
Abstract
Background
Dermoid cysts are benign germ cell tumors with ectodermal and mesodermal components. It is a slow-growing lesion that commonly arises in the midline of the head and neck. The last location represented 7%, and the periorbital region was the most frequently arising area. True lateral neck dermoid cysts are rare. We present an unusual location of a dermoid cyst in a newborn.
Case presentation
We report an unusual location of a 10-day newborn giant dermoid cyst with multiple implantation sites, namely the shoulder, scapula, cervical, temporal, and occipital scalp. Successful surgical resection was achieved, and the patient was discharged after the removal of the stitches.
Conclusion
Dermoid cysts are unusual neoplasms with rare diagnoses at birth, but often in childhood. Concomitant implantation locations on the shoulder, neck, temporal, and occipital scalps are rare.
Similar content being viewed by others


Background
Dermoid cysts are benign germ cell tumors with ectodermal and mesodermal components. Histologically, it contains adnexal structures, such as hair, follicles, sweat, and sebaceous glands, surrounded by keratinizing squamous cells [1, 2]. Its incidence is approximately 1 in 4000 births, with a slight female predominance. Dermoid cysts are mostly congenital; however, 70% of them are diagnosed after 5 years of age. They exhibit slow-growing characteristics; their size can vary but reach up to 17 cm. These lesions can arise anywhere in the body; nonetheless, only 7% have been reported in the head and neck region. In the latter region, dermoid cysts are well known to appear in the midline and most often in the periorbital area. Many locations have been reported in the literature; however, the true lateral neck location and upper shoulder area are rare [3,4,5].
In this study, we report a case of an unusual shoulder, scapula, lateral neck, temporal, and occipital scalp implantation-based large newborn dermoid cyst. We also reviewed different dermoid cyst locations reported in the literature.
Case presentation
A 10-day newborn female with an unknown medical history from a poorly monitored pregnancy with two prenatal care visits, full-term born, was referred to the neurosurgical department for a congenital right lateral cervical mass.
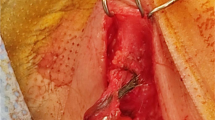
The patient’s hemodynamic and ventilation conditions were good on admission with no fever. Physical examination revealed a painless right lateral cervical cyst, presenting a regular shape with a soft consistency, measuring 14 cm in length and 8 cm in width (Fig. 1). The cyst was implanted on the lateral cervical, scalp edge, and upper shoulder, extending posteriorly to the scapula. Other examinations were unremarkable, with no other associated anomalies or deformities. Computed tomography was obtained, which showed a right lateral cervical bilocular mass measuring 9.9 cm × 7.6 cm on the axial section, a fluid-filled lesion external to the skull, cervical canal, and thorax that did not compress the trachea (Fig. 2). Based on these findings, our differential diagnoses included cystic lymphangioma, cystic teratoma, and cervical choristoma.

A, B The anterior and posterior aspects of the cyst and its implantation and extension, respectively. C The postoperative 10-day surgical wound after stitches were removed

A, C A right lateral neck mass non-extended in the vertebral canal C nor the thoracic cavity. B, D The scalp attaches without intracranial extension
Surgical resection was performed under general anesthesia, and the mass was removed from the scalp, cervical canal, and shoulder. The histopathology was consistent with a dermoid cyst (Fig. 3). The postoperative period was uneventful, the surgical wound healed, and the patient was discharged after the removal of the stitches.

Describe the dermoid cyst wall with a completely attenuated lining comprised of smooth and skeletal muscle bundles, adipose tissue, and congested cavernous blood vessels
Literature review
A literature review was conducted using PubMed and Google Scholar databases, and the following search terms were used [(((cervical) OR (neck)) AND (dermoid)) AND (cyst)]. The selection criteria were dermoid cysts with histopathological confirmation, published from 2000 to 2023, regardless of the dermoid cyst location and publication language. The publications outside of that time span were excluded. The following information on age, gender, size, and location was extracted and analyzed using SPSS software. Overall, 37 cases were selected; there were 18 men (48.6%) and 19 women (51.4%), and the mean age was 27.63 ranging, 1 month to 75 years). The most reported location was the submental in 40.5% of cases, followed by the parotid gland (10.8%) (Table 1). The mean cyst was 4.85 cm ranging from 0.13 to 14 cm. The chi-square test was carried out to assess the difference in size according to the location; no significant difference was found (P value > 0.05).
Discussion
Dermoid cysts are slow-growing benign lesions that arise from the entrapment of ectodermal elements along embryonic closure lines. It is the second most common midline neck cyst, representing 25% of all congenital cystic masses of the neck [18, 40]. Despite its congenital origin, an acquired etiology was also reported to account for 10% of dermoid cysts due to trauma or implantation of epithelial cells in utero [15]. Dermoid cysts may occur anywhere in the body, with approximately 7% of cases reported in the head and neck [5]. In the last region, the periorbital dermoid cyst is the most commonly encountered, and Pryor et al. and Choi et al. reported 61% and 84% of periorbital locations [2, 4]. Dermoid cysts of the head and neck were previously classified into four groups by New and Erich [41]: group 1 periorbital, group 2 nose, group 3 submental, and group 4 midventral and mid-dorsal fusion area of the suprasternal, thyroidal, and suboccipital regions. However, many cases were found later, and the relative location was not included in the New and Erich classification, which Pryor grouped and named “head, not neck.” Choi et al. found it necessary to further develop these classifications to integrate the ear and scalp regions and extend intracranially [2, 42]. In this case, the cyst extended from the shoulder to the temporal-occipital scalp and scapula, without intracranial and intravertebral canal or intrathoracic extension. A complete classification integrating all dermoid cysts may be difficult because unusual locations still appear and may not be predictive. Imaging investigations are fundamental for the assessment of the anatomical relationship with the surrounding structures. It can allow anatomical study of the lesion and its extension and help with the resection plan. We first rolled out the intracranial and intravertebral canal extensions in this case using CT.
The diagnosis remains challenging; congenital lateral neck cystic lesions, such as cystic hygroma, cystic teratoma, epidermoid cyst, and lymphangioma, may be considered in the preliminary differential diagnosis. These lesions often present as painless, soft, compressible, non-tender transluminal masses. The presentation can sometimes be related to complications such as respiratory distress, feeding difficulty, and lesion infection. Histology remains the only tool to differentiate between these lesions and provide a final diagnosis [43, 44].
Dermoid cysts are common in infants and adults. The mean age of the cases reported in the last decade was 27.63 years ranging from 0 to 75 years. Pryor et al. reported the mean age at presentation was 39 months [2]. Additionally, Choi et al. enrolled 62 patients with dermoid cysts; almost half of them were older than six [4]. In this case, the diagnosis was made at birth, and the reason may be the huge size and its location; we think the age of the diagnosis may depend on the lesion's location and size. Therefore, small dermoid cysts in a hidden location may not be visible at birth or may be neglected by parents. This can explain why many childhood or adult cases are diagnosed after the lesion grows and may become symptomatic.
Overall, the prognosis for these lesions was good when complete surgical resection was achieved. Many authors reported no recurrence in their series, and the patients recovered very well [10, 15, 31].
Conclusion
Dermoid cysts are unusual neoplasms with rare diagnoses at birth, but often in childhood. Concomitant implantation locations on the shoulder, neck, temporal, and occipital scalps are rare. In this case, it would be wise to roll out intracranial and intravertebral canal extensions by imaging prior to the removal attempt. The prognosis was good with no recurrence after complete resection.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Chorney SR, Irace AL, Sobin L. Cervical dermoid cysts. Oper Tech Otolaryngol-Head Neck Surg. 2017;28(3):179–82. https://doi.org/10.1016/j.otot.2017.05.017.
Pryor SG, Lewis JE, Weaver AL, Orvidas LJ. Pediatric dermoid cysts of the head and neck. Otolaryngol-Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg. 2005;132(6):938–42. https://doi.org/10.1016/j.otohns.2005.03.005.
Diercks GR, Iannuzzi RA, McCowen K, Sadow PM. Dermoid cyst of the lateral neck associated with the thyroid gland: a case report and review of the literature. Endocr Pathol. 2013;24(1):45–8. https://doi.org/10.1007/s12022-013-9234-2.
Choi JS, Bae YC, Lee JW, Kang GB. Dermoid cysts: epidemiology and diagnostic approach based on clinical experiences. Arch Plast Surg. 2018;45(6):512–6. https://doi.org/10.5999/aps.2018.00017.
Vavro M, Horák S, Dvoranová B, et al. Rare location of a dermoid cyst in the parotid gland: a case report. Prague Med Rep. 2022;123(3):193–8. https://doi.org/10.14712/23362936.2022.18.
Taha A, Enodien B, Frey DM, Taha-Mehlitz S. Thyroglossal duct cyst, a case report and literature review. Dis Basel Switz. 2022;10(1). https://doi.org/10.3390/diseases10010007
Bali R, Sharma P, Sangwan V, Gupta H. Branchial cleft cyst versus dermoid cyst of digastric triangle: report of two cases. J Maxillofac Oral Surg. 2009;8(1):81–4. https://doi.org/10.1007/s12663-009-0020-0.
Graham RM, Thomson EF, Woodwards RTM, Sloan P. Lateral dermoid cyst. Br J Oral Maxillofac Surg. 2008;46(2):131–2. https://doi.org/10.1016/j.bjoms.2006.10.015.
Gattia KVN, Kacouchia NB, Kouassi YM, Kouassi-Ndjeundo J, Vroh Bi TS, Abouna AD. Submandibular dermoid cyst extended to the cervical region. Rev Stomatol Chir Maxillofac. 2012;113(3):173–5. https://doi.org/10.1016/j.stomax.2012.02.003.
Papadogeorgakis N, Kalfarentzos EF, Vourlakou C, Alexandridis C. Surgical management of a large median dermoid cyst of the neck causing airway obstruction. A case report Oral Maxillofac Surg. 2009;13(3):181–4. https://doi.org/10.1007/s10006-009-0165-5.
Shah SP, Quiroz F, Shah CJ. Dermoid cyst. Ultrasound Q. 2012;28(3):215–7. https://doi.org/10.1097/RUQ.0b013e318266d322.
Boko E, Amaglo K, Kpemissi E. A bulky dermoid cyst of the floor of the mouth. Eur Ann Otorhinolaryngol Head Neck Dis. 2014;131(2):131–4. https://doi.org/10.1016/j.anorl.2013.01.003.
Kyriakidou E, Howe T, Veale B, Atkins S. Sublingual dermoid cysts: case report and review of the literature. J Laryngol Otol. 2015;129(10):1036–9. https://doi.org/10.1017/S0022215115001887.
Sahoo NK, Choudhary AK, Srinivas V, Tomar K. Dermoid cysts of maxillofacial region. Med J Armed Forces India. 2015;71(2):S389-394. https://doi.org/10.1016/j.mjafi.2013.11.004.
Kusuyama Y, Takeuchi N, Wakabayashi K, Yura Y. Dermoid cyst of the lateral neck included within the submandibular gland. J Craniofac Surg. 2016;27(1):e33-34. https://doi.org/10.1097/SCS.0000000000002300.
Tekkesin MS, Ozer N, Olgac V. Sublingual dermoid cyst: a case report. Turk J Pathol Published online. 2014. https://doi.org/10.5146/tjpath.2014.01236.
Somashekhar SN. Dermoid cyst of neck: a diagnostic dilemma and a therapeutic challenge. Int J Head Neck Surg. 2017;8(3):125–7. https://doi.org/10.5005/jp-journals-10001-1320.
Dwivedi G, Saxena P, Patnaik U, Kumari A, Sood A. Dermoid cyst floor of mouth: a diagnostic conundrum. Indian J Otolaryngol Head Neck Surg Off Publ Assoc Otolaryngol India. 2022;74(Suppl 2):1961–3. https://doi.org/10.1007/s12070-020-01939-1.
Giarraputo L, Savastano S, D’Amore E, Baciliero U. Dermoid cyst of the floor of the mouth: diagnostic imaging findings. Cureus. 2018;10(4):e2403. https://doi.org/10.7759/cureus.2403.
Sauer A, Abrol A, Cabrera CI, Shah J. A pediatric lateral submental mass: a rare presentation of dermoid cyst. Ear Nose Throat J. Published online May 25, 2021:1455613211019787. https://doi.org/10.1177/01455613211019787
Yang C, Wang X, Zhang S, Wu D. Dermoid cyst of the parotid gland location. J Craniofac Surg. 2020;31(7):e698–9. https://doi.org/10.1097/SCS.0000000000006655.
Yigit N, Karslioglu Y, Yildizoglu U, Karakoc O. Dermoid cyst of the parotid gland: report of a rare entity with literature review. Head Neck Pathol. 2015;9(2):286–92. https://doi.org/10.1007/s12105-014-0563-3.
Islam S, Hoffman GR. Parotid dermoid cyst: a rare entity. J Laryngol Otol. 2009;123(2): e7. https://doi.org/10.1017/S0022215109004447.
Samal S, Sable MN, Pradhan S, Pradhan P. Intraconal orbital dermoid cyst: a rare location. Autopsy Case Rep. 2021;11:e2021282. https://doi.org/10.4322/acr.2021.282.
Maeng MM, Godfrey KJ, Kazim M. Multilobular dermoid cyst of the orbit. Orbit. 2019;38(4):328–30. https://doi.org/10.1080/01676830.2018.1509098.
Pham NS, Dublin AB, Strong EB. Dermoid cyst of the orbit and frontal sinus: a case report. Skull Base Off J North Am Skull Base Soc Al. 2010;20(4):275–8. https://doi.org/10.1055/s-0030-1247631.
Al-Muhaimeed HS, Abdelwahed HY, Elgamal EA, Alokby GM, Binnasser AM, Ashraf MM. Extradural dermoid cyst of mastoid bone: a case report. Case Rep Otolaryngol. 2012;2012:548340. https://doi.org/10.1155/2012/548340.
Jonas RH, Casazza GC, Dibbern M, Kesser BW. Congenital dermoid cyst in an atretic ear. Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc Eur Acad Otol Neurotol. 2022;43(3):e397–8. https://doi.org/10.1097/MAO.0000000000003449.
Nagendra V, Phatak SV, Patwa PA, Pattabiraman S, Prashanti G. Neck dermoid cyst with rare imaging appearance on ultrasound, elastography, and computed tomography. J Clin Diagn Res Published online. 2022. https://doi.org/10.7860/JCDR/2022/58087.16990.
Santrac N, Goran M, Markovic I, et al. A rare case of dermoid cyst of the neck - clinical presentation and surgical treatment. Endocr Abstr. Published online May 13, 2016. https://doi.org/10.1530/endoabs.41.EP348
Zhao H, Cao Z, Gu Z. Dermoid cyst of nasal tip and nasal septum. J Craniofac Surg. 2022;33(5):e454–6. https://doi.org/10.1097/SCS.0000000000008281.
Ülkü ÇH, Yücel H. Dermoid cyst arising from the epiglottis. Turk Arch Otorhinolaryngol. 2015;53(1):42–4. https://doi.org/10.5152/tao.2014.664.
Jeong J, Choi YJ, Lee K, Choi HS. Dermoid cyst in the postauricular area. J Craniofac Surg. 2020;31(7):e664–5. https://doi.org/10.1097/SCS.0000000000006499.
Ma X, Xiao J, Wang W. Retroperitoneal dermoid cyst mimicking a liposarcoma based on imaging assessment: case report and literature review. Gland Surg. 2021;10(6):2062–8. https://doi.org/10.21037/gs-21-65.
Partha Sri M, Prabhat AK, Dammalapati MR, et al. Dermoid cyst of the penis: a case report of an unusual penile mass. Cureus. 2022;14(10):e30227. https://doi.org/10.7759/cureus.30227.
Signorelli F, Montano N, Scerrati A, Cioni B, Papacci F. Isolated intramedullary cervical dermoid cyst. Acta Neurol Belg. 2014;114(3):223–4. https://doi.org/10.1007/s13760-013-0241-3.
Nakajima K, Korekawa A, Nakano H, Sawamura D. Subcutaneous dermoid cysts on the eyebrow and neck. Pediatr Dermatol. 2019;36(6):999–1001. https://doi.org/10.1111/pde.13976.
Rinna C, Reale G, Calafati V, Calvani F, Ungari C. Dermoid cyst: unusual localization. J Craniofac Surg. 2012;23(5):e392-394. https://doi.org/10.1097/SCS.0b013e31825ab1e1.
Robinson L, Sengoatsi T, van Heerden WFP. Concomitant congenital intraoral dermoid cyst and heterotopic gastrointestinal cyst. Head Neck Pathol. 2021;15(1):298–302. https://doi.org/10.1007/s12105-020-01160-0.
Shareef S, Ettefagh L. Dermoid cyst. In: StatPearls. StatPearls Publishing; 2022. https://europepmc.org/article/nbk/nbk560573.
McAvoy JM, Zuckerbraun L. Dermoid cysts of the head and neck in children. Arch Otolaryngol - Head Neck Surg. 1976;102(9):529–31. https://doi.org/10.1001/archotol.1976.00780140061004.
Choi HJ. Bilateral lambdoid dermoid cyst. J Craniofac Surg. 2014;25(4):e321-322. https://doi.org/10.1097/SCS.0000000000000585.
Mirza B, Ijaz L, Saleem M, Sharif M, Sheikh A. Cystic hygroma: an overview. J Cutan Aesthetic Surg. 2010;3(3):139. https://doi.org/10.4103/0974-2077.74488.
Hsieh YY, Hsueh S, Hsueh C, et al. Pathological analysis of congenital cervical cysts in children: 20 years of experience at Chang Gung Memorial Hospital. Chang Gung Med J. 2003;26(2):107–13.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from public, commercial, or not-for-profit funding agencies.
Author information
Authors and Affiliations
Contributions
The authors contributed equally. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent to participate was obtained from the parent. This publication fulfills the ethical requirements of the Declaration of Helsinki.
Consent for publication
Written Informed consent has been obtained from the patient parents to publish the case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rabiou, M.S., Moussa, M.R.H., Amadou, H.A. et al. An unusual location of newborn huge dermoid cyst: a case report and literature review. Ann Pediatr Surg 19, 39 (2023). https://doi.org/10.1186/s43159-023-00266-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43159-023-00266-8