
Abstract
Aim
To investigate the effectiveness of tele-rehabilitation for children diagnosed with unilateral cerebral palsy.
Method
The design of this study is a narrative review. An electronic search was conducted for studies that related to tele-rehabilitation using the following databases: CINAHL, PubMed, MEDLINE, OTSeeker, and PEDro. The data extracted were analyzed by evaluating them according to the key results, limitations, suitability of the methods used to the initial hypothesis, interpretation of the results, and impact of the conclusions in the field.
Results
Out of 139 studies, 3 studies met the inclusion criteria. Further, manual searches of the references of included studies identified 2 more relevant studies. The interventions applied in those studies were web-based multi-modal therapy program using Move-it-to-improve-it (Mitii™), home-based hand-arm bimanual intensive therapy (H-HABIT), and lower-extremity functional training (LIFT). The outcomes were executive functions, occupational performance, activity capacity, dexterity, quality of bimanual hand-use, functional goals, gait capacity, and performance.
Conclusion
Tele-rehabilitation is effective in improving the functions of the upper and lower extremities in daily living activities for children with unilateral cerebral palsy (UCP), aged between 2 to 18 years old, classified to levels I and II in GMFCS and levels I, II, and III in MACS. Webcam and good internet connection are essential requirements to conduct tele-rehabilitation. Children need to be contacted weekly via phone or e-mail for further follow-ups. Additionally, tele-rehabilitation may be considered one of the intervention strategies for patients who live in rural areas.
Similar content being viewed by others


Introduction
Cerebral palsy (CP) is a neurodevelopmental disorder that affects children’s development and limits their functions and activities. It occurs in 1.5 to 2.5 per 1000 live births [1]. CP is characterized according to the tone abnormalities and motor distributions abnormalities categorized as follows: [2] spastic CP (85–91%), [3] dyskinetic CP (4–7%), [4] ataxic CP (4–6%), and [5] hypotonic CP (2%). Dyskinetic, ataxic, and hypotonic CP mostly affect bilateral upper limbs and bilateral lower limbs, while spastic CP might be [2] hemiplegic CP which represent 38% of CP cases, diplegic CP (37%), and quadriplegic CP (24%) [6]. In Saudi Arabia, CP has the highest rate of prevalence among all children with neurological disorders (2.34 per 1000) [7].
The symptoms of CP include muscle tone abnormalities which are considered to be the most common symptoms among CP children. Hypertonicity, hyperreflexia, clonus, and poor coordination are also the symptoms of children diagnosed with CP. Other symptoms include feeding difficulties, drooling, hip dislocation, scoliosis, seizures, intellectual impairment, communication difficulties, and impaired vision and hearing; those symptoms cause many impairments for the child [8].
The most common impairment that CP children would have is upper limb impairment [9]. Another impairment that CP children would complain about is gross motor impairment. Those impairments reduce the speed of movement, accuracy, and coordination and cause a reduction in the independence of the activities of daily living (ADL) [10].
CP treatment depends on symptoms and impairments. The treatments have been divided into pharmacologic treatment (oral baclofen and botulinum toxin injection), which targets muscle tone abnormalities, and non-pharmacologic treatment, including surgical or rehabilitation treatment. Surgical treatment aims to reduce spasticity and improve gait kinematics, while rehabilitation programs may enhance motor development and help to prevent secondary deformities [11]. The outcomes of the surgical intervention may vary and could be difficult to be predicted [12].
Early intervention is essential for infants diagnosed with CP because infants who are not actively using their motor cortex may lose cortical connections and functions. An infant’s motor behavior increases by discovering and interacting with the environment. Hence, controlling and generating the growth, development of muscles, ligaments, and bones and development of the neuromotor system lead to improving the neuroplasticity [6]. Early interventions should include child-initiated movement combined with environment modification [13].
During pandemics and crises such as coronavirus (COVID-19), rehabilitation services would be almost impossible and difficult for children and their caregivers in the rehabilitation centers. One of the solutions that might be effective for children with disabilities for getting rehabilitation services is tele-rehabilitation [5].
Tele-rehabilitation has become an interest for many physical therapy professions especially during the crisis of COVID-19. World Confederation for Physical Therapy (WCPT) provided a global hub of resources to support the physiotherapy profession in its response to COVID-19, and advise the rapid, measured, and responsive way the global profession has responded, whereas tele-rehabilitation became a viable solution for offering rehabilitation services [5].
Tele-rehabilitation defines as a creative way to deliver rehabilitation services remotely using tele-communication technologies [14]. Communication between the therapist and the patient can be attained remotely by videoconferencing, e-mails, and texting [15]. Recent tele-communication technologies have given the chance for rehabilitation services to be delivered to the patients via the internet or other technology devices; research has shown effective improvement in a clinical outcome in cases with disabilities through tele-rehabilitation [2].
Recent studies have proven that tele-rehabilitation reinforces the early intervention for children diagnosed with CP [16]. Providing rehabilitation intervention at home (simulating the actual environment for the child) is better than having the intensive rehabilitation service at a day camp, which is the best motor skill that the child can learn [10].
Tele-rehabilitation might have many advantages such as reducing the cost for both therapists and patients and providing healthcare services for patients who live in rural areas and who have difficulties with transportation [15]. On the other hand, the required devices to provide therapeutic services are not flexible to be provided remotely [2]. Tele-rehabilitation could have some limitations because most of the interventions in the rehab centers included touching, handling, using machines such as treadmills, and performing specific tasks, which are difficult to be applied remotely [17]. Additionally, it is important to take the feedback from the patients and their caregivers to observe the outcomes during the rehabilitation that applied remotely [15].
Therefore, the purpose of this narrative review is to assess and synthesize the studies that used tele-rehabilitation to improve functions in daily activities. This will include investigating the effectiveness of tele-rehabilitation performed for children diagnosed with CP and investigate the psychometric properties of the outcome measures involved in the selected studies.
Method
Study design
The study design is a narrative review.
Search strategy
An electronic search was conducted for studies that were published in English which is related to tele-rehabilitation using the following databases: CINAHL, PubMed, MEDLINE, OTSeeker, and PEDro from 2010 to September 2021, using the medical subject heading (MeSH) or keywords such as “tele-rehabilitation,” “tele-health,” “tele-medicine,” and “remote rehabilitation,” and every set search included MeSH terms which was combined by AND cerebral palsy. Table 1 summarizes the process of searching. A flow diagram was added to depict the flow of the information of the collected data.
Inclusion and exclusion criteria
The included studies were selected according to the following inclusion criteria: [2] children diagnosed with CP [3]; RCT designs, as they are given one of the highest levels of evidence in the hierarchies rank studies ([4] children aged between 2 and 18 years old [5]; studies that are published from 2010 to September 2021, to focus in recent technologies; and [18] studies measured the functional outcomes whether upper limbs functions or lower limbs functions.
On the other hand, the exclusion criteria were [2] children diagnosed with other impairments or diseases such as acquired brain injury, psychological problems, Erb’s palsy, autism, and Down’s syndrome [3]; interventions applied in rehabilitation centers or hospital settings [4]; the outcomes that measured were not reliable to assess functional status [5]; other studies rather than RCTs; and [18] studies published before 2010.
Data extraction
The data extracted from each study were retrieved and include the citation details, participants’ characteristics, the interventions applied, the concluded outcomes, and the outcome measures that were performed to assess the improvement.
Data analysis
The data were analyzed through the critical assessment process by evaluating them according to the following: [2] key results, [3] limitations, [4] suitability of the methods used to the initial hypothesis, [5] interpretation of the results, and [18] impact of the conclusions in the field, according to [19]. Additionally, the psychometric properties of the outcome measures were investigated.
Results
Literature search and screening process
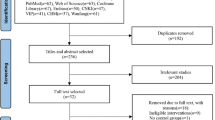
The process of the search strategy and screening of articles that were followed in the current review is shown in Fig. 1. The electronic databases search retrieved 139 articles. After removing 42 duplicates, 97 articles were title screened which resulted in 62 studies, and these studies were abstract screened critically which resulted in 31 studies. Full-text screening of all relevant articles yielded 3 studies that satisfied the eligibility. Further, manual searches of the references of included articles identified 2 more relevant studies.

Flow diagram depicting search strategy and article selection process
Characteristics of the included studies
The main findings are summarized in Table 2. Tele-rehabilitation was performed in 353 children diagnosed with unilateral cerebral palsy (UCP); the range of the age was between 2 and 18 years old. They were classified to levels I and II according to the Gross Motor Function Classification System (GMFCS) and levels I, II, and III according to Manual Ability Classification System (MACS).
The interventions were applied remotely including a web-based multi-model therapy program (Mitii), home-based hand-arm bimanual hand function intensive therapy (H-HABIT), and lower-extremity intensive functional training (LIFT). The main outcomes were functional outcomes including executive function, occupational performance, activity capacity, dexterity, bimanual hand function, and lower extremity function. The selected studies were assessed critically using the critical assessment process; Table 3 demonstrates the critical assessment in detail.
Web-based multi-modal therapy program
The studies ([20, 21], and [22] used Move-it-to-improve-it (Mitii), a multi-modal web-based program as a tele-rehabilitation to determine the effectiveness of the program to improve activity capacity, occupational performance, and executive function respectively in children with UCP compared with the control group (waitlist).
All the previous studies applied for the program in the home setting, and they were monitored via a computer and webcam. The duration of the intervention was performed for 20 weeks, 20–30 min per day, 6 days per week. They were contacted weekly via phone or e-mail to provide feedback and support. The outcome measures were taken remotely for both groups, at the baseline and after 20 weeks.
The program was varied according to the child’s needs. However, it included 40% of gross motor exercises such as squatting on balance foam by pretending to fly on a spaceship or shooting a pirate ship with a cannonball to perform for lunging. On the other hand, roughly 75% of the lower limb strengthening exercise was determined by task setting. The intensity of the exercise was increased weekly by increasing the repetition and speed of the task and height of the step.
Mitii showed no significant improvement in executive functions for children with UCP. In contrast, it showed an improvement in the motor skills and processing skills, activities of daily living, occupational performance, processing skills, goal attainment, visual processing, and physical capacity in children with UCP.
Home-based hand-arm bimanual intensive therapy (H-HABIT)
The study [23] used H-HABIT to investigate the efficacy of H-HABIT to improve the dexterity, functional performance, and bimanual performance in children with UCP compared with lower-limb intensive functional training (LIFT-control). Participants were monitored remotely via webcam software (Adobe Connect) during performing the exercises at home.
Children performed home-based activities under caregivers’ supervision for 2 h per day, 5 days per week, for 9 weeks. The H-HABIT group performed exercises in form of children’s fun sports including bimanual specific activities, environmental shaping to enhance bimanual hand-use, and grading of desired tasks. In LIFT-control, the exercises were performed as a fun game during functional tasks including ball kicking, hopscotch game, or walking over obstacles.
They hypothesized that H-HABIT would improve dexterity, quality of bimanual hand-use, and functional goals; the study interpreted that the H-HABIT program improves the dexterity and performance of functional goals, but there was no improvement in bimanual performance. Additionally, home-based rehabilitation programs provide a valuable family-centered approach to increase the rehabilitation intensity.
Lower-extremity intensive functional training (LIFT)
In the study [10], the effectiveness of LIFT was investigated compared with the control group which received H-HABIT to improve the gait and gross motor functions by improving the strength of the lower extremity and enhance the balance and coordination. The activities were monitored remotely using Adobe Connect once a week for 1 h.
LIFT was used to determine if there were any improvements in motor skills or strength. Strengthening domain included body weight exercises such as sit to stand, step up, and jumping; regarding the gait (motor skills), the lower extremities muscle group was targeted to be strengthened using body weight and thera-band such as bridging and clamshells. Regarding balance, children performed activities such as single-leg standing, and standing on unsteady surfaces, ball kicking, tandem walking, jumping jacks, and galloping/skipping to improve coordination. The program was performed daily, 2 h/day.
They concluded that intensive intervention for lower extremity applied at home environment given by caregivers has a significant improvement in gait capacity and performance. Tele-rehabilitation program using LIFT with remote supervision resulted in an improvement in ambulation distance and overall walking ability.
Outcome measures
The outcome measures used in the included studies were briefly described and investigated according to the population (condition and age) and psychometric properties (validity and reliability). Table 4 demonstrates the details regarding the results of the outcome measure investigation.
Discussion
This narrative review aims to evaluate and synthesize studies that used tele-rehabilitation to improve functions in daily activities for children with CP. This involved investigating the effectiveness of tele-rehabilitation for children with CP.
During pandemics and crises, tele-rehabilitation is the best solution that seems to be an effective treatment for children with disabilities during the pandemic; World Confederation for Physical Therapy (WCPT) provided a global hub of resources to support the physiotherapy profession to continue the rehabilitation programs during the pandemic [5]. The study [16] demonstrated that tele-rehabilitation is an alternative intervention to the usual rehabilitation at the rehabilitation center for children who live in rural areas and have transportation difficulties. Nevertheless, the frequency and duration of the rehabilitation intervention impact the improvement of the outcomes; the proper contact via phone or e-mail with the caregivers, at least once a week, may lead to greater improvements [18].
The effectiveness of tele-rehabilitation might have the same outcomes as compared to interventions that are applied face-to-face [18]. However, to promote effective tele-rehabilitation for children with CP, good internet connection is required to avoid the technical issues that occurred in the included studies ([20,21,22]. Furthermore, the included studies in our review did not mention any risk of injury that may be associated with tele-rehabilitation, as the caregivers have no experience regarding the proper rehabilitation for children diagnosed with CP.
This narrative review showed that tele-rehabilitation has significant effectiveness for children with UCP to improve functions (gait capacity and performance, occupational performance, dexterity, bimanual hand function, and lower extremity function); the age range was between 2 and 18 years old, levels I and II in GMFCS, and levels I, II and III in MACS. However, children with younger age were not included. Also, children with levels III, IV, and V in GMFCS and levels IV and V in MACS were not included as there is no evidence to support this hypothesis, which indicates certain barriers to be encountered in such cases. We have also noticed that all the selected studies included children diagnosed with UCP, which reflects that the result of our study can be applied to children with UCP only and not for all children with CP. In contrast, tele-rehabilitation has a significant improvement for other cases in other studies that were not included in our study as we focused only on CP cases.
From our point of view, treating children with levels III, IV, and V in GMFCS and levels IV and V in MACS might need special equipment and special techniques that the caregivers are unable to perform them as they do not have enough experience, which corresponds to the study [17], that tele-rehabilitation could have some limitations because most of the interventions in the rehab centers included touching, handling, or using machines and equipment such as treadmills or special tools to perform specific exercises, which are difficult to be applied remotely.
During investigating the outcome measures, we found that some of the included studies used invalid measurement tools for children aged from 2 to 18 years old. For example, BBT is a tool designed to assess gross manual dexterity for children aged between 6 and 19 years old [3]. Thus, the measurement tool is invalid for children younger than 6 years. Also, the 30-s chair rise is a test performed for adults with osteoarthritis [31] indicating that the outcome measure used in that study is invalid for young children. These outcome measures lead us to re-consider about the outcome measures that are supposed to be used in the field.
Given the above limitations, we are unable to generalize that tele-rehabilitation is effective for all children with CP just because the selected studies specified children with levels I and II GMFCS and levels I, II, and III on MACS.
Limitations of the study
This study is a narrative review; a risk of bias or quality assessment of the included studies was not performed in this review. Additionally, the included studies were all RCTs because they are given the highest level of evidence in the hierarchies rank studies. Furthermore, there were clear methodological limitations in the included articles which could have influenced the findings of this review, for example, the selected studies did not include children with moderate or severe disability given that all children were levels I and II on GMFCS and levels I, II, and III on MACS, which affect on the results of the treatment for children with moderate or severe disabilities. Also, the included studies did not mention any risk of injury that may be associated with tele-rehabilitation, which may influence the treatment and cause complications and difficulties for the patients.
Recommendations for research
Further studies are recommended by performing a quality assessment for the selected studies in form of a systematic review. Additionally, it is recommended to include other studies rather than RCTs for further investigation regarding the effectiveness of tele-rehabilitation. Risk of injury associated with tele-rehabilitation should also be investigated. All levels of disability children are suggested being included.
Conclusion
The findings of this narrative review showed that tele-rehabilitation is effective in improving the functions of the upper and lower extremities in daily living activities (gait capacity and performance, occupational performance, dexterity, bimanual hand function, and lower extremity function) for children diagnosed with UCP, aged between 2 and 18 years old, classified to levels I and II in GMFCS and levels I, II, and III in MACS.
Children should be monitored via a webcam and good internet connection. In addition, they should be supervised by therapists for at least once weekly via a phone, e-mail, or video conference to promote an effective tele-rehabilitation. The suggested duration and intensity are 30 min for 5 days weekly regarding the Mitii and 2 h for 5–6 days regarding performing LIFT or H-HABIT. Additionally, tele-rehabilitation may be considered one of the intervention strategies for patients who live in rural areas. Tele-rehabilitation should be performed with caution; the children should be monitored and followed up frequently to prevent the risks of injury that may occur during performing the suggested intervention that is performed remotely.
Availability of data and materials
No data and materials are available for this review.
Abbreviations
- 1MWT:
-
1-Minute Walk Test
- 30-s chair rise:
-
30 Seconds Chair Rise
- 6MWT:
-
6-Minute Walk Test
- ABILOCO-Kids:
-
A Measure of Locomotion Ability for Children
- ADL :
-
Activities of daily living
- AHA:
-
Assisting Hand Assessment
- AMPS:
-
Assessment of Motor and Process Skills
- BBT:
-
Box and Blocks Test
- BRIEF:
-
Behavior Rating Inventory of Executive Function
- COPM:
-
Canadian Occupational Performance Measure
- COVID-19:
-
Coronavirus disease 2019
- CP:
-
Cerebral palsy
- D-KEFS:
-
Delis–Kaplan Executive Function System
- GMFCS:
-
Gross Motor Function Classification System
- H-HABIT :
-
Home-Based Hand-Arm Bimanual Intensive Therapy
- JTTHF:
-
Jebsen–Taylor Test of Hand Function
- LIFE-H:
-
Assessment of Life Habits
- LIFT :
-
Lower-Extremity Functional Training
- MACS :
-
Manual Ability Classification System
- Mitii :
-
Move-it-to-improve-it
- Mob- Ques28:
-
28-item Mobility Questionnaire
- MUUL:
-
Melbourne Assessment of Unilateral Upper Limb Function
- N :
-
Number
- N/A:
-
Not applicable
- SLS:
-
Single-leg stance
- TVPS-3:
-
Test of Visual Perceptual Skill (non-motor) 3rd edition
- UCP :
-
Unilateral cerebral palsy
- WISC-IV-SF:
-
Wechsler Intelligence Scale for Children, Fourth Edition Short-Form
References
Hallman-Cooper JL, Rocha Cabrero F. Cerebral palsy. In StatPearls: StatPearls Publishing; 2021. http://www.ncbi.nlm.nih.gov/pubmed/30844174
Agostini M, Moja L, Banzi R, Pistotti V, Tonin P, Venneri A, et al. Telerehabilitation and recovery of motor function: a systematic review and meta-analysis. J Telemed Telecare. 2015;21(4):202–13. https://doi.org/10.1177/1357633X15572201.
Araneda R, Ebner-Karestinos D, Paradis J, Saussez G, Friel KM, Gordon AM, et al. Reliability and responsiveness of the Jebsen-Taylor test of hand function and the box and block test for children with cerebral palsy. Dev Med Child Neurol. 2019;61(10):1182–8. https://doi.org/10.1111/dmcn.14184.
Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine; 2011. https://doi.org/10.1097/PRS.0b013e318219c171.
Bury, T. J., & Stokes, E. K. (2020). On “musculoskeletal physical therapy during the COVID-19 pandemic: is Telerehabilitation the answer?” Turolla a, Rossettini G, Viceconti a, Palese a, Geri T. Phys Ther. 2020;100:1260-1264. Physical therapy, 100(10), 1883. https://doi.org/10.1093/ptj/pzaa131.
Novak I, Morgan C, Adde L, Blackman J, Boyd RN, Brunstrom-Hernandez J, et al. Early, accurate diagnosis and early intervention in cerebral palsy: advances in diagnosis and treatment. JAMA Pediatr. 2017;171(9):897–907. https://doi.org/10.1001/jamapediatrics.2017.1689.
Mohamed Madi S, Mandy A, Aranda K. The perception of disability among mothers living with a child with cerebral palsy in Saudi Arabia. Global Qualitative Nursing Research. 2019;6 https://doi.org/10.1177/2333393619844096.
Sewell MD, Eastwood DM, Wimalasundera N. Managing common symptoms of cerebral palsy in children. BMJ (Online). 2014;349(September):1–13. https://doi.org/10.1136/bmj.g5474.
Comans T, Mihala G, Sakzewski L, Boyd RN, Scuffham P. The cost-effectiveness of a web-based multimodal therapy for unilateral cerebral palsy: the Mitii randomized controlled trial. Dev Med Child Neurol. 2017;59(7):756–61. https://doi.org/10.1111/dmcn.13414.
Surana BK, Ferre CL, Dew AP, Brandao M, Gordon AM, Moreau NG. Effectiveness of lower-extremity functional training (LIFT) in young children with unilateral spastic cerebral palsy: a randomized controlled trial. Neurorehabil Neural Repair. 2019;33(10):862–72. https://doi.org/10.1177/1545968319868719.
Chin EM, Gwynn HE, Robinson S, Hoon AH. Principles of medical and surgical treatment of cerebral palsy. Neurol Clin. 2020;38(2):397–416. https://doi.org/10.1016/j.ncl.2020.01.009.
Khamis S, Herman T, Krimus S, Danino B. Is functional electrical stimulation an alternative for orthotics in patients with cerebral palsy? A literature review. Eur J Paediatr Neurol. 2018;22(1):7–16 https://doi.org/10.1016/j.ejpn.2017.10.004.
Morgan C, Darrah J, Gordon AM, Harbourne R, Spittle A, Johnson R, et al. Effectiveness of motor interventions in infants with cerebral palsy: a systematic review. Dev Med Child Neurol. 2016;58(9):900–9. https://doi.org/10.1111/dmcn.13105.
Jiang S, Xiang J, Gao X, Guo K, Liu B. The comparison of telerehabilitation and face-to-face rehabilitation after total knee arthroplasty: a systematic review and meta-analysis. J Telemed Telecare. 2018;24(4):257–62 https://doi.org/10.1177/1357633X16686748.
Peretti A, Amenta F, Tayebati SK, Nittari G, Mahdi SS. Telerehabilitation: review of the state-of-the-art and areas of application. JMIR Rehabilitation and Assistive Technologies. 2017;4(2):e7. https://doi.org/10.2196/rehab.7511.
Molinaro, A., Micheletti, S., Pagani, F., Garofalo, G., Galli, J., Rossi, A., Fazzi, E., & Buccino, G. (2020). Action observation treatment in a tele-rehabilitation setting: a pilot study in children with cerebral palsy. Disabil Rehabil, 0(0), 1–6. https://doi.org/10.1080/09638288.2020.1793009.
Unterholzner, L., Carrer, M., Bär, A., Beikircher, B., Dämon, B., Losso, A., Prendin, A. L., & Mayr, S. (2020). Sc Sc.
Camden, C., Pratte, G., Fallon, F., Couture, M., Berbari, J., & Tousignant, M. (2019). Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: results from a systematic review. Disabil Rehabil, 0(0), 1–13. https://doi.org/10.1080/09638288.2019.1595750.
Ferrari R. Writing narrative style literature reviews. Medical Writing. 2015;24(4):230–5. https://doi.org/10.1179/2047480615z.000000000329.
James S, Ziviani J, Ware RS, Boyd RN. Randomized controlled trial of web-based multimodal therapy for unilateral cerebral palsy to improve occupational performance. Dev Med Child Neurol. 2015;57(6):530–8 https://doi.org/10.1111/dmcn.12705.
Mitchell LE, Ziviani J, Boyd RN. A randomized controlled trial of web-based training to increase activity in children with cerebral palsy. Dev Med Child Neurol. 2016;58(7):767–73 https://doi.org/10.1111/dmcn.13065.
Piovesana A, Ross S, Lloyd O, Whittingham K, Ziviani J, Ware RS, et al. Randomized controlled trial of a web-based multi-modal therapy program for executive functioning in children and adolescents with unilateral cerebral palsy. Disabil Rehabil. 2017;39(20):2021–8. https://doi.org/10.1080/09638288.2016.1213899.
Ferre CL, Brandão M, Surana B, Dew AP, Moreau NG, Gordon AM. Caregiver-directed home-based intensive bimanual training in young children with unilateral spastic cerebral palsy: a randomized trial. Dev Med Child Neurol. 2017;59(5):497–504. https://doi.org/10.1111/dmcn.13330.
Crawford JR, Anderson V, Rankin PM, MacDonald J. An index-based short-form of the WISC-IV with accompanying analysis of the reliability and abnormality of differences. Br J Clin Psychol. 2010;49(2):235–58. https://doi.org/10.1348/014466509X455470.
Delis DC, Kramer JH, Kaplan E, Holdnack J. Reliability and validity of the Delis-Kaplan executive function system: an update. J Int Neuropsychol Soc. 2004;10(2):301–3. https://doi.org/10.1017/S1355617704102191.
Ezpeleta L, Granero R, Penelo E, de la Osa N, Domènech JM. Behavior rating inventory of executive functioning–preschool (BRIEF-P) applied to teachers: psychometric properties and usefulness for disruptive disorders in 3-year-old preschoolers. J Atten Disord. 2015;19(6):476–88. https://doi.org/10.1177/1087054712466439.
Holmefur MM, Krumlinde-Sundholm L. Psychometric properties of a revised version of the assisting hand assessment (kids-AHA 5.0). Dev Med Child Neurol. 2016;58(6):618–24 https://doi.org/10.1111/dmcn.12939.
McDowell BC, Kerr C, Parkes J, Cosgrove A. Validity of a 1 minute walk test for children with cerebral palsy. Dev Med Child Neurol. 2005;47(11):744–8 https://doi.org/10.1017/S0012162205001568.
Martakis K, Stark C, Rehberg M, Semler O, Duran I, Schoenau E. One-minute walk test in children with cerebral palsy GMFCS level 1 and 2: reference values to identify therapeutic effects after rehabilitation. Developmental Neurorehabilitation. 2020;23(4):201–9 https://doi.org/10.1080/17518423.2019.1625981.
de Baptista CRJA, Vicente AM, Souza MA, Cardoso J, Ramalho VM, Mattiello-Sverzut AC. Methods of 10-meter walk test and repercussions for reliability obtained in typically developing children. Rehabilitation Research and Practice. 2020;2020:1–7. https://doi.org/10.1155/2020/4209812.
Silva PFS, Quintino LF, Franco J, Faria CDCM. Measurement properties and feasibility of clinical tests to assess sit-to-stand/stand-to-sit tasks in subjects with neurological disease: a systematic review. Brazilian Journal of Physical Therapy. 2014;18(2):99–110. https://doi.org/10.1590/s1413-35552012005000155.
Sember V, Grošelj J, Pajek M. Balance tests in pre-adolescent children: retest reliability, construct validity, and relative ability. Int J Environ Res Public Health. 2020;17(15):1–13. https://doi.org/10.3390/ijerph17155474.
Gilles CD, Arnould C, Thonnard JL, Lejeune TM. Abiloco-kids: a Rasch-built 10-item questionnaire for assessing locomotion ability in children with cerebral palsy. J Rehabil Med. 2008;40(10):823–30 https://doi.org/10.2340/16501977-0267.
Fitzgerald D, Hickey C, Delahunt E, Walsh M, O’Brien T. Six-minute walk test in children with spastic cerebral palsy and children developing typically. Pediatr Phys Ther. 2016;28(2):192–9 https://doi.org/10.1097/PEP.0000000000000224.
Van Ravesteyn NT, Dallmeijer AJ, Scholtes VA, Roorda LD, Becher JG. Measuring mobility limitations in children with cerebral palsy: Interrater and intrarater reliability of a mobility questionnaire (MobQues). Dev Med Child Neurol. 2010;52(2):194–9. https://doi.org/10.1111/j.1469-8749.2009.03341.x.
O’Neil ME, Fragala-Pinkham MA, Forman JL, Trost SG. Measuring reliability and validity of the ActiGraph GT3X accelerometer for children with cerebral palsy: a feasibility study. J Pediatr Rehabil Med. 2014;7(3):233–40. https://doi.org/10.3233/PRM-140292.
Noreau L, Lepage C, Boissiere L, Picard R, Fougeyrollas P, Mathieu J, et al. Measuring participation in children with disabilities using the assessment of Life habits. Dev Med Child Neurol. 2007;49(9):666–71. https://doi.org/10.1111/j.1469-8749.2007.00666.x.
Payne S, Howell C. An evaluation of the clinical use of the assessment of motor and process skills with children. Br J Occup Ther. 2005;68(6):277–80. https://doi.org/10.1177/030802260506800606.
Sığırtmaç İC, Öksüz Ç. Investigation of reliability, validity, and cutoff value of the Jebsen-Taylor hand function test. J Hand Ther. 2020. https://doi.org/10.1016/j.jht.2020.01.004.
Randall M, Carlin JB, Chondros P, Reddihough D. Reliability of the Melbourne assessment of unilateral upper limb function. Dev Med Child Neurol. 2001;43(11):761–7. https://doi.org/10.1111/j.1469-8749.2001.tb00158.x.
Verkerk GJQ, Wolf MJMAG, Louwers AM, Meester-Delver A, Nollet F. The reproducibility and validity of the Canadian occupational performance measure in parents of children with disabilities. Clin Rehabil. 2006;20(11):980–8. https://doi.org/10.1177/0269215506070703.
Chan PLC, Chow SMK. Reliability and validity of the test of visual-perceptual skills (non-motor) - revised for Chinese preschoolers. Am J Occup Ther. 2005;59(4):369–76. https://doi.org/10.5014/ajot.59.4.369.
Acknowledgements
This study was supported by the Faculty of Applied Medical Science, Umm Al-Qura University. We would like to express our special thanks to Dr. Shamekh M. El-Shamy for his guidance and support that made it possible for this study to be complete. We would like to take this opportunity to thank everyone who has helped and encouraged us throughout our studies; your support has been priceless.
Funding
No financial support was received for this review.
Author information
Authors and Affiliations
Contributions
All authors contributed to this paper. S.M.E was responsible for the conception; M.E.T conducted the entire review, with S.S.A as a second reviewer. All authors were involved with the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained by the Biomedical Research Ethics Committee of Umm Al-Qura University. Approval No. (HAPO-02-K-012-2021-04-657).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tamboosi, M.E., Al-Khathami, S.S. & El-Shamy, S.M. The effectiveness of tele-rehabilitation on improvement of daily living activities in children with cerebral palsy: narrative review. Bull Fac Phys Ther 26, 40 (2021). https://doi.org/10.1186/s43161-021-00055-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43161-021-00055-7