
Abstract
Background
Tumor-induced osteomalacia (TIO) is a rare condition with fewer than 500 cases reported in the literature although described. Phosphaturic mesenchymal tumor (PMT) is often unrecognized cause of hypophosphatemia. This case report aims to highlight such a rare association which warrants clinical and radiologist attention.
Case
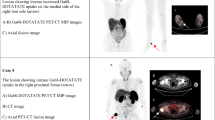
A 51-year-old man had pain in his feet 2 years prior to the most recent presentation in our clinic. The patient experienced increasingly severe body aches and pain, which affected the feet, hips, knees, ribs, waist, and shoulders. MRI and CT led to the diagnosis of multiple insufficiency fractures. Laboratory tests showed that inorganic phosphate (IP) levels had decreased to 0.52 mmol/L(0.81–1.45 mmol/L), while alkaline phosphatase (ALP) had increased to 216 U/L(38.0–126.0 U/L). Positron emission tomography computed tomography showed tumor-derived hypophosphate osteomalacia of the right iliac wing; surgical resection was performed. markers of bone metabolism and bone density returned normal postoperative, after 9 months follow-up.
Conclusion
The possibility of tumor-induced osteomalacia should be considered if unexplained joint pain, decreased bone mineral density, increased ALP and insufficiency fractures, and no similar family history are found in adult patients. Surgical resection of the tumor is the key to the treatment.
Similar content being viewed by others
Background
Phosphaturic mesenchymal tumor (PMT) is an extremely rare pathologic phenomenon that presents as paraneoplastic tumor-induced osteomalacia (TIO) caused by the release of phosphatonins, most notably fibroblast growth factor-23, from the tumor; these hormones decrease proximal renal tubule reabsorption of phosphate and inhibit 1-α-hydroxylase production of 1.25-dihydroxycholecalciferol [1]. TIO is a rare condition with fewer than 500 cases reported in the literature [2]. It was first reported in 1947 by Robert McCance; he described a patient with pain, weakness, gait abnormalities, and low phosphorus levels. The patient was treated with high doses of vitamin D, but the symptoms did not completely resolve until the tumor in the femoral bone was removed [3]. Most clinicians, radiologists, and pathologists are unaware of this rare disease; a small number of cases have been described in the rheumatology literature [1]. Because of poor awareness among clinicians regarding the existence of TIO, combined with the difficulty in locating the instigating tumor after TIO has been recognized as a possible diagnosis, most patients with TIO can have symptoms for up to 5–10 years before a definitive diagnosis is made [4].
Here, we present the case of a 51-year-old man with hypophosphatemic osteomalacia who underwent successful surgical resection of a left acetabulum tumor after 2 years of symptoms. Physicians tend to lack important medical knowledge regarding TIO, mainly because of its early misdiagnosis as gouty arthritis, lumbar degenerative osteoarthropathy, or insufficiency fracture, as well as its atypical clinical manifestations.
Case presentation
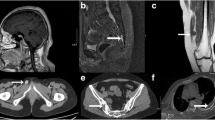
In February 2018, the patient came to our hospital with the complaint of pain between the toes with no obvious cause, as well as impaired mobility and hip discomfort. Laboratory tests showed a uric acid (UA) level of 503 μmol/L (202.3–416.5 μmol/L) and an IP level of 102 mmol/L (0.81–1.45 mmol/L); other laboratory test results were normal. In August 2018, magnetic resonance imaging (MRI) of both feet (i.e., the base of the first metatarsal of the left foot and the proximal segment of the second metatarsal and second metatarsal head of the right foot (Fig. 1-1, 1-2)) led to the diagnosis of insufficiency fractures. After multiple outpatient treatments for gout and foot fasciitis, the patient’s symptoms did not substantially improve. Lumbosacral pain, stiffness, and discomfort gradually appeared; furthermore, the symptoms of bilateral chest muscle pain, breathing difficulty, and coughing were aggravated. The patient was treated for a bulging disc, but his symptoms did not improve. He was hospitalized in April 2019 and diagnosed with gouty arthritis, aseptic necrosis of the left femoral head (Fig. 1-3), and osteopenia (overall lumbar spine T value − 2.0, hip joint T value − 0.8). He received clinical treatments for pain, elevated uric acid level, and osteoporosis. The symptoms improved and he was discharged from the hospital; however, he continued to experience pain in multiple joints. By September 2019, the patient’s clinical symptoms had worsened; thus, he was hospitalized in the Fifth Affiliated Hospital of Sun Yat-sen University (Zhuhai, China) for insufficiency fractures of both the tibial plateau and thoracolumbar spine. Dual-source CT showed gouty arthritis of both feet and laboratory tests showed an alkaline phosphatase (ALP) level of 158 U/L, which led to the diagnosis of myopathy. The patient was treated for his symptoms, then discharged. Beginning in January 2020, the patient experienced pain in multiple joints throughout the body including the feet, hips, knees, ribs, waist, and shoulders; he also experienced poor mobility. Outpatient treatments for dry mouth, dry eyes, rash, and oral ulcers were ineffective. The patient was hospitalized in May 2020 in the orthopedics department. No obvious abnormalities were found in the bilateral femur, tibia and fibula, hip, knee, or ankle joints. Chest CT showed fractures on ribs 1, 2, and 5–7 on the right side (Fig. 1-4); ribs 2 and 3 on the left side; the thoracic spine (T4–5,T9);and the first vertebra of the lumber spine (L1) (Fig. 1-5, 1-6, 1-7, 1-8). Laboratory examination showed that that the IP level had decreased to 0.52 mmol/L, ALP level had increased to 216.4 U/L, osteocalcin (OST) 23.02 μg/L (9.80–26.40 μg/L), type I collagen amino-terminal extension of peptides (TPINP) 113.0 ng/ml (21.6 ng/ml), β-C-terminal telopeptide of type I collagen (β-CTx) 0.69 μg/mL (≤ 0.704 μg/mL) and UA level had increased to 477 μmol/L, parathyroid hormones (PTH) 16.50 pg/ml (15–65 pg/ml). There were no obvious abnormalities in routine blood test, coagulation, erythrocyte sedimentation rate, or thyroid function findings. The stool test findings were normal. Components of bone metabolism were re-evaluated after 7 days of hospitalization: IP had decreased to 0.36 mmol/L and ALP had increased to 205.7 U/L. Multidisciplinary consultation suggested TIO. Positron emission tomography-computed tomography (PET-CT) was performed and revealed presence of the right iliac active nodules. Tumor-derived low phosphorus osteomalacia was considered (Fig. 1-1, 1-2, 1-3).

2018 T1WI, T2WI, proximal second metatarsal linear T1WI, T2WI low signal shadow fracture line (indicated by arrow). 1-3 2018 MRI T1WI left femoral head avascular necrosis. 1-4 CT right third anterior rib fracture in 2020. 1-5–1-8 2020 thoracic spine CT, T1WI, T2WI, STIR image, T4–5, and T9–L1 compression fracture
Preoperative imaging
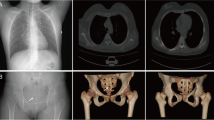
MRI showed an abnormal signal focus on the anteromedial lower right iliac bone; based on the patient’s clinical history, this focus was presumed to be a PMT (Fig. 2-1, 2-2, 2-3). Bone density examination showed that the overall T value of the lumbar spine was − 1.6, while the T value of the hip joint was − 2.6, suggesting osteoporosis of the hip joint. CT showed bone hyperplasia of the right iliac bone, with no obvious abnormalities.

2-1 T2WI pressure-fat in 2019, right iliac bone abnormal signal (arrow). 2-2 and 2-3 2020 T1WI, T2WI pressure-fat with increased iliac bone abnormal signal range. 2-4 2020 normal CT
Preoperative laboratory examination
Laboratory tests showed that ALP increased to 185.3 U/L, while IP increased to 0.54 mmol/L. Routine blood and stool tests showed no obvious abnormalities. Furthermore, there were no obvious abnormalities in coagulation, erythrocyte sedimentation rate, fasting blood glucose, rheumatoid factor, myocardial enzyme, electrolyte, or any other preoperative test results.
Surgical resection of pathology in August 2020
The fragmented bone tissue was subjected to pathology analysis. Tumor cells were visible in the bone trabecula, with diffuse infiltrating growth; this was characterized by abundant uniform oval and short spindle-shaped cells distributed around the blood vessel in a sheet and band. There were no obvious abnormalities in the tumor cells, and nuclear divisions were occasionally observed. The interstitium was rich in blood vessels, some of which were hemangiopericytoma-like blood vessels; bone-like matrix was evident.
Immunohistochemistry results
CD34(rich in blood vessels), SMA(−), Desmin(−), Ki67(1%+), S-100(−), STAT6 cytoplasm +), CK(−), Vimentin(+), CD56(+), CD68(−), NSE(part +), CD99(−), ERG(part +), FLi1(−), D2-40(−), STAB2(+) (Fig. 3-4).

3-1–3-3 Microscopic features of PMT. 3-1 In the bone trabecula, uniform oval and short spindle-shaped tumor cells were found in sheets and bands around blood vessels. 3-2 Some vessels exhibited hemangiopericytoma-like structures. 3-3 The tumor cells had no obvious abnormalities, and nuclear divisions were occasionally observed. The mesenchyme was rich in blood vessels, and local bone-like matrix was evident. 3-4 Immunohistochemical findings in PMT Vimentin (+)
Pathological diagnosis
Consistent with the blood biochemical test results, clinical manifestations, imaging data, and immunohistochemical results, the pathological morphology was suggestive of PMT.
Review in May 2021
Four components of bone metabolism were analyzed: ALP, 102 U/L; osteocalcin, 23.2 μg/L (9.80–26.40 μg/L); calcium (Ca), 2.32 mmol/L (2.10–2.55 mmol/L); and IP, 1.22 mmol/L. Bone density evaluation showed that the overall T value of the lumbar spine was − 0.5, while the T value of the hip joint was − 0.3, indicating normal bone quality.
Diagnosis and treatment process (Table 1)
Follow-up and outcomes
Pathologically, distal-type PMT was diagnosed. There has been no disease recurrence, and no treatment such as chemotherapy or radiotherapy was required, On May 2021, four components of bone metabolism showed normal.
Discussion
Hypophosphatemic osteomalacia is mainly divided into hereditary and acquired types. Acquired hypophosphatemic osteomalacia is divided into drug-induced and neoplastic subtypes; neoplastic hypophosphatemia osteomalacia is a rare paraneoplastic syndrome [5]. Clinical manifestations are unexplained bone pain, muscle weakness, fractures, and bone deformities. Because its early clinical manifestations are non-specific, complex, and diverse, the rates of clinical misdiagnosis and missed diagnosis are high [6]. The most frequent misdiagnoses are intervertebral disc herniation, spondylarthritis (including ankylosing spondylitis), and osteoporosis. Wu N et al. [7] report 43.1% (62/144) of hypophosphatemia cases are overlooked and their diagnoses are missed. Most studies have shown that the excessive secretion of phosphate-regulating factors by tumors, especially fibroblast growth factor-23, acts on the proximal convoluted tubules; this indirectly inhibits phosphate reabsorption by the kidneys. The effects include increased renal phosphorus excretion, high urinary phosphorus, and a low level of phosphate in the blood, leading to acquired hypophosphatemia osteomalacia; conventional phosphorus supplementation is ineffective [2, 8]. These clinical signs are caused by PMTs of the soft tissue and bone, which are usually benign. Recently, malignant neoplasms such as small cell lung carcinoma [9], colon adenocarcinoma [10], prostate adenocarcinoma [11], renal cell carcinoma [12], and multiple myeloma [13] have been associated with acquired hypophosphatemia osteomalacia [14].
After a diagnosis of TIO is established, it is crucial to locate the PMT, because surgical excision of the tumor is the only definitive curative treatment. Because the tumor is small and indolent, affected patients’ medical histories and physical examinations seldom reveal a lump or bump. Additionally, approximately 2% of patients may have multifocal disease at initial presentation [2].
Imaging is important for tumor localization. Tumors are usually small, especially in distal extremities, and can easily be missed by CT or MRI [15]. The morphological features of PMTs are usually similar to other more common bone or soft tissue tumors. Using conventional CT and MRI, it is difficult to distinguish whether a tumor has secretory function [16]. Some clinicians have recommended molecular imaging as an initial imaging tool for the detection and localization of TIO. TIO pathogenic tumors mostly originate from mesenchymal tissues and express somatostatin receptors. Somatostatin receptor imaging has become an important means to explore TIO pathogenic tumors. Relevant imaging agents include 111In-octreotide, 99Tcm-hydrazinonicotinamide-Tyr3-OC, and68Ga-labelled somatostatin analogues. Ga-68 DOTATATE, used during PET-CT, has high diagnostic sensitivity of 92.6–98.1% [1, 2, 4, 9, 17]. Selective somatostatin receptor imaging with Ga-68 DOTATATE PET-CT has been established as a preferred primary imaging modality [18].
Currently, there are no guidelines for the treatment of TIO. For this disease, most clinicians focus on treating the cause; generally, patients can be cured after complete removal of the tumor [1, 19]. Tumor recurrence occurs in fewer than 5% of patients with TIO [6, 20]. The lung is a common site of metastasis. The course after metastasis is variable, and survival of up to 30 years has been reported [20].
This case demonstrates the typical chronological progression of TIO, in which the diagnosis and tumor localization are challenging for clinicians and radiologists. Our patient initially experienced pain between the toes and received treatment for gouty arthritis, which provided some symptomatic improvement. His laboratory test results were normal, which increased the risk of missed diagnosis. Then, progressive bone and joint pain, substantial muscle weakness, hyperuricemia, and atypical inflammatory back pain occurred. Inflammation indicators were normal. Osteoporosis, multiple insufficiency fractures, and subsequent treatments of gouty arthritis and osteoporosis were ineffective, suggesting the presence of metabolic bone disease. Further screening for markers of bone metabolism: ALP level had increased to 216.4 U/L and TPINP level had increased to 113.0 ng/ml, OST and β-CTx level were normal. Additional analyses were conducted to identify the cause of hypophosphatemia. The patient had no familial medical history suggestive of a genetic aetiology; he also had no distinctive medication history. Fanconi syndrome caused by systemic diseases (e.g., amyloidosis or Sjogren’s syndrome) was excluded, the patient’s blood sugar and blood routine test levels were normal. Notably, conventional CT and MRI easily missed the diagnosis in this patient. After the tumor had been removed. Oral calcium supplementation, calcitriol capsules, and traditional Chinese medicine in the treatment of osteoporosis and phosphorus supplementation were administered. The patient’s symptoms of bone pain and muscle weakness were substantially relieved, and ALP, calcium, and bone density returned to normal. Thus, the patient’s osteomalacia-related hypophosphatemia had been caused by the tumor.
Conclusion
Tumor-induced osteomalacia (TIO) is a rare disease. The early clinical manifestations are non-specific, and routine laboratory examinations show no characteristic indicators; these are the main reasons for misdiagnosis in patients with TIO. When a patient has unidentified limb joint pain, low back pain, and muscle weakness, clinicians should consider laboratory assessments of bone metabolism abnormalities, imaging examinations to identify osteoporosis and insufficiency fractures, and a detailed physical examination to exclude primary and drug-induced causes. Adequate tumor screening, especially PET-CT examination of soft tissue and bone tumors to facilitate early diagnosis and early surgical resection, is important for osteomalacia prognosis. In addition, timely pathological examination can effectively prevent or reduce misdiagnosis.
Availability of data and materials
Some or all data, models, or code generated or used during the study are available from the corresponding author by request (MQ Xiao, Email: xmqzhuhai@163.com).
Abbreviations
- PMT:
-
Phosphaturic mesenchymal tumor
- TIO:
-
Tumor-induced osteomalacia
- MRI:
-
Magnetic resonance imaging
- CT:
-
Computed tomography
- ALP:
-
Alkaline phosphatase
- PET-CT:
-
Positron emission tomography–computed tomography
- UA:
-
Uric acid
- OST:
-
Osteocalcin
- TPINP:
-
Type I collagen amino-terminal extension of peptides
- β-CTx:
-
β-C-terminal telopeptide of type I collagen
- IP:
-
Inorganic phosphate
- PTH:
-
Parathyroid hormones
References
Dadoniene J, Miglinas M, Miltiniene D, Vajauskas D, Seinin D et al (2016) Tumour-induced osteomalacia: a literature review and a case report. World J Surg Oncol 14(1):4. https://doi.org/10.1186/s12957-015-0763-7
Richardson AL, Richardson OK (2019) Phosphaturic mesenchymal tumor: Case report. Radiol Case Rep 14(12):1518–1524. https://doi.org/10.1016/j.radcr.2019.09.027
Mc CR (1947) Osteomalacia with Looser's nodes (Milkman’s syndrome) due to a raised resistance to vitamin D acquired about the age of 15 years. Q J Med 16(1):33–46
Kumar S, Diamond T (2020) Lessons learnt from delayed diagnosis of FGF-23-producing tumour-induced osteomalacia and post-operative hungry bone syndrome. Bone Rep 12:100276. https://doi.org/10.1016/j.bonr.2020.100276
Folpe AL, Fanburg-Smith JC, Billings SD, Bisceglia M, Bertoni F et al (2004) Most osteomalacia-associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. Am J Surg Pathol 28(1):1–30. https://doi.org/10.1097/00000478-200401000-00001
Feng J, Jiang Y, Wang O, Li M, Xing X et al (2017) The diagnostic dilemma of tumor induced osteomalacia: a retrospective analysis of 144 cases. Endocr J 64(7):675–683. https://doi.org/10.1507/endocrj.EJ16-0587
Wu N, Zhang Z, Zhou X, Zhao H, Ming Y et al (2020) Mutational landscape and genetic signatures of cell-free DNA in tumour-induced osteomalacia. J Cell Mol Med 24(9):4931–4943. https://doi.org/10.1111/jcmm.14991
Obo T, Koriyama N, Tokito A, Ogiso K, Nishio Y (2020) Neurofibromatosis type 1 associated with hypophosphatemic osteomalacia due to hypersecretion of fibroblast growth factor 23: a case report. J Med Case Rep 14(1):56. https://doi.org/10.1186/s13256-020-02381-1
Tantisattamo E, Ng RC (2011) Dual paraneoplastic syndromes: small cell lung carcinoma-related oncogenic osteomalacia, and syndrome of inappropriate antidiuretic hormone secretion: report of a case and review of the literature. Hawaii Med J 70(7):139–143
Leaf DE, Pereira RC, Bazari H, Juppner H (2013) Oncogenic osteomalacia due to FGF23-expressing colon adenocarcinoma. J Clin Endocrinol Metab 98(3):887–891. https://doi.org/10.1210/jc.2012-3473
Mak MP, da Costa e Silva VT, Martin RM, Lerario AM, Yu L et al (2012) Advanced prostate cancer as a cause of oncogenic osteomalacia: an underdiagnosed condition. Support Care Cancer 20(9):2195–2197. https://doi.org/10.1007/s00520-012-1474-z
Xie Y, Li HZ (2013) Oncogenic osteomalacia caused by renal cell carcinoma. J Clin Endocrinol Metab 98(12):4597–4598. https://doi.org/10.1210/jc.2013-3335
Reyskens M, Sleurs K, Verresen L, Janssen M, van den Bergh J et al (2015) Hypophosphatemic osteomalacia: an unusual clinical presentation of multiple myeloma. Osteoporos Int 26(7):2039–2042. https://doi.org/10.1007/s00198-015-3090-5
Pal R, Agrawal K, Gupta S, Bhansali A, Behera A et al (2020) Worsening of unrecognized tumour-induced osteomalacia with inadvertent use of recombinant human parathyroid hormone. Endokrynol Pol 71(1):102–103. https://doi.org/10.5603/EP.a2019.0045
Singh D, Chopra A, Ravina M, Kongara S, Bhatia E et al (2017) Correction to Oncogenic osteomalacia: role of Ga-68 DOTANOC PET/CT scan in identifying the culprit lesion and its management. Br J Radiol 90(1079):20160811e. https://doi.org/10.1259/bjr.20160811.e
Li B, Dong Y, Liu D, Yao Q, Guo S et al (2020) Left maxillary sinus tumour-induced hypophosphataemic osteomalacia and combined with thyroid papillary carcinoma: a case report and literature review. Intern Med J 50(6):755–761. https://doi.org/10.1111/imj.14864
Zhou Z, Yue H, Xu J, Xu X, Guo Q et al (2018) A case with tumour-induced osteomalacia misdiagnosed as axial spondyloarthritis. Rheumatology (Oxford) 57(12):2242–2243. https://doi.org/10.1093/rheumatology/key255
Bhavani N, Reena Asirvatham A, Kallur K, Menon AS, Pavithran PV et al (2016) Utility of Gallium-68 DOTANOC PET/CT in the localization of Tumour-induced osteomalacia. Clin Endocrinol (Oxf) 84(1):134–140. https://doi.org/10.1111/cen.12822
Minisola S, Peacock M, Fukumoto S, Cipriani C, Pepe J et al (2017) Tumour-induced osteomalacia. Nat Rev Dis Primers 3:17044. https://doi.org/10.1038/nrdp.2017.44
Khosravi A, Cutler CM, Kelly MH, Chang R, Royal RE et al (2007) Determination of the elimination half-life of fibroblast growth factor-23. J Clin Endocrinol Metab 92(6):2374–2377. https://doi.org/10.1210/jc.2006-2865
Acknowledgements
We greatly appreciate the assistance of the staff in the Department of Hepatobiliary Surgery and Pathology at Zhuhai Hospital of Guangdong Hospital of Traditional Chinese Medicine for their help and efforts.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
PK Huang was involved in drafting the manuscript. M Zhang, JZ Ye, and JH Tang were involved in acquisition of data and preparing the figures. MQ Xiao designed the manuscript. MQ Xiao and J Chen were involved in analysis and interpretation of data. PK Huang and MQ Xiao were involved in review and revised the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of Guangdong Hospital of Traditional Chinese Medicine.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, P., Xiao, M., Zhang, M. et al. Diagnosis and surgical treatment of tumor-induced osteomalacia—a literature review and a case report. Egypt J Intern Med 34, 14 (2022). https://doi.org/10.1186/s43162-022-00101-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-022-00101-3