
Abstract
Background
Failed extubation increases the intensive care unit (ICU) length of stay, hospital length of stay, and financial costs and it reduces the patient’s functional ability. Avoiding failed extubation is of utmost importance, therefore predictors for successful extubation are paramount.
Objective
To determine if successful extubation in mechanically ventilated patients can be predicted by physiotherapists using upper limb muscle strength and exercise endurance.
Methods
Fifty-seven patients from the medical and trauma ICUs of a large academic hospital were eligible for testing. Muscle strength was evaluated using the Oxford grading scale, Medical Research Council score (MRC score), handgrip dynamometer, and maximum inspiratory pressure (MIP). Exercise endurance was tested while the patient was actively riding the MOTOmed® letto2 cycle ergometer for six minutes with the upper limbs.
Results
Exercise endurance (time the patient rode actively) (P = 0.005), MRC-score (P = 0.007), and number of days ventilated (P = 0.005) were associated with successful extubation. The handgrip strength (P = 0.061), MIP (P = 0.095), and muscle strength of the sternocleidomastoid (P = 0.053) and trapezius muscles (P = 0.075) were marginally associated with successful extubation. Due to multicollinearity when developing the prediction equation, the final multivariable logistic regression prediction model included only exercise endurance and the number of days ventilated. The newly developed prediction equation conferred a sensitivity of 81.82% and a specificity of 77.14% to predict successful extubation.
Conclusion
Successful extubation of mechanically ventilated patients can be predicted by physiotherapists using the newly developed prediction equation consisting of exercise endurance and number of days ventilated.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Since the inception of mechanical ventilators, successful weaning and extubation failure have always been a challenge that physiotherapists, nurses, and physicians grapple with [1]. Early liberation from the ventilator is beneficial to patients, yet premature discontinuation of mechanical ventilation can compromise gas exchange and lead to re-intubation [2]. Failed extubation is associated with an increase in intensive care unit (ICU) length of stay, hospital length of stay, increased cost, and an increase in mortality rate [3]. It can be due to congestive cardiac failure, upper airway obstruction, neurological impairment, an ineffective cough with airway secretions, or respiratory failure [1, 4]. Respiratory failure usually occurs when the load on the diaphragm and accessory respiratory muscles (trapezius, sternocleidomastoid, scalene, and pectoralis major muscles) exceed their capacity [5].
A physiotherapist plays an important role in managing the patient’s respiratory system as well as the musculoskeletal system in the ICU. It is thus vital that physiotherapists are actively involved in the decision to extubate [6]. Physiotherapy-driven weaning protocols are safe and decrease the weaning time [7, 8].
Several studies have been performed to evaluate successful extubation predictors, but none can be used with absolute certainty or in isolation [1,2,3, 6, 9,10,11]. Parameters reflecting cardiovascular and respiratory function such as the fluid balance, pneumonia, amount of secretions, respiratory rate, heart rate variability, tidal volume, rapid shallow breathing index (RSBI), cough strength, partial pressure of arterial oxygen to fraction of inspired oxygen ratio (PaO2/FiO2 ratio), maximum inspiratory pressure (MIP), maximum expiratory pressure, diaphragmatic dysfunction and handgrip strength have been explored [1,2,3, 10,11,12,13,14,15]. None of these factors included exercise endurance. A study conducted by De Jonghe et al. [12] indicated that respiratory muscle weakness is associated with peripheral muscle weakness. Toosizadeh et al. [13] on the other hand concluded that upper extremity strength is associated with pulmonary function and exercise endurance tested with the 6-min walking test. A pilot study by De Beer et al. [14] demonstrated that the muscle strength of the deltoid, sternocleidomastoid, and trapezius muscles measured with the Oxford grading scale may possibly be associated with successful extubation. During the same study exercise endurance tested with the MOTOmed® letto2 cycle ergometer indicated a trend of possible association with successful extubation [14].
The possible associations between respiratory muscle strength, peripheral muscle strength, exercise endurance, and successful extubation raise the question of whether successful extubation can be predicted using upper limb muscle strength and exercise endurance as predictors [12,13,14]. The aim of this study was to determine if upper limb muscle strength and exercise endurance can predict successful extubation using a prediction equation.
Methods
Study design and population
A predictive correlational study was conducted for eighteen months at an Academic Hospital in Pretoria, South Africa. Ethical approval was obtained from the Research Ethics Committee, Faculty of Health Sciences, University of Pretoria (number 394/2017). Patients were recruited from the Surgery/Trauma and Medical ICUs.
All patients who were considered for extubation for the first time by the healthcare team according to the unit protocol (Table 1), were evaluated daily to determine if they complied with the inclusion criteria for the study. Inclusion criteria were age 18 years and older, mechanically ventilated for three and more days, understanding Afrikaans and/or English, awake and cooperative with Richmond Agitation-Sedation Scale (RASS) “ − 1, 0, 1” and 3/5 for the 5-point questionnaire. Hemodynamic stability with a heart rate ≤ 140b/min, systolic blood pressure ≥ 90 mmHg, hemoglobin ≥ 7 g/dl−1, and a temperature < 38.5 °C. Minimal mechanical ventilator settings of continuous positive pressure ventilation, positive end-expiratory pressure (PEEP) ≤ 8 cmH2O, FiO2 ≤ 40%, SpO2 ≥ 90%, and pH ≥ 7.35 were required. In addition, a good cough reflex to tracheal suctioning and minimal to moderate secretions (patients only suctioned four hourly according to unit protocol) were stipulated. The exclusion criteria were: patients with “do not resuscitate” status, upper airway obstruction, body mass index > 35 kg/m2, cardiomyopathy, atrial fibrillation, primary/previously diagnosed neuromuscular disorder, psychiatric disorder, severe agitation (RASS ≥ + 2) or an acute asthma attack. Patients who were not able to perform manual muscle testing techniques due to a spinal cord injury, bilateral amputations, bilateral fractures, soft tissue injuries, burns, or dressings limiting the testing of the muscle strength were also excluded.
All patients recruited in the study received usual physiotherapy treatment. The treatment included chest physiotherapy and rehabilitation (mobilization and active or passive upper limb and lower limb exercises). All patients included in the study gave informed consent.
Study procedures
The demographic and clinical characteristic information, muscle strength, exercise endurance, and MIP data were collected by the principal researcher. Patients considered for extubation were evaluated daily for awareness and orientation by using the RASS [15] and a 5-point questionnaire [12]. The RSBI, electrolytes, and PaO2/FiO2 ratio were documented before muscle strength testing was commenced. The Medical Research Council score (MRC score) was used to evaluate the patient’s general muscle strength. The muscle strength of the deltoid, sternocleidomastoid, trapezius, and pectoralis major muscles was evaluated with the Oxford grading scale. Muscle testing started within the position of a grade 3 muscle and then adapted according to the patient’s ability to include or illuminate the influence of gravity [16, 17].
After completing the muscle strength testing, the patients were positioned in an upright position in bed with arms by side and elbows 90° flexed to test the handgrip strength with the handgrip dynamometer. The forearm was allowed to rest on the thigh. For all patients, the maximum contraction was determined as the highest of the three contractions. The dynamometer handle was in the second position as described by published recommendations from the American Society of Hand Therapists [18]. One-minute rest periods were present between contractions. The dominant and non-dominant hands were tested. The handgrip dynamometer and cycle ergometer were automatically calibrated before each test.
After the handgrip assessment, exercise endurance was tested with the MOTOmed® letto2 cycle ergometer. Patients were positioned in the semi-Fowler’s position in bed with their upper limbs placed in the forearm shells with arm cuffs. Patients rode the cycle ergometer for six minutes with the upper limbs against a resistance of one gear (1 gear = 0.85 kg) while using the Servo Cycle program [19]. The time and distance the patient rode actively (pushing the pedals themselves) as well as passively (machine is moving the pedals) were documented.
Patients remained in the semi-fowler’s position in bed for the MIP measurements. The manometer was connected to the endotracheal tube/tracheostomy. The best measurement out of three was used in the study. Patients rested for a minimum of five minutes or until their heart rate and oxygen saturation were back to baseline between positional changes (sitting to supine) and the different tests. Patients also had to respond to the qualitative question whether they were comfortable or not, before any test was commenced. Testing was discontinued immediately when a patient developed any sign of hemodynamic instability (any changes of 20% of the baseline heart rate, blood pressure, or oxygen saturation) [9, 20] or if the heart rate, blood pressure, or oxygen saturation did not return to baseline after 5 min.
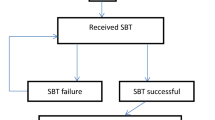
All patients started with the extubation process 30 min after completion of the muscle strength and endurance tests. Patients are evaluated at 48 h and 72 h post-extubation in order to determine whether the patient was successfully extubated. The research process is demonstrated in Fig. 1.

Research process
Statistical analysis
The statistical objective of this study was to develop a prediction equation based on upper limb muscle strength (deltoid, sternocleidomastoid, trapezius, and pectoralis major muscles) and exercise endurance (distance rode actively) for the outcome of extubation. Continuous data was summarised using mean, standard deviation, median, interquartile range, and 95% confidence intervals. For discrete parameters frequency, percentage, cross-tabulation, and 95% confidence intervals were reported. Univariable analyses were done to assess the association of the observed factors with extubation outcomes. For continuous data use, Student’s two-sample t-test while for discrete data Pearson’s chi-square test and univariable logistic regression were employed. The purpose of the univariable analysis was to identify possible factors (marginal significant and significant factors) for inclusion in a multivariable logistic regression analysis to develop the prediction equation. In the modeling process factors which were no longer significant in the multivariable model dropped out, multicollinearity among factors was also responsible for dropout. The predictive ability of the prediction equation was assessed in a cross-validation. Testing was based on a 0.05 level of significance. P ≤ 0.05 was regarded as statistically significant, 0.05 < P ≤ 0.1 was marginally significant and P > 0.1 was not significant. Data analysis employed STATA version 15.1 software [21]. The outcome of extubation was referred to and divided into successful extubation and failed extubation.
Results
A total of 463 patients were recruited but only 57 patients were eligible for inclusion data analysis (Fig. 1). All the included patients completed the assessment. No adverse events were reported. Table 2 outlines the demographic data of the 57 patients. Seven female (30.4%) and 15 male (44.1%) participants failed extubation. Gender and age were not statistically significantly associated with successful extubation. The diagnosis of the patients included medical (asthma, congestive cardiac failure, renal failure, organophosphate poisoning), and surgery (abdominal surgery, poly-trauma, vascular surgery, orthopedic surgery, urology, gynecology) conditions.
Successfully extubated patients had a marginally significant greater proportion of grade 3 muscle strength of sternocleidomastoid (P = 0.058: 71.4% vs 45,5%) and trapezius (P = 0.095: 94.3% vs 77.3%) muscles than failed extubated subjects. The muscle strength of the deltoid (P = 0.366) and pectoralis major (P = 0.417) muscles were not significantly associated with successful extubation. Logistic regression analysis for the upper limb muscle strength in Table 3 reflected that the sternocleidomastoid and trapezius muscles were marginally significantly associated with successful extubation.
The mean body muscle strength, tested with the MRC score, was significantly greater in the successfully extubated group (Table 4). A one-point increase in the MRC score was associated with a (7%) reduction in the risk of failing extubation. The extubation groups were marginally significantly different with regards to the mean handgrip strength measured with the handgrip dynamometer and respiratory muscle strength measured with the MIP respectively.
Successfully extubated patients rode the cycle ergometer significantly longer by themselves (actively) than the failed extubated subjects (Table 4). The logistic regression analysis in Table 3 indicates that for every 15 s that the subject rode actively on the cycle ergometer with the upper limbs, their relative risk of failing extubation decreased by 5%. Post-testing the successfully extubated patients did not differ significantly from the failed extubated subjects with respect to mean heart rate (% of maximum heart rate) (P = 0.125: 54.8% vs 59.4%). The resting heart rate was marginally associated with successful extubation whereas the systolic and diastolic blood pressure measurements were not significantly associated with successful extubation (Table 4). The continuous data in Table 4 showed that the RSBI is significantly associated with successful extubation but the PaO2/FiO2 ratio and RASS were only marginally significantly associated with successful extubation. Successfully extubated patients were ventilated for shorter times. Every day a patient was ventilated, the higher the relative risk (RR = 1.242) was to fail extubation.
To develop a prediction equation for predicting successful extubation a multivariable logistic regression was employed. The sternocleidomastoid muscle strength, MRC score, exercise endurance (time rode actively on the cycle ergometer), number of days ventilated, and RSBI were included as significant exposure factors. Factors were considered at the liberal 0.10 level of significance. The MRC score and exercise endurance were strongly correlated (r = 0.7247; P < 0.001) and the linear relationship was found as MRC-score = 26.97 + 0.062 × exercise endurance (active time rode). The MRC-score and handgrip strength also correlated (r = 0.5323; P < 0.001) and the linear relationship was found as MRC-score = 32.01 + 0.610 × handgrip strength. The handgrip strength and exercise endurance correlated (r = 0.5276; P < 0.001) with a lower correlation coefficient than the MRC-score and exercise endurance.
Due to the multicollinearity, the final multivariable logistic regression prediction model included only the exercise endurance (active time the patient was riding in 15-s units) and the number of days ventilated (Table 5) as the other factors did not add to the predictive value of the model. This model conferred a sensitivity of 81.82% and a specificity of 77.14% for a 0.43 cut-off in the probability of a poor extubation outcome.
The predictive ability of the newly developed tool was assessed using cross-validation for the latter best equation, based on the number of days ventilated and exercise endurance respectively. The calculations demonstrated that if the equation, ŷ = − 1.0064–(0.17 × active time) + (0.230 × ventilator days), is used and the value for ŷ is less than or equal to − 0.282, the model has a sensitivity of 81.8% (Table 6) to predict successful extubation.
The electrolyte data was documented as part of the clinical data. All the values for the electrolytes were within normal limits and did not influence the extubation outcome.
Discussion
Successfully predicting extubation is difficult as it is confounded by many factors. We have observed that successful extubation in critically ill mechanically ventilated patients may be predicted based on exercise endurance and duration of ventilation.
We measured exercise endurance according to the time the patient rode the MOTOmed® letto2 cycle ergometer actively with the upper limbs. Using the upper limb cycle ergometer for six minutes is aligned with both Hol et al. [22] and Bulthuis et al. [23] who recommend the 6-min arm test (6-MAT) with a cycle ergometer to determine exercise endurance. Hol et al. [22] used the 6-MAT on spinal cord injured patients whereas Bulthuis et al. [23] used it among 30 healthy volunteers. To our knowledge, our study is the first that has included more than 30 patients when evaluating exercise endurance with an arm ergometer in the ICU setting. The training intensity of our patients was 54% of the patients’ maximum heart rate. This is in accordance with Swain et al. [24] and the American College of Sports Medicine (cited Swain et al.) who suggest that a 70 to 30% heart rate reserve is required to produce an exercise training effect and result in improved aerobic capacity in unfit people. Evaluating exercise endurance can be challenging when not performed in a laboratory where the VO2 max can confirm a change in the training intensity and aerobic capacity. Exercise endurance indicates whether a patient has sufficient maximal oxygen uptake to perform an activity. Riding the cycle ergometer with the upper limbs causes a higher oxygen uptake, heart rate, and pulmonary ventilation than riding with the lower limbs [24]. According to Mitropoulos et al. [25] there is an increase in anaerobic metabolism, greater carbohydrate oxidation, lactate release, and lower oxygen extraction capacity in the arms than in the legs. An increase in the cardiac output during exercise increases oxygen uptake by the working muscles as well as increases blood flow to the lungs [26]. Transitioning to spontaneous breathing after extubation increases the work of breathing and myocardial oxygen consumption [27, 28]. Evaluating exercise endurance should therefore assist the physiotherapist in determining their cardiorespiratory reserve to tolerate spontaneous breathing.
Our successfully extubated patients demonstrated a greater proportion of grade 3 sternocleidomastoid and trapezius muscle strength than patients who failed extubation. The sternocleidomastoid and trapezius muscle are important when the ventilator demands increase [29]. When their muscle strength increases, the diaphragm functions better. Critically ill patients often fixate their neck/cervical spine which can lead to contraction of the trapezius and sternocleidomastoid muscles. The sternocleidomastoid and trapezius muscles might therefore have a grade 3 muscle strength and could explain why there are some associations with successful extubation.
The deltoid muscle is responsible for shoulder abduction whilst the pectoralis major muscles can contract during forced expiratory tasks [29]. Vivier et al. [30] showed that pectoral muscle atrophy was associated with prolonged weaning from mechanical ventilation. During mechanical ventilation, the work of breathing is decreased due to pressure support given by the ventilator. The decrease in the negative pressure also causes a reduction in the cough strength [30]. The correlation between the electromyographic activity of the pectoralis major muscle and the peak expiratory flow, the decreased work of breathing, and the weak cough might indicate that the pectoralis major muscle function is also decreased. We recommend that future studies explore the correlation between pectoralis major muscle strength and cough strength. The deltoid and pectoralis major muscles consist mainly of fast-twitch muscle fibres and their inactivity might lead to muscle atrophy occurring explaining why they are not associated with successful extubation. A decrease in pectoralis major muscle strength did not influence our patients while riding the cycle ergometer. As outlined by Mitropoulos et al. [25] this might be because during arm cycle ergometry the primary working muscles are the biceps and triceps brachii muscles.
Patients with a higher MRC score were more likely to be successfully extubated. Similarly, Dres et al. [31] found that failed extubation was associated with significantly lower MRC scores and that the MRC score is not independently associated with weaning failure. Although our results demonstrated that the MRC-score was associated with extubation failure, our final multivariable logistic regression prediction model also did not merit its inclusion. In view of the correlation between the MRC score, handgrip strength and exercise endurance there was multicollinearity when developing the prediction equation, hence the inclusion of exercise endurance only. Our correlation between the MRC score and handgrip strength has been previously described by Yosef-Brauner et al. [32].
Unlike our marginal association, Cottereau et al. [33] found no association between handgrip strength and extubation outcome. They explain that the handgrip strength evaluation does represent patients with predominant proximal muscle weakness and not distal hand weakness [33]. Interestingly, Efstathiou et al. [34] demonstrated a strong correlation between MIP and handgrip strength. These differences in findings, maybe due to sample size variations. Cottereau et al. [33] evaluated 84 patients whereas our study and Efstathiou et al. [34] evaluated 57 and 24 subjects respectively. As such we recommend that future research explore factors such as hand dominancy or oedema that might influence handgrip strength or its assessment.
Our observation that successful extubation was associated with RSBI and MIP (only marginally) contrasts with others [35, 36] where MIP has demonstrated greater predictive precision than RSBI. Including the RSBI in the multivariable logistic prediction model in our model conferred a sensitivity of 86.36% and specificity of 80%. However after cross-validation, the predictive model (RSBI, exercise endurance, and number of days ventilated) exhibited a sensitivity of 68.2% and specificity of 74.3%, and thus RSBI was excluded. RSBI is the most studied parameter and RSBI < 105 b/min is a good predictor for weaning, but not when used in isolation [37]. Variable results regarding MIP and RSBI as predictors may be due to the MIP being difficult for patients to perform, whilst the RSBI is a computation. For critically ill patients, the MIP test may not be practical to implement and interpret.
Our findings that the number of days ventilated is associated with successful extubation have also been described by Thille et al. [38] and Baptistella et al. [37] who observed that the longer the patients are ventilated, the higher the risk for extubation failure.
Currently utilized predictors focus mainly on respiratory factors. Our model adds to this by considering the functionality of the respiratory, cardiovascular, and musculoskeletal systems which are inextricably linked to achieving successful extubation [39]. We thus argue that our model would be very useful as an additional tool to inform the decision process for extubation.
Limitations
As a single center study conducted in medical and general surgical patients, this limits the findings to this subset of critically ill patients. Further, participants were exposed to the handgrip dynamometer or cycle ergometer for the first time during the course of the study.
Recommendations
We recommend that our prediction model be externally validated in medical and surgical ICU settings. We also recommend exploration of the association between cough strength and successful extubation as well as the association between MIP and upper limb muscle strength.
Conclusion
This study has demonstrated that successful extubation of mechanically ventilated patients may be predicted by using the newly developed prediction equation which incorporates exercise endurance and number of days ventilated. This tool adds to the array of available methods to assist the multidisciplinary healthcare team in determining readiness for extubation. This is the first study that combines cardio-respiratory and muscle function to evaluate extubation success. Essentially we conclude that as the number of days the patient is ventilated increases and the exercise endurance reduces the risk of failing extubation increases. Taking into account the benefits of successful extubating, the findings of this study have the potential to impact positively on patient outcomes.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ICU:
-
Intensive care unit
- ICU-AW:
-
Intensive care unit acquired weakness
- MRC-score:
-
Medical Research Council score
- MIP:
-
Maximum inspiratory pressure
- PaO2/FiO2 ratio:
-
Partial pressure of arterial oxygen to fraction of inspired oxygen ratio
- PEEP:
-
Positive end-expiratory pressure
- RSBI:
-
Rapid shallow breathing index
- RASS:
-
Richmond Agitation Sedation Scale
References
Torrini F, Gendreau S, Morel J, Carteaux G, Thille AW, Antonelli M, et al. Predication of extubation outcome in critically ill patients: a systematic review and meta-analysis. Crit Care. 2021;25:391.
Baptistella A, Mantelli L, Matte L, Carvalho ME, Fortunatti JA, Costa IZ, et al. Prediction of extubation outcome in mechanically ventilated patients: development and validation of the extubation predictive score. PLoS One. 2021;16(3):e0248868.
Zein H, Baratloo A, Negida A, Safari S. Ventilator weaning and spontaneous breathing trials; an educational review. Emergency. 2016;4(2):65–71.
Díaz MC, Ospina-Tascón GA, Salazar BC. Respiratory muscle dysfunction: a multicausal entity in the critically ill patient undergoing mechanical ventilation. Arch Bronconeumol. 2014;50(2):73–7.
Martin AD, Smith BK, Davenport PD, Harman E, Gonzalez-Rothi RJ, Baz M, et al. Inspiratory muscle strength training improves weaning outcome in failure to wean patients: a randomized trial. Crit Care. 2011;15(2):R84.
Cork G, Camporota L, Osman L, Shannon H. Physiotherapist prediction of extubation outcome in the adult intensive care unit. Physiother Res Int. 2019;24(4):e1793. https://doi.org/10.1002/pri.1793.
Taniguchi C, Victor ES, Pieri T, Henn R, Santana C, Giovanetti E, et al. Smart Care™ versus respiratory physiotherapy-driven manual weaning for critically ill adult patients: a randomised controlled trial. Crit Care. 2015;19:246. https://doi.org/10.1186/s13054-015-0978-6.
Plani N, Becker P, Van Aswegen H. The use of a weaning and extubation protocol to facilitate effective weaning and extubation from mechanical ventilation in patients suffering from traumatic injuries: a non-randomized experimental trial comparing a prospective to retrospective cohort. Physiother Theory Pract. 2013;29(3):211–21. https://doi.org/10.3109/09593985.2012.718410.
Liu Y, Mu Y, Li G, Yu X, Li P, Shen Z, et al. Extubation outcome after a successful spontaneous breathing trial: a multicentre validation of a 3-factor prediction model. Exp Ther Med. 2015;10(4):1591–601. https://doi.org/10.3892/etm.2015.2678.
Dos Santos BU, Souza GF, Campos ES, De Carvalho EF, Fernandes MG, Santoro I, et al. Maximum inspiratory pressure and rapid shallow breathing index as predictors of successful ventilator weaning. J Phys Ther Sci. 2015;27:3723–7.
Huang C-T, Yu C-J. Conventional weaning parameters do not predict extubation outcome in intubated subjects requiring prolonged mechanical ventilation. Respir Care. 2013;58(8):1307–14. https://doi.org/10.4187/respcare.01773.
De Jonghe B, Bastuji-Garin S, Durand MC, Malissin I, Rodrigues P, Cerf C, et al. Respiratory weakness is associated with limb weakness and delayed weaning in critical illness. Crit Care Med. 2007;35(9):2007–15.
Toosizadeh N, Berry C, Bime C, Najafi B, Kraft M, Mohler J. Assessing upper-extremity motion: an innovative method to quantify functional capacity in patients with chronic obstructive pulmonary disease. PLoS One. 2017;12(2):e0172766. https://doi.org/10.1371/journal.pone.0172766.
De Beer CR, Van Rooijen AJ, Pretorius JP, Becker PJ, Rheeder P, Paruk F. Muscle strength and endurance to predict successful extubation in mechanically ventilated patients: a pilot study evaluating the utility of upper limb muscle strength and ergometry. S Afr J Crit Care. 2018;34(2):44–9. https://doi.org/10.7196/SAJCC.2018.v34i2.360.
Sessler CN, Gosnell MS, Grap MJ, Brophy GM, O’Neal PV, Keane KA, et al. The Richmond Agitation-Sedation Scale, Validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338–44. https://doi.org/10.1164/rccm.2107138.
Parry SM, Berney S, Granger CL, Dunlop DL, Murphy L, El-Ansary D, et al. A new two-tier strength assessment approach to the diagnosis of weakness in intensive care: an observational study. Crit Care. 2015;19(1):52. https://doi.org/10.1186/s13054-015-0780-5.
Kendall FP, McCreary EK, Provance PG, McIntyre Rodgers M, Romani WA. Muscles: testing and function with posture and pain. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2005.
Lee JJ, Waak K, Grosse-Sundrup M, Xue F, Lee J, Chipman D, et al. Global muscle strength but not grip strength predicts mortality and length of stay in a general population in a surgical intensive care unit. Phys Ther. 2012;92:1546–55. https://doi.org/10.2522/ptj.20110403.
Reck Medical Devices. MOTOmed Brochure. Available at http://www.motomed.com/en.html. Accessed 23 Sept 2023.
Burtin C, Clerckx B, Robbeets C, Ferdinande P, Langer D, Troosters T, et al. Early exercise in critically ill patients enhances short-term functional recovery. Crit Care Med. 2009;37(9):1–7.
STATA version 15.1 StataCorp LLC. http://www.stata.com or stata@stata.com.
Hol AT, Eng JJ, Miller WC, Sproule S, Krassioukov AV. Reliability and validity of the 6-minute arm test for the evaluation of cardiovascular fitness in individuals with spinal cord injury. Arch Phys Med Rehabil. 2007;88(4):489–95. https://doi.org/10.1016/j.apmr.2006.12.044.
Bulthuis Y, Drossaers-Bakker W, Oosterveld F, Van der Palen J, Van de Laar M. Arm crank ergometer is reliable and valid for measuring aerobic capacity during submaximal exercise. J Strength Cond Res. 2010;24(10):2809–15.
Swain DP, Franklin BA. VO2 reserve and the minimal intensity for improving cardiorespiratory fitness. Med Sci Sports Exerc. 2002;34(1):152–7.
Mitropoulos A, Gumber A, Crank H, Klonizakis M. Validation of an arm crank ergometer test for use in sedentary adults. J Sports Sci Med. 2017;16:558–64.
Balady G, Arena R, Sietsema K, Myers J, Coke L, Fletcher G, et al. Clinician’s guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation. 2010;122:191–225. https://doi.org/10.1161/CIR.0b013e3181e52e69.
Vignon P. Cardiovascular failure and weaning. Ann Transl Med. 2018;6(18):354. https://doi.org/10.21037/atm.2018.05.46.
Pinsky MR. Breathing as exercise: the cardiovascular response to weaning from mechanical ventilation. Intensive Care Med. 2000;26:1164–6. https://doi.org/10.1007/s001340000619.
Terson de Paleville DGL, McKay WB, Folz RJ, Ovechkin AV. Respiratory motor control disrupted by spinal cord injury: mechanisms, evaluation and restoration. Transl Stroke Res. 2011;2(4):463–73.
Vivier E, Roussey A, Doroszewski F, Rosselli S, Pommier C, Carteaux G, Dessap AM. Atrophy of diaphragm and pectoral muscles in critically ill patients. Anesthesiology. 2019;131:169–79.
Dres M, Dubé BP, Mayaux J, Delemazure J, Reuter D, Brochard L, Similowski T, Demoule A. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am J Respir Crit Care Med. 2017;195(1):57–66. https://doi.org/10.1164/rccm.201602-0367OC.
Yosef-Brauner O, Adi N, Shahar TB, Yehezkel E, Carmeli E. Effect of physical therapy on muscle strength, respiratory muscles and functional parameters in patients with intensive care unit-acquired weakness. Clin Respir J. 2015;9:1–6. https://doi.org/10.1111/crj.12091.
Cottereau G, Dres M, Avenel A, Fichet J, Jacobs FM, Prat D, et al. Handgrip strength predicts difficult weaning but not extubation failure in mechanically ventilated subjects. Respir Care. 2015;60(8):1097–104.
Efstathiou ID, Mavrou IP, Grigoriadis KE. Correlation between maximum inspiratory pressure and hand-grip force in healthy young and middle age individuals. Respir Care. 2016;61(7):925–9. https://doi.org/10.4187/respcare.04319.
Baess AI, Abdallah TH, Emara DM, Hassan M. Diaphragmatic ultrasound as a predictor of successful extubation from mechanical ventilation: thickness, displacement, or both? Egypt J Bronchol. 2016;10(2):162–6. https://doi.org/10.4103/1687-8426.184370.
Tu C-S, Chang C-H, Chang S-C, Lee C-S, Chang C-T. A decision for predicting successful extubation of patients in intensive care unit. Biomed Res Int. 2018;2018:6820975. https://doi.org/10.1155/2018/6820975.
Baptistella AR, Sarmento FJ, Da Silva KR, Baptistella SF, Taglietti M, Zuquello RA, Filho JRN. Predictive factors of weaning from mechanical ventilation and extubation outcome: a systematic review. J Crit Care. 2018;48:56–62. https://doi.org/10.1016/j.jcrc.2018.08.023.
Thille AW, Boissier F, Ghezala HB, Razazi K, Mekontso-Dessap A, Brun-Buisson C. Risk factors for and prediction by caregivers of extubation failure in ICU patients: a prospective study. Crit Care Med. 2015;43:613–20.
McArdle WD, Katch FI, Katch VL. Essentials of exercise physiology. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2006.
Acknowledgements
We thank the staff of the participating intensive care units.
Funding
The principle researcher received a research grant of 20,000 (ZAR) from the Critical Care Society of South Africa.
Author information
Authors and Affiliations
Contributions
CRdBB contributed to the literature search, data collection, study design, and manuscript preparation. AJvR contributed to the study design and review of the manuscript. PJB analyzed the data. FP reviewed the manuscript.
AJvR supervised and FP co-supervised the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Research Ethics Committee, Faculty of Health Sciences, University of Pretoria in 2017 (number 394/2017). All patients included gave informed consent to participate. Permission to conduct the study was also obtained from the CEO of Steve Biko Academic Hospital as well as the head of the Critical Care and Physiotherapy departments of the hospital respectively. The study complies with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Beer-Brandon, C.R., van Rooijen, A.J., Becker, P.J. et al. Upper limb muscle strength and exercise endurance as predictors of successful extubation in mechanically ventilated patients. Bull Fac Phys Ther 29, 19 (2024). https://doi.org/10.1186/s43161-024-00178-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43161-024-00178-7