2001) G6PD deficiency, distribution and variants in Saudi Arabia: an overview. Ann Saudi Med 21(3–4):174–177
May WL, Kyaw MP, Blacksell SD, Pukrittayakamee S, Chotivanich K, Hanboonkunupakarn B et al (2019) Impact of glucose-6-phosphate dehydrogenase deficiency on dengue infection in Myanmar children. PLoS ONE 14(1):e0209204
Luzzatto L, Arese P (2018) Favism and Glucose-6-Phosphate Dehydrogenase Deficiency. N Engl J Med 378(1):60–71
Acknowledgements
The authors would like to thankful to Dr. Sulaiman Al Habib Medical Group’s Research Centre for their tremendous support, and all patients that participated are also gratefully acknowledged.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
AA and IS conceived and designed the study, conducted research, provided research materials, and collected and organized data. NS analysed and interpreted the data. IS wrote the initial draft of the article, AA wrote the final draft of the article, WA and NS provided logistical support. All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ‘Dr. Sulaiman Al Habib Medical Group, Buraidah, Qassim, Saudi Arabia’ (Ethical approval # RC23.01.02). The study participants' consent waiver was due to the use of completely de-identified data with no associated risk to the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
AlShomar, A., Sula, I., Al Abdulmonem, W. et al. Evaluation of the prevalence of glucose-6-phosphate dehydrogenase deficiency in Al-Qassim region of Saudi Arabia. Egypt J Intern Med 35, 68 (2023). https://doi.org/10.1186/s43162-023-00255-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-023-00255-8