
Abstract
Amyloidosis is a rare condition where fibrillar proteins and abnormal, soluble peptides accumulate throughout the body’s organs. Gastrointestinal symptoms secondary to amyloid deposition vary widely and may be confused with other common small intestine diseases, making the diagnosis challenging. Our case is a 63-year-old male with a past medical history of smoking who showed up in the ED with 5 months of diffuse abdominal pain referred to the back. Pelvis-abdominal ultrasound showed bilateral acute pyelonephritis. A colonoscopy revealed large multiple ileal ulcers about 10 cm from the ileocecal valve with a wide base. Pathology biopsies revealed ileal amyloidosis and chronic ileitis with superficial erosions. The patient has been diagnosed with primary localized ileal AL amyloidosis. The patient has finally been referred for surgical resection. We want to raise awareness of ileal amyloidosis and emphasize the importance of considering uncommon etiologies of small intestine pathology in patients presenting with chronic diarrhea, malabsorption, abdominal pain, and weight loss. Finally, patients with small intestine amyloid disease progressing rapidly and failing to respond to non-surgical treatment should be considered for surgical resection.
Similar content being viewed by others


Introduction
Amyloidosis is an unusual disorder characterized by the deposition of abnormal, insoluble peptides and fibrillar proteins in body organs. Nearly every single organ, including the gastrointestinal tract, can be influenced [1]. Gastrointestinal symptoms secondary to amyloid deposition vary widely and may be confused with other common small intestine diseases, making the diagnosis challenging [2]. Here, we present a very rare case of primary localized ileal amyloidosis, which needed surgical resection as a definitive treatment.
Case presentation
A 63-year-old male, not known to be hypertensive nor diabetic, with a past medical history of smoking and NSAIDS abuse showed up in the ED with 5 months of diffuse abdominal pain referred to back, progressive, colicky in nature, increases with eating, decreases with fasting, along with bilious vomiting and offensive watery motions, with no bleeding. Other symptoms include marked weight loss and loss of appetite. The patient denied chest pain, palpitation, and fever. On presentation, vitals were as follows: BP 100/50, pulse: 85 beats/min, RR 16, temperature 37.1 °C. On examination, the patient was awake, alert, and oriented to time, place, and person; however, looked weak and stressed. The heart and lung examinations were unremarkable. Abdomen: soft with mild diffuse tenderness more on the right iliac fossa area without rigidity, distension nor hepatosplenomegaly.
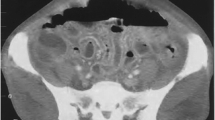
Initial labs were done at the ED and revealed, WBCs 10.91 × 103/mcl (n: 4.8–10.8), Hb 11 g/dl (n: 14–18), Htc 28% (n: 42–52), MCV 83 fl (n: 80–99) PLT:472 × 103/mcl (150–450), Cr 1.2 ESR 1st hour 111, ESR 2nd hour 167, and CRP 12.1 mg/l. The H. Pylori test was positive, and the H. Pylori eradication regimen was started with no improvement. Typhoid and paratyphoid tests were negative. Pelvis-abdominal ultrasound showed bilateral acute pyelonephritis, while urine analysis showed pus in urine 10–15 and urate positive. QuantiFERON TB gold was negative. Colonoscopy revealed large multiple ileal ulcers about 10 cm from the ileocecal valve with wide base, fibrous tissue, and undermined edge, multiple biopsies were taken for histopathological examination which showed active ileitis with extensive ulceration. In setting of clinical, physical, and endoscopic findings, IBD was highly suspected and medical treatment including Solupred 20 mg three times daily, Pentasa 500 mg two tablets three times daily and Imuran 50 mg twice daily were empirically started for 4 weeks without significant improvement. Repeated pelvic abdominal ultrasound showed thickened omentum with multiple mesenteric lymph nodes for clinical correlation. Colonoscopy was repeated and showed diffuse mucosal ileal ulceration with cobblestone appearance, multiple biopsies were taken for histopathological examination (Fig. 1). Pathological biopsies revealed ileal amyloidosis and chronic ileitis with superficial erosions (Fig. 2). The patient was referred to the rheumatology clinic where the following labs have been done ANA: negative, RF and anti-CCP: negative, and bone marrow biopsy which revealed mild hypercellular bone marrow. HRCT chest to exclude any chronic lung diseases didn’t reveal any abnormal findings. Serum amyloid A: 3 (n: 1–10 μg/m), and the FMF gene was normal. Based on the case presentation, physical examination, and previous work up patient has been diagnosed with primary localized ileal amyloidosis. Colchicine 1 mg daily started then titrated to 3 mg daily, metoclopramide, and multiple antibiotics including ciprofloxacin and Flagyl were administered without improvement. Multi-disciplinary round was made, and the patient referred for surgical resection after the persistence of symptoms and instructed to follow-up at the gastroenterology clinic along with the rheumatology clinic with interval screening for possible systemic amyloid deposition in the future. The patient was seen in the clinic 3 months later without any active complaints.

A Multiple large rounded ulcers of variable size surrounded by longitudinal reddish mucosa and granular appearance (ileum). B Multiple yellowish–white polyamide protrusions and thinking of the fold (ilium). C Diffuse friable granular mucosa with easy bleeding with multiple small minute ulcers (jejunum). D By the narrow band: diffuse patchy reddish mucosa was presented along submucosal veins (jejunum)

A, B Ileum with marked lympho-plasmocytic infiltration of the mucosa. Glands are not involved by the inflammation. C, D Amyloid deposition in the ileum submucosa. E, F Congo red stain with polarization shows amyloid deposition in the ileum submucosa
Discussion
Amyloidosis is an uncommon condition that develops when an amyloid protein deposits as insoluble fibrils that alter the structure of tissue. This amyloid buildup affects organ proper functioning. Over 20 different proteins have been identified as forming in vivo amyloid fibrils, but not all of this causes overt disease. Organs that may be affected include the heart, kidneys, liver, spleen, nervous system, and digestive tract [3].
The incidence and prevalence of ileal amyloidosis are not thoroughly reported in the search results provided. However, the prevalence of amyloidosis in patients with inflammatory bowel disease (IBD) is 0.53% (95% confidence interval [CI] 0.32–0.75) [4]. The estimated incidence of primary and secondary systemic amyloidosis is between 5.1 and 12.8 cases per million person-years [5]. The incidence of amyloidosis is estimated to range between five and nine cases per million patient-years worldwide [6]. AL amyloidosis is the most prevalent form of systemic amyloidosis in industrialized nations, with an estimated incidence of 9 cases per million inhabitants per year [7].
Based on the precursor protein that creates the amyloid fibril, classification of amyloidosis is made, and includes AL. Amyloidosis, also known as primary amyloidosis (immunoglobulin light chain amyloidosis). This is the most common type of amyloidosis in developed countries, this disease is associated with subtle clonal dyscrasia of plasma cells or B lymphoid cells [8]. AA amyloidosis, also called secondary amyloidosis is related to chronic inflammation. The acute phase reactant, serum amyloid A protein (SAA), an apolipoprotein component of HDL, is the protein that forms the amyloid fibril. [9]. A2M 2 microglobulin is one of the additional forms of amyloidosis. Long-term dialysis is associated with periarticular and sporadically systemic amyloidosis. ATTR transthyretin in normal plasma systemic amyloidosis in the elderly with significant cardiac involvement and ATTR gene-modified transthyretin systemic amyloidosis that is autosomal dominant Familia Amyloid polyneuropathy [10].
Histopathologic affection in the digestive tract is frequent in patients with systemic amyloidosis, but it is frequently subclinical. In contrast, primary gastrointestinal illnesses, such as IBD, can cause AA amyloidosis, which can lead to systemic amyloidosis. Destruction to the gastrointestinal tract is frequently a part of the involvement of different organs in systemic amyloidosis [11].
Typical clinical manifestations are macroglossia, hemorrhage, motility disorders, bowel habit disturbance, and malabsorption; however, most of which are nonspecific [10]. Also, Wang et al., [12] attested terminal ileum primary amyloidosis as a cause of chronic watery diarrheal motions and weight loss in their case report of a 43-year-old-man after diagnosis has been confirmed by terminal ileum biopsies which showed amyloid deposition illustrated by Congo Red staining.
The affection of the small bowel in systemic amyloidosis can be diffuse or, in rare cases, focal. Some cases of duodenum and jejunum focal amyloidomas with no extraintestinal manifestations have been reported [13].
In 1986, Shimizu et al. [14] reported a case of a 60-year-old patient with primary amyloidosis localized to the small intestine after enteroscopic polypectomy of the small intestine lesions that revealed massive deposition of amyloid in the lamina propria and the submucosa. Li et al. [15], reported a case of a 57-year-old female with past medical history of tuberculosis 30 years ago status post ant tuberculous medications, presented to the gastrointestinal department with diarrhea of 6-month duration, found to have terminal ileum amyloidosis confirmed with biopsy and typical red Congo stain features. In 2022, Wolf et al. [2], reported a case a stricturing lesion at the distal ileum in 60 years old women with past medical history of rheumatoid arthritis and celiac disease presented with abdominal pain and diarrhea diagnosed initially as Crohn’s disease based on the CT findings and the clinical presentation, with progression of symptoms and need for definitive diagnosis a laparotomy and small intestine resection with double barrel end ileostomy formation. The resected ileum’s histopathology revealed evidence of diffuse ulceration, localized, chronic inflammatory mucosa, and trans-mural thickening in Congo red-stained sections, which supported amyloidosis.
Our case demonstrates how small bowel amyloidosis can be similar to Crohn’s disease in the presentation. Here, we want to raise awareness of ileal amyloidosis and emphasize the importance of considering other reasons of small bowel pathology in patients presenting with chronic diarrhea, malabsorption, abdominal pain, and weight loss. Patients with small bowel lesions progressing rapidly and failing to respond to non-surgical treatment should be considered for surgical resection. The best way to successfully manage this uncommon condition is multidisciplinary management.
Conclusion
In conclusion, primary localized ileal amyloidosis is a rare disease that involves the deposition of amyloid protein in the ileum, which can lead to chronic ileitis. This case report highlights the diagnostic challenges associated with this condition, as it can present with nonspecific symptoms and mimic other gastrointestinal disorders. The use of endoscopy with biopsy and Congo red staining is essential for definitive diagnosis.
Availability of data and materials
All data are available with the corresponding author upon request.
Abbreviations
- NSAIDS:
-
Non-steroidal anti-inflammatory drugs
- ED:
-
Emergency department
- BP:
-
Blood pressure
- RR:
-
Respiratory rate
- WBCs:
-
White blood cells
- Hb:
-
Hemoglobin
- MCV:
-
Mean corpuscular volume
- PLT:
-
Platelet
- Ht:
-
Hematocrit
- ESR:
-
Erythrocyte sedimentation rate
- CRP:
-
C-reactive protein
- Cr:
-
Creatinine
- ANA:
-
Anti-nuclear anti-body
- FMF:
-
Familial Mediterranean Fever
- RF:
-
Rheumatoid Factor
References
Bansal R et al (2018) Small bowel amyloidosis. Curr Gastroenterol Rep 20(3):11
Wolf B et al (2022) Amyloidosis of the distal ileum: a stricturing lesion is not always Crohn’s disease. ANZ J Surg 92(3):576–578
Pepys MB (2006) Amyloidosis. Annu Rev Med 57:223–241
Tosca Cuquerella J et al (2016) Amyloidosis in inflammatory bowel disease: a systematic review of epidemiology, clinical features, and treatment. J Crohns Colitis 10(10):1245–1253
Nyirady JH (2021) Primary Systemic Amyloidosis Available from: (https://emedicine.medscape.com/article/1093258-overview)
de Asúa Real et al (2014) Systemic AA amyloidosis: epidemiology, diagnosis, and management. Clin Epidemiol 6:369–77
Desport E et al (2012) AL Amyloidosis. Orphanet J Rare Dis 7(1):54
Kyle RA, Gertz MA (1995) Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol 32(1):45–59
Lachmann HJ et al (2007) Natural history and outcome in systemic AA amyloidosis. N Engl J Med 356(23):2361–2371
Sattianayagam PT, Hawkins PN, Gillmore JD (2009) Systemic amyloidosis and the gastrointestinal tract. Nat Rev Gastroenterol Hepatol 6(10):608–617
Talar-Wojnarowska R, Jamroziak K (2021) Intestinal amyloidosis: clinical manifestations and diagnostic challenge. Adv Clin Exp Med 30(5):563–570
Wang C et al (2013) Chronic diarrhea as the presenting feature of primary systemic AL amyloidosis: serendipity or delayed diagnosis? BMC Gastroenterol 13:71
Mainenti PP et al (2010) Intestinal amyloidosis: two cases with different patterns of clinical and imaging presentation. World J Gastroenterol 16(20):2566–2570
Shimizu S et al (1986) A case of primary amyloidosis confined to the small intestine. Gastroenterol Jpn 21(5):513–517
Li DF, Yao J, Wang LS (2021) Ileal amyloidosis mimicking Crohn´s disease as a cause of chronic diarrhea. Rev Esp Enferm Dig 113(12):855–856
Acknowledgements
None
Funding
None.
Author information
Authors and Affiliations
Contributions
Mahmod Ghoname: case reporter. Hazem Abosheaishaa: discussion, introduction, corresponding author. Mostafa Shehata: case presentation. Mohammed Abdelwahed: pathology diagnosis. Moataz Yousry Soliman: supervision, manuscript revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Consent for publication given by the patient with no identifiable data on the manuscript.
Consent for publication
No IRB approval is required for case report publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ghoname, M., Abosheaishaa, H., Shehata, M. et al. Primary localized ileal amyloidosis with chronic ileitis: a case report with review of literature. Egypt J Intern Med 35, 53 (2023). https://doi.org/10.1186/s43162-023-00237-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-023-00237-w