
Abstract
Background
Chronic kidney disease is a growing worldwide public health concern. On the other hand, patients’ perception of health is an important outcome measure in the assessment of the influence of chronic disease and received treatment. Interest in measuring health-related quality of life has increased together with an awareness that such humanistic outcomes require valid and reliable measures. The aimed study was to evaluate the health-related quality of life (QoL) and to investigate the relationship between selected demographic and clinical characteristics and Health-related Quality of Life (HRQoL) scores in hemodialysis patients.
Methods
This survey study was conducted on hemodialysis patients (209 patients) during the periods 2017–2018. The QoL includes 25 questions classified into five dimensions, which are mobility, personal care, common activities, discomfort and pain, anxiety, and depression. P value < .05 was considered statistically significant.
Results
Overall 209 hemodialysis patients, the mean of the five domains varies from a minimum value of 1.75 ± 1.06 for personal care to a maximum value of 2.65 ± 1.44 for anxiety and/or depression. In our study, among hemodialysis patients is seen a significant association scored between the quality of life and demographic variables like age groups (p = 0.034), and gender (p = 0.01) as in the previous studies. The presence of comorbidities was significantly associated with the QOL (p = 0.001). About the questionnaire, “How good or bad your health is today” the average score resulted to be 47.08 ± 4.5.
Conclusion
As we saw from the results of this study, a considerable number of the patients live with low income. Age, sex, and comorbidities are dependent factors of HRQoL. Therefore, we suggest that future studies include other factors that will evaluate hemodialysis efficiency and find the association between these and QoL.
Similar content being viewed by others


Introduction
Chronic kidney disease (CKD) is a growing worldwide public health concern [1, 2]. It is characterized by an irreversible worsening of renal function that could lead to end-stage renal disease (ESRD), which necessitates treatment with renal replacement therapy (RRT) such as renal transplant or hemodialysis (HD) [3, 4]. According to the 2010 Global Burden of Disease report, Chronic Kidney Disease (CKD) is the 18th most common cause of death [5].
Although the incidence of ESRD has relatively remained stable, the prevalence of maintenance dialysis has almost doubled from 1990 to 2010, increasing from 165 to 284 per million population [6] and is expected to rise even further in the coming decade [7]. By 2030, it is predicted that the number of patients receiving Renal Replacement Therapy (RRT) is expected to reach 5439 million worldwide [7]. Although there exists considerable variability in the choice of appropriate RRT modality all over the world, most patients are treated with in-center hemodialysis (HD), which in most countries exceeds 90% of the incident and 60% of the prevalent ESRD population [8]. Despite numerous advances in the field of RRT, outcomes related to the quality of life and morbi-mortality in ESRD patients have not reached the expected levels. Health-related quality of life (HRQoL) is the individual’s beliefs, experiences, perceptions, and expectations standing for enjoyment in those aspects of life probably influenced by health conditions [9]. HRQoL is identified as a vital health outcome for studies evaluating the quality of healthcare, assessing the influence of illness, and analyses of cost-effectiveness [10, 11]. Lower HRQoL scores lead to a significant risk of hospitalization and mortality.
For dialysis patients and for DM patients, the HRQoL is a significant matter [12, 13], and the degree of her is considerably lower for those patients than for the other people. Furthermore, HRQoL has been discovered to be a forecaster of mortality in both diabetic patients [14] and patients on hemodialysis [15, 16].
The QOL (quality of life) is influenced by socioeconomic status, family life, availability, and utilization of health care facilities. In addition to the increasing numbers of ESRD patients, poverty and exclusion are major problems being faced especially the older persons.
With changing social and economic parameters, research on the quality of life (QOL) is also important [17], because this has direct implications at the individual, community, social, and national levels. The aimed study was to evaluate the health-related quality of life (QoL) and to investigate the relationship between selected demographic and clinical characteristics and health-related quality of life (HRQoL) scores in hemodialysis patients.
Methods
This is a cross-sectional and descriptive survey study conducted on hemodialysis patients (209 patients) during the periods 2017–2018. The inclusion criteria in our study were all the hemodialysis patients who accepted to participate in this investigation, patients over 18 years old, and the patients who had to be medically able to speak, listen, and respond to our questionnaire. A standardized questionnaire was adopted to obtain data from all patients. The questionnaire consisted of four parts. In the first part are included the demographic data, including gender, age, residence area, level of education, marital status, and living condition. In the second part are included the risk factors for hemodialysis patients including BMI (body mass index), alcohol, occupation, and monthly income. In the third part were included the clinical data, including, dialysis data of patients, time of dialysis start, frequency of dialysis, duration of dialysis, and comorbidities. The fourth part deals with questions HRQoL. The World Health Organization Quality of Life Instruments (WHOQoL-BREF), a generic health-related questionnaire developed by the WHOQoL group was selected to quantify the HRQoL of ESRD patients [18]. The Cronbach’s alpha for the scale of QoL resulted in 0.835. A trained person collected the data face to face for each patient, especially for the third part of the questionnaire), and for the questionnaires in which the patients did not answer we attempted to find the record files of hemodialysis patients.
The QoL includes 25 questions classified into five dimensions, which are mobility, personal care, common activities, discomfort and pain, anxiety, and depression. The software SPSS version 20.0, was used to analyze and evaluate the data obtained in this study. Epidemiological data were presented as frequency, percent, mean and standard deviation (x¯±s). t test, unpaired t test, and ANOVA were conducted in the analysis of QoL data. The categorical data were compared using the χ2 test. With multivariable linear regression, we investigate the potential predictors of QoL. P value < .05 was considered statistically significant.
Results
Overall in 209 hemodialysis patients, the average age was 56.64 ± 12. Std deviation with a minimum of age 19 years old and a maximum of 79 years old. The age group between 60 and 69 years old presented the highest number of cases (35.4%) compared to the other age groups. In addition, the age group of 18–39 years old presented the lower number of patients 5.7% (12/209). Males were the most predominant sex compared to females 72.2% (151/209) and 27.8% (58/209) respectively. There was found a significant level between sex for 95% CI, p value < 0.0001. Most of them lived in rural areas 57.4% (120/209) and the other patients lived in urban areas 42.6% (89/209).
Regarding the education level of our patients, 6.7% reported that don’t have got any education, 37.8% have got only primary school, most of them have got secondary education, and only 14.3% of them have completed their university studies. 7.6% (16 cases) of our patients resulted to be single, 68.4% (143 cases) were married, 12.4% (26 cases) were widows and 11.57% (24 cases) were divorced. Regarding the living condition, 75.8 (164 cases) were living with their family and 24.2% (45 cases) were living alone.
Regarding the risk factors for hemodialysis patients, we evaluated their BMI, and 10% of the patients (21 cases) were underweight, 51.2% (107 cases) were of normal weight, 22% (46 cases) were in the category of pre-obese and 16.3% (34 cases) were obese. We asked our patients about their employment status, and the results we received are as below, unemployed 6.7% (14 cases), employed 54.5% (114 cases), retired 31.1% (65 cases), and treated as invalids 7.6% (16 cases).
Regarding the monthly income, it can be mentioned that in Albania, almost all the payments for all categories are done in Lek, the Albanian currency. However, in our study, we have converted the sum of Albanian currency into Euro (European currency). We found out that the minimum l monthly income in this group of patients is less than 200 euros, and most of the patients are living at a low income of 42.1%.
In the categorized moderate living group, only 50.7% of the patients are classified and only 7.2% of the patients are living in the categorized high-income living group in high income with more than 400 euros per month.
Table 1 presents the distribution of epidemiological data, the risk factors, and the correlation between the QoL and general characteristics of hemodialysis patients in Albania. The data are presented as frequency, percentage, mean, and Std. For most of the variables, we have seen a significant association with the QoL used in the evaluation of the quality of life in hemodialysis patients’, participants in this study.
From the data analysis of our dialysis patients, 31.6% of the results originate from renal disease caused by chronic kidney disease; Glomerulonephritis and Pyelonephritis presented in 22.9% and 20.1% respectively, and the other factors are less than 7%. More than half of the patients (59.3%) have more than four years of dialysis and 40.7% less than four years. For the frequency of dialysis, more than 3/4 of them (78.5%) are presented at the dialysis center three or more times during the week and only 21.5% of them have a frequency in the dialysis center two times a week. The duration of dialysis varies from less than 4 h (24.4%) to more than 4 h (78.6%). All patients have related or problems with some comorbidities where 67.9% presented cardiovascular diseases, 41.6% of patients with diabetes mellitus, and with rheumatoid arthritis only 9.1% of the patients. In Table 2, we have presented the distribution of dialysis data and comorbidity of hemodialysis patients and the correlation between QoL and dialysis and comorbidities data.
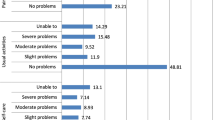
As we introduced before in the methods part, for our hemodialysis patients about the QoL we have created a questionnaire that includes 25 questions classified into five dimensions, which are mobility, personal care, common activities, discomfort and pain, anxiety, and depression. In Table 3, we have presented the mean scores for the five dimensions of QoL that we have used for patients on hemodialysis. The mean of the five domains varies from a minimum value of 1.75 ± 1.06 for personal care to a maximal value of 2.65 ± 1.44 for anxiety and/or depression. The minimum score for each of the domains is 1 and the max score is 5.
About the distribution of the five domains among the hemodialysis patients, we have seen that for mobility most of the patients responded with a score of 2, for personal care, and for common activities or leisure activities most of them responded with a score of 5 respectively, for the pain and discomfort most of them have responded with score 3 and for the anxiety and/or depression most of them have responded with score 5. Figure 1 presents the distribution of health-related quality of life measures in hemodialysis patients.

Distribution of health-related quality of life measures in hemodialysis patients
One of the points at the end of our questionnaire was “How good or bad your health is today”. For this questionnaire, we used a scale numbered from 0 to 100, to evaluate the health status they felt when asked, where the number 100 means the best health they can feel and 0 means the worst health that they can feel. In Fig. 2 we have presented the frequency distribution of “How good or bad your health is today”.

The frequency distribution of “How good or bad your health is today”
Discussion
Nowadays, the quality of life (QOL) research endpoints have emerged as valuable research tools in assessing the outcome of therapeutic intervention in chronic diseases, especially in hemodialysis patients [19, 20]. End-stage renal disease (ESRD) is one such chronic disease causing a high level of disability in different domains of the patients’ lives, leading to impaired QOL [21, 22]. The prevalence of renal replacement therapy in Albania results in 348 cases per million [23], but the information about health-related quality of life (HRQoL) among hemodialysis patients is missing. This is the first study conducted in Albania for QoL among the hemodialysis patients with the aim of evaluating the HRQoL and epidemiological data that affect QoL among the hemodialysis patients.
Based on SF (short form of QoL) the data are presented as mean ± SD. Spearman coefficient was used to evaluate the correlation between the variables. In our sample, represented by a group of 209 hemodialysis patients, the quality of life seems to be correlated with some of the analyzed variables. Many studies showed that older patients over 60 years old had the worst relationship with the QoL [24,25,26,27]. The more years pass the worse they have the appreciation for their quality of life because patients of advanced age usually have bad experiences related to physicals and cognitive impairment or may have lower expectations if we compare them with the younger individuals.
The difference in gender also is seen as a factor that affects the quality of life in patients on hemodialysis [25, 28]. Females have poor QOL as compared to male patients.
Anees et al, in their study, mention that males have better QOL in the social relationship domain as compared to females. The reason for better QOL in males is that males have better social relationships (strong relations and sexual activation) and support than females [29].
In our study, among hemodialysis patients is seen a significant association scored between the quality of life and demographic variables like age groups (p = 0.034), and gender (p = 0.01) as in the previous studies.
Related to other demographic characteristics of hemodialysis patients that affects the QoL, some studies suggested that there is a positive relationship between the level of school education and the QOL [30]. Because a high education means job opportunities and much more monthly income which improves in the same times the financial status and improves QOL in HD patients. Our findings are consistent with other studies [29,30,31,32] because we have found an association between the QoL and education level (p = 0.044); and monthly income (p = 0.017).
Also, residence area, BMI, and alcohol use are found as significant in our study [residence areas (p = 0.002); education level (p = 0.044); BMI (p = 0.001)] like other studies [29, 33, 34].
The presence of comorbidities is an important predictor of mortality because among the hemodialysis patients a reduced QoL is usually associated with cardiovascular disease. Our findings indicated a higher number of comorbidities among hemodialysis patients, same as other studies’ findings [34,35,36]. In this study, the presence of comorbidities was significantly associated with the QOL (p = 0.001). Regarding the origin of renal diseases (p = 0.016); the time of dialysis start (p = 0.04); and frequency of dialysis (p = 0.01) were significantly associated with the overall QOL in hemodialysis patients.
At the end of the questionnaire, we asked all patients: “How good or bad your health is today”.
We used a scale numbered from 0 to 100, to evaluate the health status they felt when asked, where the number 100 means the best health they can feel and 0 means the worst health that they can feel. The average score for our patients resulted to be 47.08 ± 4.5 (mean ± SD). Thirteen patients confirmed that they were in their worst health status and only 5 patients pretended to be in their best health status. Most of the patients that answered this question, declared to feel in status marked from 40 to 80 scale score.
This means that after the dialysis our patients have shown an important improvement in their health status, which is linked to the good feeling of good health.
Conclusion
As we saw from the results of this study, a considerable number of the patients live with low income. Which makes the situation more challenging than usual. Our results have pointed out that different factors like gender, age, residence area, education level, BMI, monthly income, alcohol use, the origin of renal disease, time of dialysis, frequency of dialysis, and presence of comorbidities affect the QOL of HD patients. Regarding the other factors were not evidenced as possible factors for QoL changes in our study. It is necessary to build policies in order to help this category not only economically (provide financial support), but on other aspects also, such as health education, self-care, lifestyle, and focus also on emotional and mental health too. Prevention of severe cases by raising awareness in the population should be the focus of our health system. Therefore, we suggest that future studies include other factors that will evaluate hemodialysis efficiency and find the association between these and QoL. Because the adequate management of some of these factors could influence patient outcomes regarding a better score of QoL. All of this would save human lives and improve the quality of life of patients too.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Karopadi AN, Mason G, Rettore E, Ronco C (2013) Cost of peritoneal dialysis and hemodialysis across the world. Nephrol Dial Transplant 28(10):2553–2569. https://doi.org/10.1093/ndt/gft214
Mushi L, Marschall P, Flessa S (2015) The cost of dialysis in low and middle-income countries: a systematic review. BMC Health Serv Res 15(1):506. https://doi.org/10.1186/s12913-015-1166-8
Murtagh FE, Addington-Hall J, Higginson IJ (2007) The prevalence of symptoms in end-stage renal disease: a systematic review. Adv Chronic Kidney Dis 14(1):82–99. https://doi.org/10.1053/j.ackd.2006.10.001
Levey AS, Coresh J (2012) Chronic kidney disease. Lancet 379(9811):165–180. https://doi.org/10.1016/S0140-6736(11)60178-5
Lozano R, Naghavi M, Foreman K, Lim S et al (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2095–2128. https://doi.org/10.1016/S0140-6736(12)61728-0
Thomas B, Wulf S, Bikbov B, Perico N et al (2015) Maintenance dialysis throughout the world in years 1990 and 2010. J Am Soc Nephrol 26:2621–2633. https://doi.org/10.1681/ASN.2014101017
Liyanage T, Ninomiya T, Jha V, Neal B et al (2015) Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet 385:1975–1982. https://doi.org/10.1016/S0140-6736(14)61601-9
Saran R, Robinson B, Abbott KC, Agodoa LY et al (2017) US renal data system 2016 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis 69:1–2. https://doi.org/10.1053/j.ajkd.2017.01.040
Zyoud SH, Al-Jabi SW, Sweileh WM, Arandi DA et al (2015) Relationship of treatment satisfaction to health-related quality of life among Palestinian patients with type 2 diabetes mellitus: Findings from a cross-sectional study. J Clin Transl Endocrinol 2(2):66–71. https://doi.org/10.1016/j.jcte.2015.03.002
Fukuhara S, Yamazaki S, Hayashino Y, Green J (2007) Measuring health-related quality of life in patients with end-stage renal disease: why and how. Nat Clin Pract Nephrol 3(7):352–353. https://doi.org/10.1038/ncpneph0510
Dashti-Khavidaki S, Sharif Z, Khalili H, Badri S et al (2013) The use of pharmaceutical care to improve health-related quality of life in hemodialysis patients in Iran. Int J Clin Pharm 35(2):260–267. https://doi.org/10.1007/s11096-012-9748-6
Jacobson AM, de Groot M, Samson JA (1994) The evaluation of two measures of quality of life in patients with type I and type II diabetes. Diabetes Care 17(4):267–274. https://doi.org/10.2337/diacare.17.4.267
Sorensen VR, Mathiesen ER, Watt T, Bjorner JB et al (2007) Diabetic patients treated with dialysis: complications and quality of life. Diabetologia 50(11):2254–2262. https://doi.org/10.1007/s00125-007-0810-1
Landman GW, van Hateren KJ, Kleefstra N, Groenier KH, Gans RO, Bilo HJ (2010) Health-related quality of life and mortality in a general and elderly population of patients with type 2 diabetes (ZODIAC-18). Diabetes Care 33(11):2378–2382. https://doi.org/10.2337/dc10-0979
Kleefstra N, Landman GW, Houweling ST, Ubink-Veltmaat LJ et al (2008) Prediction of mortality in type 2 diabetes from health-related quality of life (ZODIAC-4). Diabetes Care 31(5):932–933. https://doi.org/10.2337/dc07-2072
Kalantar-Zadeh K, Kopple JD, Block G, Humphreys MH (2001) Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J Am Soc Nephrol 12(12):2797–2806. https://doi.org/10.1681/ASN.V12122797
Roshan R, Singh R, Menon GR (2014) ICMR-Forte Joint Planning Workshop On Ageing and Health. Workshop Report. From the Division of Non-Communicable Diseases, Indian Council of Medical Research. New Delhi; p. 9. https://cdn5.euraxess.org/sites/default/files/funding/indo-sweden_planning_workshop_report.pdf
World Health Organization Division of Mental Health. (2012) WHOQOL-BREF: introduction, administration, scoring and generic version of the assessment: field trial version, December 1996. https://www.who.int/publications/i/item/WHOQOL-BREF
Testa MA, Simonson DC (1996) Assessment of quality-of-life outcomes. N Engl J Med 334:835–839. https://doi.org/10.1056/NEJM199603283341306
Kaufman SE (2001) The increasing importance of quality of life research. Clin Res 1:18–22
Edgell ET, Coons SJ, Carter WB, Kallich JD et al (1996) A review of health-related quality-of-life measures used in end-stage renal disease. Clin Ther 18:887–938. https://doi.org/10.1016/s0149-2918(96)80049-x
Fox E, Peace K, Neale TJ, Morrison RB, Hatfield PJ, Mellsop G (1991) “Quality of Life” for patients with end-stage renal failure. Ren Fail 13:31–35. https://doi.org/10.1056/NEJM198502283120905
Spasovski G, Rroji M, Vazelov E, Basic Jukic N et al (2019) Nephrology in the Eastern and central European region: challenges and opportunities. Kidney Int 96:287–290. https://doi.org/10.1016/j.kint.2019.02.040
Gerasimoula K, Lefkothea L, Maria L, Victoria A, Paraskevi T, Maria P (2015) Quality of life in hemodialysis patients. Mater Soc 27(5):305–309. https://doi.org/10.5455/msm.2015.27.305-309
Seica A, Segall L, Verzan C, Văduva N et al (2009) Factors affecting the quality of life of hemodialysis patients from Romania: a multicentric study. Nephrol Dial Transplant 24(2):626–629. https://doi.org/10.1093/ndt/gfn506
Bayoumi M, Al Harbi A, Al Suwaida A, Al Ghonaim M, Al Wakeel J, Mishkiry A (2013) Predictors of quality of life in hemodialysis patients. Saudi J Kidney Dis Transpl 24(2):254–259. https://doi.org/10.4103/1319-2442.109566
Mandoorah QM, Shaheen FA, Mandoorah SM, Bawazir SA, Alshohaib SS (2014) Impact of demographic and comorbid conditions on quality of life of hemodialysis patients: a cross-sectional study. Saudi J Kidney Dis Transpl 25(2):432–437. https://doi.org/10.4103/1319-2442.128613
Zyoud SH, Daraghmeh DN, Mezyed DO, Khdeir RL et al (2016) Factors affecting the quality of life in patients on hemodialysis: a cross-sectional study from Palestine. BMC Nephrol 17(1):44. https://doi.org/10.1186/s12882-016-0257-z
Anees M, Malik MR, Abbasi T, Nasir Z, Hussain Y, Ibrahim M (2014) Demographic factors affecting the quality of life of hemodialysis patients – Lahore, Pakistan. Pak J Med Sci 30(5):1123–1127. https://doi.org/10.12669/pjms.305.5239
Coelho-Marques FZ, Wagner MB, Figueiredo CE, Avila DO (2006) Quality of life and sexuality in chronic dialysis female patients. Int J Impot Res 18:539–543. https://doi.org/10.1038/sj.ijir.3901470
Patti F, Pozzilli C, Montanari E, Pappalardo A et al (2007) Italian study group on quality of life in Ms. Effects of education level and employment status on HRQoL in early relapsing-remitting multiple sclerosis. Mult Scler 13(6):783–791. https://doi.org/10.1177/1352458506073511
Ayub N, Iqbal Z (2009) Income-related behavior. Pakistan Business Review
Norozi Firoz M, Shafipour V, Jafari H, Hosseini SH, Yazdani-Charati J (2019) Relationship of hemodialysis shift with sleep quality and depression in hemodialysis patients. Clin Nurs Res 28(3):356–373. https://doi.org/10.1177/1054773817731852
Valderrábano F, Jofre R, López-Gómez JM (2001) Quality of life in end-stage renal disease patients. Am J Kidney Dis 38(3):443–464. https://doi.org/10.1053/ajkd.2001.26824
Lopes AA, Bragg-Gresham JL, Goodkin DA, Fukuhara S et al (2007) Factors associated with health-related quality of life among hemodialysis patients in the DOPPS. Qual Life Res 16(4):545–557. https://doi.org/10.1007/s11136-006-9143-7
Lin Y, Wu P, Kuo M, Lin M et al (2013) High cost and low survival rate in high comorbidity incident elderly hemodialysis patients. PLoS One 8(9):1–8. https://doi.org/10.1371/journal.pone.0075318
Acknowledgements
Firstly, the acknowledgments go to the head of the Dialysis unit in Elbasan City, for his hospitality and assistance in finalizing this paper. I want to acknowledge my co-authors for their support, assistance, and contribution during the preparation of this paper. And finally, but not less importantly, I would like to acknowledge all participating patients willing to provide the required data. Without their help, this work would be difficult to accomplish.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
B. Elezi and E. Abazaj both were involved in the conception and design of the study. E. Elezi and M. Rumano were part of the data collection. E. Elezi, M. Rumano, and E. Abazaj designed the article format and E. Abazaj analyzed the data (statistical analyses) while S. Topi made critical revisions. All researchers drafted the manuscript and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
At the time when the study was conducted in our country, there is not yet one ethics committee that approved the study, but we are allowed to do a study after we are permitted by the head of the institution where the study is carried out. Before the enrollment of all contributors, the researcher explained the purpose of the study. During this study, we followed the guidelines of the Declaration of Helsinki of 1975, as revised in 2008. No personal data were recorded. We warrant that all ethical guidelines for medical research “on the protection of personal data” were strictly respected.
Consent for publication
All authors of this study have given their consent for the publication of this paper.
Competing interests
All the authors played a significant role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the report for publication.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elezi, B., Rumano, M., Abazaj, E. et al. Health-related quality-of-life measures used in hemodialysis patients in Albania. Egypt J Intern Med 35, 3 (2023). https://doi.org/10.1186/s43162-022-00172-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-022-00172-2