
Abstract
Background
Diabetes mellitus is a complex chronic disease characterized by chronic hyperglycemia resulting from defective insulin secretion, defective insulin action, or both. Chronic hyperglycemia related to diabetes can lead to end-organ dysfunction or failure, and changes related to diabetes involving arterioles and capillaries are responsible for long-term microvascular complications in diabetic patients. The neutrophil-to-lymphocyte ratio (NLR) is a novel, simple, and inexpensive marker of subclinical inflammation.
Aim of work
To evaluate the possibility that neutrophil-lymphocyte ratio (NLR) could be used as a predictor of microvascular complications during follow-up of elderly patients with type 2 diabetes.
Patients and methods
Sixty elderly diabetes patients ≥ 65 years old, diagnosed 16 according to ADA criteria, were collected from the endocrine clinic in Kasr El-Ainy Hospital. For every patient, full history and examination were done (including 18 neurological and fundus examinations). Labs (CBC with a differential in blood and 19 albumin/creatinine ratio in urine) were done and the neutrophil/lymphocyte ratio.
Results
We found that NLR has a statistically significant difference in the detection of nephropathy and retinopathy. There is a significant correlation between nephropathy and NL ratio in all patients (r = 0.44, P < 0.001). Elderly diabetic patients (with or without hypertension) with microvascular complications had a higher NLR value than those without complications.
Conclusion
NLR value can be used as a non-invasive simple marker for predicting microvascular complications in elderly diabetics with/without hypertension.
Similar content being viewed by others


Background
Diabetes is a complex, chronic disease with multifactorial risk factors. Although glycemic control is an important factor for risk reduction, the prevention and early detection of complications are other factors to reduce both morbidity and mortality.
The global prevalence of diabetes mellitus in adults aged from 20 to 79 years is estimated at 8.8%, with a higher incidence in high-middle-income countries than in low-income countries with the peak incidence at age 65–69 years for men and 75–79 years for women [1].
Type 2 diabetes mellitus can be considered as an age-related disorder; although aging has a minimal effect on insulin action directly, multiple factors in an older person may contribute to hyperglycemia; aging has been thought of as an independent factor associated with low-grade inflammation [2]. As chronic inflammation plays an important role in the development and progression of type 2 diabetes mellitus (T2DM), the role of the inflammatory process in the occurrence and progression of diabetes complications has been demonstrated before when high doses of sodium salicylate administration were found to decrease glycosuria in diabetics [3]. Other inflammatory markers found to be implicated are TLC count, CRP, and interleukin 6 (IL-6) [4].
N/L ratio was found to be associated with an elevation of pro-inflammatory cytokine [5, 6]. So the use of the N/L ratio as a cheap, rapid inflammatory marker for early detection of microvascular diabetic complications (retinopathy, nephropathy, and neuropathy) and rapid early intervention has been very effective and represents a great advance in diabetes management that reduce morbidity incidence as amputation, blindness, and renal failure and also the risk of mortality [7].
Methodology
Aim of the work
Our study aims to prove that NLR could be used as a predictor of microvascular complications during follow-up of elderly patients with type 2 diabetes.
Study design and population
This case-control study was carried out in Kasr Elainy Hospital, Cairo University, Egypt, in the period extending from May 2018 to May 2019. The study included 60 patients of more than 65 years old of both sex, on the presentation full history with full clinical examination taken. The population of the study was divided into two groups: Group A: 30 patients with type 2 diabetes with hypertension and Group B: 30 patients with type 2 diabetes without hypertension.
Lab investigations
-
1.
Blood test (CBC with differential): (NLR) is estimated by dividing the absolute neutrophil ratio by the absolute lymphocyte ratio.
-
2.
Urine test, albumin/creatinine ratio. All patients were surveyed on age, sex, duration of diabetes, chronic disease, family history of diabetes, smoking, and drugs that could affect inflammation like anti-dyslipidemia agents, (NSAIDs), opioids’ analogs, hormonal contraceptives, steroids, immunosuppressive, and immune-modulators drugs.
-
3.
Patients with type 2 diabetes mellitus according to ADA diagnostic criteria, from both sex ≥ 65 years old were included.
-
4.
ADA criteria: HbA1c ≥ 6.5, or FPG ≥ 126 mg/dl (7.0 mmol/L), or 2-h PG ≥ 200 mg/dl (11.1 mmol/L), or a random plasma glucose ≥ 200 mg/dl (11.1 mmol/L) in patients with classic symptoms of hyperglycemia, or hyperglycemic crises.
-
5.
Any patient with acute or chronic infections and inflammatory conditions for the last 2 weeks, chronic heart failure, history of myocardial infarction or coronary artery disease, hematological disorders, autoimmune diseases, cancers, severe liver or kidney disorders, and active smokers were excluded.
Statistical analysis
Data were analyzed using SPSS software version 21 (IBM SPSS, Armonk, NY, USA) and presented as median and range or mean and standard deviation. Comparisons between patients’ groups were analyzed using an independent t test and one-way ANOVA. Pearson’s χ2 was used to determine the significance of associations between categorical variables. A person’s test was used to detect the strength of concordance between two variables. Receiver operating characteristic (ROC) curves were used to assess the diagnostic power of the NL ratio for diabetic complications. P < 0.05 (two-tailed) was considered to indicate a statistically significant difference.
Results
More than 70 patients were seen, but some were not included for many reasons (evidence of current infection, evidence of other chronic infections ex. HCV, abnormal lab test ex. abnormal low platelet count) (Table 1).
There is no statistically significant difference between Groups 1 and 2 respecting the following variables: age, gender, family history, duration of diabetes or hypertension, BMI, patients on single or double oral hypoglycemic drugs (OHD), and patients on aspirin, statin, or insulin.
Regarding the laboratory hematological indices, there was a statistically significant difference in Hb level between Group 1 (12.5 ± 0.9) and Group 2 (13.3 ± 1.3), with a P value of 0.011, while other studies of hematological indices did not differ statistically (P>0.05).
There is no significant difference between the hematological indices of Retinopathy, neuropathy, and nephropathy in the two groups of patients with P values of 0.195, 0.424, and 0.492, respectively (Table 2).
In Group 1, there is a significant association between neutrophil-lymphocyte ratio and retinopathy (P=0.006, Fig. 1), while there is no statistically significant association between NL ratio and neuropathy (P=0.905, Fig. 2). There is a significant association between neutrophil-lymphocyte ratio and macro-albuminuria (P= 0.042, Fig. 3).

The difference in the mean value of NLR in geriatric patients screened for retinopathy in Group 1 (T2DM with HTN) and Group 2 (only T2DM) individually

The difference in the mean value of NLR in geriatric patients screened for neuropathy in Group 1 (T2DM with hypertension) and Group 2 (only T2DM) individually

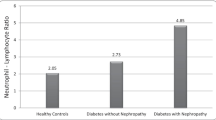
The difference in the mean value of NLR in geriatric patients who screened for nephropathy with A/C ratio in both Group 1 (DM + HTN) and Group 2 (only DM) individually
In Group 2, there was no statistically significant difference relating NLR with retinopathy, neuropathy, or nephropathy with P values 0.268, 0.390, and 0.342, respectively, (Figs. 1, 2, and 3).
There is a significant correlation between nephropathy (a/c) and NL ratio in Group 1 (r = 0.473, P = 0.008). Also, there is a significant correlation between nephropathy (a/c) and NL ratio in Group 2 (r = 0.406, P = 0.026). There is a significant correlation between nephropathy (c/a) and NL ratio in all patients (r = 0.44, P < 0.001, Fig. 4). NLR shows a ~68% sensitivity and ~66% specificity, for detecting retinopathy with a cutoff value of 1.58, in all patients. NLR shows a ~70% sensitivity and ~69% specificity, for detecting retinopathy with a cutoff value of 1.6, in Group 1 patients. NLR shows a ~78% sensitivity and ~70% specificity, for detecting nephropathy with a cutoff value of 1.92, in all patients. NLR shows a ~67% sensitivity and ~71% specificity, for detecting nephropathy with a cutoff value of 1.98, in Group 1 (DM + HTN) patients (Table 3).

Showing the correlation of NLR and DN in T2DM geriatric patients
Discussion
Changes in human behavior and lifestyle over the last century have resulted in a dramatic increase in the incidence of diabetes worldwide [8]. NLR is a new, simple, and cheap marker of subclinical inflammation that has recently been used as a systemic inflammatory marker in chronic disease as well as a predictor of prognosis in cardiovascular diseases and malignancies [7]. Our study showed that elderly diabetic patients (with or without hypertension) with microvascular complications had a higher NLR value than those without complications. These results showed agreement with Öztürk et al., a study conducted on 242 elderly patients with type 2 DM (145 diabetic patients with complications and 97 diabetic patients without complications) and 218 control subjects; this study showed that patients with microvascular complications had higher NLR than patients without complications and controls [7].
Our study showed that NLR is significantly elevated in elderly diabetic patients with nephropathy, to diabetic patients without and this shows agreement with Ciray et al. [9,10,11].
Ateia et al.’s study on 100 patients showed that there is a significant increase in NLR and its relation to albuminuria in the group with macro-albuminuria, compared to the group of those with micro-albuminuria [12]. This comes from our results (Fig. 3).
A meta-analysis study by Liu et al. on 1911 diabetic patients showed that patients with macro-albuminuria (MA) have higher levels of NLR. This indicates that NLR contributes to the development and progression of diabetic nephropathy [13]. Regarding retinopathy, our study revealed that diabetic patients with hypertension and retinopathy had a higher statistically significant NLR. However, the relation between the NLR and retinopathy was statistically insignificant in elderly patients who have only diabetes. This was in agreement with Ciray et al., who targeted 114 patients with diabetes, and showed that NLR did not differ statistically regarding retinopathy [9]. According to Akdoğan et al., in a study that targeted 278 patients with type 2 diabetes and 107 healthy control, their NLR was not affected by retinopathy [14]. However, Öztürk et al.’s and Liu et al.’s studies found a statistically significant difference between NLR and retinopathy in elderly diabetes [7, 13].
As regards the NLR and its relation to neuropathy, our study showed no significant relation between elevated NLR and neuropathy. Onalan et al.’s study that included 100 diabetic patients and 100 controls and Chittawar et al.’s study that included 115 patients with diabetes agreed with our results [15, 16]. However, Öztürk et al.’s study showed a significant difference in relating NLR to peripheral neuropathy in elderly diabetic patients [7]. The disproportionate distribution of the sample was a significant aspect that may have impacted the reliability of our results. Regarding neuropathy, we had 53 of our 60 patients with neuropathy, and thus, only 7 participants were free of neuropathy.
Our results showed that the cutoff value for predicting the microvascular complication in the elderly diabetic for retinopathy and nephropathy were 1.58 and 1.92, respectively; however, Öztürk et al.’s study conducted in Turkey and included 242 elderly diabetes patients showed that the cutoff values for NLR are 2.4 and 2.9 for retinopathy and nephropathy, respectively [7]. This difference might be due to geographical, environmental, and lifestyle differences and also the need for a larger sample size study.
Observing our results between the elderly diabetic with hypertension and the elderly diabetic without hypertension, our study showed that hypertension has a significant effect on the increase of NLR value. This was in concordance with a study done by Imtiaz et al., which measured the NLR as a predictor of systemic inflammation in the prevalent chronic diseases in 1070 of the Asian population and found a significant association between hypertension with high NLR levels [17]. Also, Gang et al.’s study agreed with our result and demonstrated that NLR value increased in hypertensive patients and could predict even it independently by age, sex, body mass index, smoking, drinking, triglyceride, and creatinine [18].
Conclusion
NLR is a simple, cheap tool that could be used as a marker to predict microvascular complications in type 2 geriatric diabetic patients mainly in predicting nephropathy followed by retinopathy. It is advised to take the baseline NLR and follow this up, as our data showed that increased albuminuria (macro-albuminuria compared with micro-albuminuria) had a higher NLR ratio.
Availability of data and materials
Data and materials are available upon request.
Abbreviations
- NLR:
-
Neutrophil to lymphocyte ratio
- CRP:
-
C-reactive protein
- IL-6:
-
Interleukin 6
- CBC:
-
Complete blood count
- NSAIDs:
-
Non-steroidal anti-inflammatory drugs
- ADA:
-
American Diabetes Association
References
Ogurtsova K, da Rocha Fernandes JD, Huang Y, Linnenkamp U, Guariguata L, Cho NH et al (2017) IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 128:40–50
Lee PG, Halter JB (2017) The pathophysiology of hyperglycemia in older adults: clinical considerations. Diabetes Care. 40(4):444–452
Shoelson SE, Lee J, Goldfine AB (2006) Inflammation and insulin resistance. J Clin Invest. 116(7):1793–1801
Dehghan A, Kardys I, De Maat MPM, Uitterlinden AG, Sijbrands EJG, Bootsma AH et al (2007) Genetic variation, C-reactive protein levels, and incidence of diabetes. Diabetes. 56(3):872–878
Tamhane UU, Aneja S, Montgomery D, Rogers E-K, Eagle KA, Gurm HS (2008) Association between admission neutrophil to lymphocyte ratio and outcomes in patients with the acute coronary syndrome. Am J Cardiol. 102(6):653–657
Papa A, Emdin M, Passino C, Michelassi C, Battaglia D, Cocci F (2008) Predictive value of elevated neutrophil-lymphocyte ratio on cardiac mortality in patients with stable coronary artery disease. Clin Chim Acta. 395(1–2):27–31
Öztürk ZA, Kuyumcu ME, Yesil Y, Savas E, Yildiz H, Kepekçi Y et al (2013) Is there a link between neutrophil-lymphocyte ratio and microvascular complications in geriatric diabetic patients? J Endocrinol Invest. 36(8):593–599
Zimmet P, Alberti KG, Shaw J (2001) Global and societal implications of the diabetes epidemic. Nature. 414(6865):782–787
Ciray H, Aksoy A, Ulu N, Cizmecioglu A, Gaipov A, Solak Y (2015) Nephropathy, but not angiographically proven retinopathy, is associated with neutrophil to lymphocyte ratio in patients with type 2 diabetes. Exp Clin Endocrinol Diabetes. 123(05):267–271
Khandare S, Chittawar S, Nahar N, Dubey T, Qureshi Z (2017) Study of neutrophil-lymphocyte ratio as novel marker for diabetic nephropathy in type 2 diabetes. Indian J Endocrinol Metab. 21(3):387
Jaaban M, Zetoune AB, Hesenow S, Hessenow R (2021) Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as novel risk markers for diabetic nephropathy in patients with type 2 diabetes. Heliyon 7(7):e07564
Abdelaziz A, Ahmed E-S, El-Sayed E-SE-ME-SE-M Tarek, Emran M, Abdallah AI et al (2018) Study of neutrophil-lymphocyte ratio (NLR) and platelet lymphocyte ratio (PLR) as a predictor inflammatory marker for diabetic nephropathy in type 2 diabetic patients. Egypt. J Hosp Med. 72(7):4800–4807
Liu J, Liu X, Li Y, Quan J, Wei S, An S, Yang R, Liu J (2018) The association of neutrophil to lymphocyte ratio, mean platelet volume, and platelet distribution width with diabetic retinopathy and nephropathy: a meta-analysis. Biosci Rep. 38(3)
Akdoğan M, Yasemin UB, Huysal K (2016) The association of hematologic inflammatory markers with atherogenic index in type 2 diabetic retinopathy patients. Clin Ophthalmol. 10:1797–1801
Onalan E, Gozel N, Donder E (2019) Can hematological parameters in type 2 diabetes predict microvascular complication development?. Pakistan J Med Sci. 35(6):1511
Chittawar S, Dutta D, Qureshi Z, Surana V, Khandare S, Dubey TN (2017) The neutrophil-lymphocyte ratio is a novel reliable predictor of nephropathy, retinopathy, and coronary artery disease in Indians with type-2 diabetes. Indian J Endocrinol Metab. 21(6):864–870
Imtiaz F, Shafique K, Mirza SS, Ayoob Z, Vart P, Rao S (2012) Neutrophil lymphocyte ratio as a measure of systemic inflammation in prevalent chronic diseases in Asian population. Int Arch Med. 5(1):1–6
Gang L, Yanyan Z (2016) Increased neutrophil to lymphocyte ratio in persons suffering from hypertension with hyperhomocysteinemia. Hypertens Res. 39(8):606–611
Acknowledgements
We acknowledged Prof. Maha Hossam “Prof. of the Internal Medicine and Geriatric, Cairo University,” for her help and guidance in this research, and we are also thankful for the participating patients in this study.
Funding
We declare receiving no funds or grants for this study.
Author information
Authors and Affiliations
Contributions
Dr. Marwa Sayed participated in processing the idea, patients’ collection, statistical analysis, and writing issues. Prof. Sahar Abou-ElEzz participated in processing the idea and follow-up of the main work. Samar Mohsen Kanzel participated in collecting patients, statistical analysis, and writing. Dr. Mohamed Mady Mohamed participated in processing the idea, patient collection, and writing. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of the Internal Medicine Department, Cairo University (21/12/2015).
Consent for publication
This study was approved by the Research Ethics Committee of the Internal Medicine Department, Faculty of Medicine, Cairo University. Written and oral informed consent was obtained from all patients included in the study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eissa, M.S., Abou-ElEzz, S., Kanzel, S.M. et al. Neutrophil-lymphocyte ratio and its relation to microvascular complication in geriatric patients with diabetes: a case-controlled study. Egypt J Intern Med 34, 94 (2022). https://doi.org/10.1186/s43162-022-00185-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-022-00185-x