
Abstract
Background
Since the first report of COVID-19 in 2019, information released has been fast and vast. Health literacy focuses on individual skills to obtain, process, and understand health information and services necessary to make informed health decisions. Increasing the level of health literacy can be addressed by the provision of high-quality, trustworthy, easy-to-access, and easy-to-understand information about COVID-19. This work aimed to assess COVID-19-related health literacy in the Egyptian population living in Alexandria and determine its associated factors. This cross-sectional study was performed during the second wave of the COVID-19 pandemic, using a questionnaire assessing COVID-19-related health literacy, adapted from HLS-EU-Q. The work included four phases. The first phase was questionnaire designing and tools used. The second phase included questionnaire filling by participants. The third phase was concerned with increasing population awareness about the COVID-19 pandemic. The fourth phase was the statistical analysis of the data.
Results
The sample compromised 3960 persons. More than half of the Egyptian population living in Alexandria have inadequate or problematic COVID-19-related health literacy scores. Female gender, younger age, higher socioeconomic status, professions with a medical background, and level of education were positively correlated with COVID-19-related health literacy.
Conclusion
COVID-19-related health literacy levels in the Egyptian population living in Alexandria are not sufficient. Policymakers, healthcare providers, and media must act proactively to increase the level of the citizens’ COVID-19-related health literacy and prepare them for other pandemics that may come later.
Similar content being viewed by others


1 Background
Since the first report of the highly contagious and rapidly spreading coronavirus disease (COVID-19) in the city of Wuhan, China, on December 2019, huge information released very rapidly [1,2,3,4]. The media covered the issue around the clock and both official and unofficial websites continuously published recommendations updates and instructions. In these hard times of the pandemic, individuals need to be informed. They need to know what preventive measures they should take and what risky behaviors they should avoid. To avoid the anticipated confusion, coordination of delivered reliable information between the healthcare sector and the media is essential [5].
Control of this highly contagious virus and stopping its transmission requires improving the knowledge and promoting preventive practices of both individuals and communities [6]. Individuals have different degrees of abilities for obtaining and using accurate health information and for proactively responding to critical pandemic times [7,8,9,10].
The European Health Literacy Survey Project (HLS-EU) came up with its definition: “The people’s knowledge, motivation, and competencies to access, understand, appraise, and apply health information to make judgments and take decisions in everyday life concerning health care, disease prevention, and health promotion to maintain or improve quality of life throughout the course of life” [11]. Tools were designed to measure the health literacy [11, 12]. The European Health Literacy Survey Questionnaire (HLS-EU-Q) was developed to measure the health literacy of general populations. However, it does not test a specific patient group but evaluates a more general health knowledge perspective [11].
Health literacy was recognized as a critical health determinant of the health systems [13, 14]. Guidelines for better health literacy were established with many approaches to improve health literacy were adopted. These approaches include screening for low levels of health literacy, determining costs and outcomes of poor health literacy, researching causal pathways of how poor health literacy influences health, and improving low-literacy patients’ health communication [15,16,17].
Advancing COVID-19-related health literacy is not only associated with better self-care, increased autonomy, personal empowerment, more adherence to medications, and improved health outcomes but is also associated with lower health expenditures [18]. Because understanding the pandemic is the first step to mitigating the virus, increasing the level of COVID-19-related health literacy among individuals and information providers about COVID-19 was highly promoted [2, 19,20,21]. This can be addressed by educating the public to become more resourceful, encouraging effective communication of individuals’ needs to health professionals, and understanding health instructions given to them [22,23,24].
Under licensed pharmacist supervision, pharmacy students can deliver health information and increase population awareness [25]. They can improve their social responsibility through the provision of culturally appropriate, updated, and relevant information about COVID-19 to the population and increase COVID-19-related health literacy levels [9, 19, 25, 26].
Notably, health literacy research on COVID-19 infodemic has remained insufficient [9], because scientists often focus on the prevention of disease, not on promoting health literacy of the disease. So, the objective of this study was to assess COVID-19-related health literacy in the Egyptian population living in Alexandria and to increase their awareness about preventing the spread of the COVID-19 virus. Also, to provide evidence-based information to the enrolled participants about the protective measures required to stop the spread of the COVID-19 virus and answer their inquiries about this topic.
1.1 Subjects and methods
1.1.1 Study design
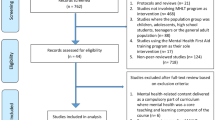
A cross-sectional study. It represents a population-based face-to-face questionnaire on comprehensive health literacy about COVID-19 information and it uses the adapted HLS-EU-Q [27] to assess coronavirus-related health literacy. Each item of the questionnaire was rated on a four-point Likert scale (very difficult, difficult, easy, and very easy). “Very difficult” was scored as 1, “difficult” was scored as 2, “easy” was scored as 3, and “very easy” was scored as 4. Scale values were summed. The questionnaire also tests the individual’s feeling of being informed or confused about COVID-19 by the high flow of information. This study was done in Alexandria, Egypt, during the second wave of the COVID-19 pandemic (Spring 2021) (Fig. 1).

Survey participation flowchart
1.2 First phase: questionnaire designing and tools used
1.2.1 Sociodemographic questions
Participants were asked about their gender, age, education, household monthly income, and occupation (medical versus non-medical background).
1.2.2 Information or confusion about the coronavirus
Two questions were used to address participants’ perceptions of information on COVID-19 derived from a previous study [27]. The first question “Overall, how well the participant’ feels informed about the coronavirus epidemic?”. Responses were rated on a 4-point Likert scale: 1- “not well at all,” 2- “not so well,” 3- “well,” and 4- “very well.” The second question “If the participant feels confused about COVID-19 information?” Responses were rated on a 3-point scale: 1- “yes, very confused,” 2- “yes, somewhat confused,” and 3- “no, barely confused/not confused at all.”
1.2.3 Health literacy assessment and tool used
COVID-19-related health literacy was assessed using the European Health Literacy Survey Questionnaire designed for the COVID-19 pandemic (HLS-COVID-Q22) [27]. This tool measures individuals’ perceived difficulty or ease when accessing, understanding, appraising, and applying health information about the COVID-19 pandemic. The questionnaire is subdivided into four subscales: accessing (six items), understanding (six items), appraising (five items), and applying (five items) COVID-19-related information. Responses range from 1 to 4. The mean of scores is calculated. A mean score of < 2.5 demonstrates inadequate health literacy, a mean score of 2.5–3 demonstrates problematic health literacy, and a mean score of > 3 demonstrates sufficient health literacy [27]. The instrument was translated from English into Arabic by two independent Arabic native speakers, and later back-translated by another translator to establish a version conceptually equivalent to the original one. To validate the draft questionnaire, focus groups were organized via convenience sampling. The sample included five students and two academic staff from the faculty of pharmacy. The retro-translation was found to keep the original ideas and matched the aim of the study. Further validation was done by an independent psychological professor, concerning both relevancy and accuracy regarding the questions understanding by the participants.
1.3 Second phase: questionnaire filling
The survey was done via a questionnaire performed by mid-senior pharmacy students who were enrolled in the obligatory course in pharmacy programs bachelor's in the spring of 2020–2021 under the supervision of the researcher. Each student gave the questionnaire to 10 face-to-face participants by convenience sampling. The participants were included from the adult Egyptian population living in Alexandria. The median time taken to complete every questionnaire was around 12 min.
1.4 Third phase: increasing population awareness about the COVID-19 pandemic
The pharmacy students informed the enrolled participants about the COVID-19 pandemic. They focused on the virus, mode of spread, complications, and the right measures for protection. In addition, they answered any inquiries of participants and differentiated between myths and facts based on up-to-date evidence-based literature.
1.5 Fourth phase: statistical analysis of the data
Data were fed to a Google Form, doublechecked, and analyzed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp). Mean scores, standard deviation, and relative frequencies were reported for COVID-19-related health literacy levels and the different sociodemographic factors, including age, gender, education, monthly income, and profession (medical vs. non-medical background). The Kolmogorov–Smirnov was used to verify the normality of the distribution of variables. Comparisons between categorical variables were assessed using the Chi-square test. Mann–Whitney test was used to compare two categories for not normally distributed quantitative variables. Kruskal–Wallis test was used to compare different categories for abnormally distributed quantitative variables. The significance of the obtained results was judged at the 1% level.
2 Results
A cross-sectional study was conducted in March–April 2021 in Alexandria, Egypt. The sample compromised 3960 persons; out of 6340 contacted with a response rate of 62.4%. The sample compromised of 40.9% females and 59.1% males (Table 1). The majority of the participants questioned were 16–29 years old. About eighty-one percent of the participants reported a household income of less than 29 US dollars, while 18.4% had an income of at least 294 US dollars per month. Education was divided into four categories: 4.4% were illiterate, 9.6% were literate (can read and write), 21% had school education, and 65.2% had high school education (university degree or postgraduate degree) (Table 1).
While most tasks addressed by the questionnaire are easy for most respondents (mean score close to 3, it was easiest to “understand doctor’s, pharmacist’s or nurse’s instructions on protective measures against coronavirus infection?” (mean = 3.07) and “find information about the coronavirus on the internet television/radio/magazines and newspapers?” (mean = 3.06) (Table 2).
On the contrary, the most difficult tasks were to “judge if you have been infected with coronavirus” (mean = 2.51),” Judge how much I am at risk for a coronavirus infection?” (mean = 2.6), and “Judge if the information on the coronavirus and the coronavirus epidemic in the media is reliable?” (mean = 2.66) (Table 2). A total of 17.2%% of participants were found to have “inadequate health literacy,” 40.0% had “problematic health literacy,” and 42.7% had “sufficient health literacy” (Table 3).
“Sufficient” levels of COVID-19-related health literacy were significantly more prevalent (76.2%) among those who felt “very well informed” about the coronavirus compared to not well at all or not so well or well informed about the coronavirus. (p < 0.001). Similarly, “sufficient” levels of COVID-19-related health literacy were significantly more prevalent (75.1%) among those who felt not confused at all (Table 4).
Health literacy levels related to COVID-19 were significantly higher in females (Table 4). Younger participants (18–29 years) were significantly more likely to have “sufficient” levels of COVID-19-related health literacy (46.9%) (Table 4). “Sufficient” levels of COVID-19-related health literacy were significantly more prevalent (51.0%) among those who hold bachelor's, master's, or doctorate degrees (Table 4). “Sufficient” health literacy levels related to COVID-19 were significantly higher (68.4%) in participants with a monthly household income of ≥ 2941 US dollars (Table 4). Individuals of professions with medical backgrounds had higher COVID-19-related health literacy scores (63.7%) (Table 4).
3 Discussion
In a desperate attempt to hinder the further spread of the COVID-19 virus and flatten the peak, governments have adopted strict strategies. Social media and the internet rapidly and drastically spread information about COVID-19. However, a significant proportion of this information is false and misleading [28]. Infodemic, the term developed to describe this “information epidemic,” refers to the great and rapid spread of vast amounts of accurate and inaccurate information on the internet and/or social media [10]. Although the term infodemic was first known during the SARS outbreak in 2003, it wasn’t much used in scientific literature until the COVID-19 pandemic era.
The European Health Literacy Survey (HLS-EU-Q) COVID-19 modified questionnaire measures health literacy in terms of accessing, understanding, appraising, and applying the information related to COVID-19 pandemic [27]. Limited health literacy, including problematic and inadequate health literacy, is a worldwide problem [29,30,31]. About 40% of our participants had problematic COVID-19-related health literacy scores, while 17.2% of our participants had inadequate COVID-19-related health literacy scores. In a previous study, the majority of participants were found to have a limited level of health literacy (inadequate and problematic) [32]. About 42.7% of our participants had sufficient COVID-19-related health literacy scores. Some previous studies showed adequate to good knowledge and practice about COVID-19 among most of the participants [33, 34].
About 54.6% of our participants reported that it is easy for them to find information on the internet, in magazines, and in newspapers about protective behaviors that can help to prevent infection with the coronavirus. Individuals with low levels of health literacy are less likely to take care of their own health [11]. They have difficulties understanding their diseases and medications which may lead to a negative impact on their health [35,36,37,38]. Adequate health literacy is required to face the COVID-19 pandemic. Health literacy about COVID-19 not only enables individuals to use accurate health information but also educates them about the implementation of preventive strategies.
Gender was previously reported to have a major impact on health literacy. The scores of COVID-19-related health literacy scores of women were higher than those of men in this work, in line with some previous studies [33, 34, 39,40,41]. A survey conducted in China showed females were more likely to adopt COVID-19 preventive behavior. They reported that females tended to wear masks and not to visit crowded places more than males [34]. This may be because women are more likely than men to seek online health information as they care for the health of their families including children and elderly people [42]. On the other hand, men scored higher than women in other previous health literacy studies [43,44,45]. However, two previous studies reported no statistically significant difference in health literacy scores between males and females [29, 46].
The socioeconomic status of the individual is another factor that may affect health literacy [43, 44, 47]. A significant positive relationship was found in this work between monthly household income and COVID-19-related health literacy, where the higher the monthly household income, the higher the individual's COVID-19-related health literacy score. Similar results were reported in previous studies [30, 48, 49]. Noteworthy, health literacy for low-income mothers was promoted previously as an empowerment tool [50]. The high cost of hand sanitizers was reported in a previous study to be associated with poor practice due to limited access [51]. Unavailability and high prices of these items and the belief of citizens that they may not be effective due to their lack of awareness can hinder the preventive practice against the COVID-19 virus. The government should provide the required disinfectants and other materials at affordable prices to its citizens to reduce the transmission of the COVID-19 virus.
It was previously suggested that employment is a predictor of better health literacy [51]. Being unemployed was associated with inadequate knowledge about COVID-19, previously [33, 34]. Significantly greater knowledge about COVID-19 and MERS-CoV existed among people who worked as healthcare professionals [33, 40]. In this work, individuals of professions with medical backgrounds had a significantly higher COVID-19-related health literacy score.
Academic institutions provided pharmacists with professional education on online platforms in a previous Egyptian study [52]. However, published literature on knowledge and attitudes about MERS-CoV among health care professionals demonstrated limited knowledge in the southern region of Saudi Arabia [53, 54]. Moreover, a previous study reported that the biology teacher candidates' COVID-19 literacy levels were low to moderate [55].
The level of education can affect health literacy. This study found a significant positive correlation between education level and COVID-19-related health literacy. In this work, individuals with university or post-graduate degrees were found to have the highest COVID-19 health literacy levels. A previous survey on the health literacy of university students during the COVID-19 pandemic showed that two-thirds of university students had low to moderate COVID-19 health literacy levels, while an only 18.45% had a high level of COVID-19 health literacy [56]. On the other hand, other studies reported that education was not a significant predictor of health literacy level [33, 34, 41, 48].
In this work, a significant negative correlation was observed between age and COVID-19-related health literacy, where the older the person is, the lower his/her COVID-19-related health literacy level is. On the other hand, health literacy was reported to be positively correlated with age, but only up to age 65 [41, 57]. This may be caused by the effect of age on cognitive deterioration, which can negatively affect health literacy level [58, 59].
Filtering accurate from inaccurate health information on the internet is a great challenge [60, 61]. Health literacy can enable the general population to identify trustworthy COVID-19 media information and to detect information that might be misleading [62]. Therefore, social media providers must act proactively and spread only accurate health information through the media. Noteworthy, the government should monitor social media platforms and ban false information [63,64,65,66,67,68]. More research is needed on the factors affecting health literacy, how to elevate the health literacy of the population, and the proactive role of pharmacy students in raising the health literacy level of the population and preparedness for what may come later.
To the best of our knowledge, until now, there was no available study on the COVID-19-related health literacy of Egyptian people living in Alexandria. This is the first study to assess COVID-19-related health literacy in this population and its associated factors. In addition, it highlights the role that pharmacy students can play in health promotion because the data published in the literature in this area are scarce. However, it is acknowledged that large sample size may artificially inflate the statistical results. Further research with a smaller number of participants will be required to confirm the results of this work. In addition, this work was done in Alexandria, Egypt, and the results cannot be generalized to the world population. We relied on pharmacy students to collect the data under the supervision of the researcher, as the researcher's time was insufficient to complete the study in a timely fashion.
4 Conclusion
There is a great need to promote health education. More than half of the Egyptian population living in Alexandria has inadequate or problematic COVID-19-related health literacy scores. Female gender, younger age, higher socioeconomic status, professions with a medical background, and level of education were positively correlated with COVID-19-related health literacy. The government, policymakers, healthcare providers, and media must act proactively to increase the level of the citizen's COVID-19-related health literacy. Raising health awareness will protect the population against what may come later.
Availability of data and materials
All data will be available when request.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- HL:
-
Health literacy
- HLS-EU:
-
The European Health Literacy Survey Project
- HLS-EU-Q:
-
The European Health Literacy Survey Questionnaire
- HLS-COVID-Q22:
-
Literacy Survey Questionnaire designed for the COVID-19 pandemic
- MERS-CoV:
-
Middle East Respiratory Syndrome Coronavirus
- US:
-
United States
References
Ashrafi-rizi H, Kazempour Z (2020) Information typology in coronavirus (COVID-19) Crisis; a commentary. Arch Acad Emerg Med 8(1):e19
Ashrafi-rizi H, Kazempour Z (2020) Information diet in Covid-19 crisis; a commentary. Arch Acad Emerg Med 8(1):e30
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA 323(13):1239–1242. https://doi.org/10.1001/jama.2020.2648
Xiang YT, Yang Y, Li W et al (2020) Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 7(3):228–229. https://doi.org/10.1016/S2215-0366(20)30046-8
Smith JA, Judd J (2020) COVID-19: Vulnerability and the power of privilege in a pandemic. Health Promot J Austr 31(2):158–160. https://doi.org/10.1002/hpja.333
Javanian M, Masrour-roudsari J, Bayani M, Ebrahimpour S (2020) Coronavirus disease 2019 (COVID-19): what we need to know. Casp J Intern Med 11(2):235–236. https://doi.org/10.22088/cjim.11.2.235
Nguyen HC, Nguyen MH, Do BN et al (2020) People with suspected COVID-19 symptoms were more likely depressed and had lower health-related quality of life: the potential benefit of health literacy. J Clin Med 9(4):E965. https://doi.org/10.3390/jcm9040965
Nguyen HT, Do BN, Pham KM et al (2020) Fear of COVID-19 scale-associations of its scores with health literacy and health-related behaviors among medical students. Int J Environ Res Public Health 17(11):E4164. https://doi.org/10.3390/ijerph17114164
Paakkari L, Okan O (2020) COVID-19: health literacy is an underestimated problem. Lancet Public Health 5(5):e249–e250. https://doi.org/10.1016/S2468-2667(20)30086-4
Zarocostas J (2020) How to fight an infodemic. The Lancet 395(10225):676. https://doi.org/10.1016/S0140-6736(20)30461-X
Sorensen K, van den Broucke S, Fullam J et al (2012) (HLS-EU) Consortium Health Literacy Project European health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health 25(12):80. https://doi.org/10.1186/1471-2458-12-80
Pleasant A, McKinney J (2011) Coming to consensus on health literacy measurement: an online discussion and consensus-gauging process. Nurs Outlook 59(2):95-106.e1. https://doi.org/10.1016/j.outlook.2010.12.006
Duong TV, Chang PW, Yang SH et al (2017) A new comprehensive short-form health literacy survey tool for patients in general. Asian Nurs Res 11(1):30–35. https://doi.org/10.1016/j.anr.2017.02.001
Watson R (2011) Europeans with poor “health literacy” are heavy users of health services. BMJ 343:d7741. https://doi.org/10.1136/bmj.d7741
Parker RM, Williams MV, Weiss BD, Baker DW, Davis TC, Doak CC, Dickinson BD (1999) Health literacy-report of the council on scientific affairs. JAMA 281(6):552–557
Lloyd LLJ, Ammary NJ, Epstein LG, Johnson R, Rhee K (2006) A transdisciplinary approach to improve health literacy and reduce disparities. Health Promot Pract 7(3):331–335. https://doi.org/10.1177/1524839906289378
McCray AT (2005) Promoting health literacy. J Am Med Inform Assoc JAMIA 12(2):152–163. https://doi.org/10.1197/jamia.M1687
Eichler K, Wieser S, Brügger U (2009) The costs of limited health literacy: a systematic review. Int J Public Health 54(5):313–324. https://doi.org/10.1007/s00038-009-0058-2
Okan SK, Messer (2021) Covid-19: a guide to good practice on keeping people well informed. Parent. https://www.news24.com/parent/family/health/covid-19-a-guide-to-good-practice-on-keeping-people-well-informed-20200408. Published 2020. Accessed September 10, 2021.
Sentell T, Vamos S, Okan O (2020) Interdisciplinary perspectives on health literacy research around the world: more important than ever in a time of COVID-19. Int J Environ Res Public Health 17(9):3010. https://doi.org/10.3390/ijerph17093010
Van den Broucke S (2020) Why health promotion matters to the COVID-19 pandemic, and vice versa. Health Promot Int 35(2):181–186. https://doi.org/10.1093/heapro/daaa042
Peerson & Saunders (2021) Health literacy revisited: what do we mean and why does it matter? Health Promotion International | Oxford Academic. Health Promot Int. Published online 2009. Accessed September 10, 2021. https://academic.oup.com/heapro/article/24/3/285/652750
Schyve (2021) Language differences as a barrier to quality and safety in health care: the joint commission perspective. J Gen Intern Med. Published online 2007. Accessed September 10, 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2078554/
Seng JJB, Yeam CT, Huang CW, Tan NC, Low LL (2020) Pandemic related health literacy – a systematic review of literature in COVID-19, SARS and MERS pandemics. Singapore Med J. https://doi.org/10.1101/2020.05.07.20094227
Chew C, Kapanen A, Gobis B, Reardon J (2021) Pharmacy students’ perspectives on involvement in workplace-based preventative health and wellness events. Curr Pharm Teach Learn 13(6):699–704. https://doi.org/10.1016/j.cptl.2021.01.038
Hernández-García I, Giménez-Júlvez T (2020) Assessment of health information about COVID-19 prevention on the internet: infodemiological study. JMIR Public Health Surveill 6(2):e18717. https://doi.org/10.2196/18717
Okan O, Bollweg TM, Berens EM, Hurrelmann K, Bauer U, Schaeffer D (2020) Coronavirus-related health literacy: a cross-sectional study in adults during the COVID-19 infodemic in Germany. Int J Environ Res Public Health 17(15):5503. https://doi.org/10.3390/ijerph17155503
Spring H (2020) Health literacy and COVID-19. Health Inf Libr J 37(3):171–172. https://doi.org/10.1111/hir.12322
Gustafsdottir SS, Sigurdardottir AK, Arnadottir SA, Heimisson GT, Mårtensson L (2020) Translation and cross-cultural adaptation of the European Health Literacy Survey Questionnaire, HLS-EU-Q16: the Icelandic version. BMC Public Health 20(1):1–11
Sørensen K, Pelikan JM, Röthlin F et al (2015) Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health 25(6):1053–1058. https://doi.org/10.1093/eurpub/ckv043
Svendsen MT, Bak CK, Sørensen K et al (2020) Associations of health literacy with socioeconomic position, health risk behavior, and health status: a large national population-based survey among Danish adults. BMC Public Health 20(1):565. https://doi.org/10.1186/s12889-020-08498-8
Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, Rudd RR (2005) The prevalence of limited health literacy. J Gen Intern Med 20(2):175–184. https://doi.org/10.1111/j.1525-1497.2005.40245.x
Heydari MR, Joulaei H, Zarei N, Fararouei M, Gheibi Z (2021) An online investigation of knowledge and preventive practices in regard to COVID-19 in Iran. Health Lit Res Pract 5(1):e15–e23. https://doi.org/10.3928/24748307-20201130-01
Zhong BL, Luo W, Li HM et al (2020) Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci 16(10):1745–1752. https://doi.org/10.7150/ijbs.45221
Duong VT, Lin IF, Sorensen K et al (2015) Health literacy in Taiwan: a population-based study. Asia Pac J Public Health 27(8):871–880. https://doi.org/10.1177/1010539515607962
Lee SYD, Tsai TI, Tsai YW, Kuo KN (2010) Health literacy, health status, and healthcare utilization of Taiwanese adults: results from a national survey. BMC Public Health 10(1):1–8. https://doi.org/10.1186/1471-2458-10-614
Nutbeam D (2008) (2008) The evolving concept of health literacy. Soc Sci Med 67(12):2072–2078. https://doi.org/10.1016/j.socscimed.2008.09.050
Wolf MS, Davis TC, Tilson HH, Bass PF, Parker RM (2006) Misunderstanding of prescription drug warning labels among patients with low literacy. Am J Health-Syst Pharm 63(11):1048–1055. https://doi.org/10.2146/ajhp050469
Almaleh R, Helmy Y, Farhat E, Hasan H, Abdelhafez A (2017) Assessment of health literacy among outpatient clinics attendees at Ain Shams University Hospitals, Egypt: a cross-sectional study. Public Health 151:137–145. https://doi.org/10.1016/j.puhe.2017.06.024
Asaad A, El-Sokkary R, Alzamanan M, El-Shafei M (2020) Knowledge and attitudes towards Middle East respiratory sydrome-coronavirus (MERS-CoV) among health care workers in south-western Saudi Arabia. East Mediterr Health J Rev Sante Mediterr Orient Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit 26(4):435–442. https://doi.org/10.26719/emhj.19.079
Bas-Sarmiento P, Poza-Méndez M, Fernández-Gutiérrez M, González-Caballero JL, Falcón RM (2020) Psychometric Assessment of the European Health Literacy Survey Questionnaire (HLS-EU-Q16) for Arabic/French-Speaking Migrants in Southern Europe. Int J Environ Res Public Health 17(21):8181. https://doi.org/10.3390/ijerph17218181
Bidmon S, Terlutter R (2015) Gender differences in searching for health information on the internet and the virtual patient-physician relationship in Germany: exploratory results on how men and women differ and why. J Med Internet Res 17(6):e156. https://doi.org/10.2196/jmir.4127
Amoah PA (2018) Social participation, health literacy, and health and well-being: a cross-sectional study in Ghana. SSM - Popul Health 4:263–270. https://doi.org/10.1016/j.ssmph.2018.02.005
Niedorys B, Chrzan-Rodak A, Ślusarska B (2020) Health literacy – a review of research using the European Health Literacy Questionnaire (HLS-EU-Q16) in 2010–2018. Pielegniarstwo XXI Wieku Nurs 21st Century. 19(1):29–41
Tiller D, Herzog B, Kluttig A, Haerting J (2015) Health literacy in an urban elderly East-German population–results from the population-based CARLA study. BMC Public Health 15(1):1–9
Lorini C, Lastrucci V, Mantwill S, Vettori V, Bonaccorsi G, Florence Health Literacy Research Group (2019) Measuring health literacy in Italy: a validation study of the HLS-EU-Q16 and of the HLS-EU-Q6 in Italian language, conducted in Florence and its surroundings. Ann Ist Super Sanita 55(1):10–18. https://doi.org/10.4415/ANN_19_01_04
Levin-Zamir D, Baron-Epel OB, Cohen V, Elhayany A (2016) The association of health literacy with health behavior, socioeconomic indicators, and self-assessed health from a national adult survey in Israel. J Health Commun 21(sup2):61–68. https://doi.org/10.1080/10810730.2016.1207115
Rouquette A, Nadot T, Labitrie P et al (2018) Validity and measurement invariance across sex, age, and education level of the French short versions of the European Health Literacy Survey Questionnaire. PLoS ONE 13(12):e0208091. https://doi.org/10.1371/journal.pone.0208091
Sundquist J (2001) Migration, equality and access to health care services. J Epidemiol Commun Health 55(10):691–692. https://doi.org/10.1136/jech.55.10.691
Porr C, Drummond J, Richter S (2006) Health literacy as an empowerment tool for low-income mothers. Fam Commun Health 29(4):328–335. https://doi.org/10.1097/00003727-200610000-00011
Machmud A, Minghat ADB (2020) The price dynamics of hand sanitizers for COVID-19 in Indonesia: exponential and cobweb forms. Indones J Sci Technol 5(2):176–184. https://doi.org/10.17509/ijost.v5i2.24431
Kassem AB, Ghoneim AI, Nounou MI, El-Bassiouny NA (2021) Community pharmacists’ needs, education, and readiness in facing COVID-19: actions & recommendations in Egypt. Int J Clin Pract. https://doi.org/10.1111/ijcp.14762
Abbag HF, El-Mekki AA, Al Bshabshe AAA et al (2018) Knowledge and attitude towards the Middle East respiratory syndrome coronavirus among healthcare personnel in the southern region of Saudi Arabia. J Infect Public Health 11(5):720–722. https://doi.org/10.1016/j.jiph.2018.02.001
Alsahafi AJ, Cheng AC (2016) Knowledge, attitudes and behaviours of healthcare workers in the Kingdom of Saudi Arabia to MERS coronavirus and other emerging infectious diseases. Int J Environ Res Public Health 13(12):1214. https://doi.org/10.3390/ijerph13121214
Fauzi A, Husamah H, Miharja FJ, Fatmawati D, Permana TI, Hudha AM (2020) Exploring COVID-19 literacy level among biology teacher candidates. Eurasia J Math Sci Technol Educ. https://doi.org/10.29333/ejmste/8270
Shaukat R, Naveed MA (2021) Health literacy of university students in Covid-19 pandemic and infodemic: a Pakistani perspective. Libr Philos Pract E-J. Published online January 1, https://digitalcommons.unl.edu/libphilprac/4708
Nakayama K, Osaka W, Togari T, et al (2021) Comprehensive health literacy in Japan is lower than in Europe: a validated Japanese-language assessment of health literacy. BMC Public Health. 2015;15(1). Accessed September 10, 2021. https://www.academia.edu/34639493/Comprehensive_health_literacy_in_Japan_is_lower_than_in_Europe_a_validated_Japanese_language_assessment_of_health_literacy
Baker DW, Gazmararian JA, Sudano J, Patterson M (2000) The association between age and health literacy among elderly persons. J Gerontol B Psychol Sci Soc Sci 55(6):S368-374. https://doi.org/10.1093/geronb/55.6.s368
Kaphingst KA, Goodman MS, MacMillan WD, Carpenter CR, Griffey RT (2014) Effect of cognitive dysfunction on the relationship between age and health literacy. Patient Educ Couns 95(2):218–225. https://doi.org/10.1016/j.pec.2014.02.005
Cuan-Baltazar JY, Muñoz-Perez MJ, Robledo-Vega C, Pérez-Zepeda MF, Soto-Vega E (2020) Misinformation of COVID-19 on the internet: infodemiology study. JMIR Public Health Surveill 6(2):e18444. https://doi.org/10.2196/18444
Eysenbach G, Powell J, Kuss O, Sa ER (2002) Empirical studies assessing the quality of health information for consumers on the world wide web: a systematic review. JAMA 287(20):2691–2700. https://doi.org/10.1001/jama.287.20.2691
Abel T, McQueen D (2020) Critical health literacy and the COVID-19 crisis. Health Promot Int 35(6):1612–1613. https://doi.org/10.1093/heapro/daaa040
Cinelli M, Quattrociocchi W, Galeazzi A et al (2020) The COVID-19 social media infodemic. Sci Rep 10(1):16598. https://doi.org/10.1038/s41598-020-73510-5
Hua J, Shaw R (2020) Corona virus (COVID-19) “infodemic” and emerging issues through a data lens: the case of China. Int J Environ Res Public Health 17(7):E2309. https://doi.org/10.3390/ijerph17072309
Luengo-Oroz M, Hoffmann Pham K, Bullock J et al (2020) Artificial intelligence cooperation to support the global response to COVID-19. Nat Mach Intell 2(6):295–297. https://doi.org/10.1038/s42256-020-0184-3
Medford RJ, Saleh SN, Sumarsono A, Perl TM, Lehmann CU (2019) An “infodemic”: leveraging high-volume twitter data to understand early public sentiment for the Coronavirus disease outbreak. Open Forum Infect Dis. https://doi.org/10.1093/ofid/ofaa258
Merchant RM, Lurie N (2020) Social media and emergency preparedness in response to novel coronavirus. JAMA 323(20):2011–2012. https://doi.org/10.1001/jama.2020.4469
Vaezi A, Javanmard SH (2020) Infodemic and risk communication in the era of CoV-19. Adv Biomed Res 9:10. https://doi.org/10.4103/abr.abr_47_20
Acknowledgements
We would like to thank students in the course of PN 407 – Pharmaceutical care II (spring 2020-2021) in the faculty of pharmacy, Pharos University in Alexandria, Egypt, for collecting the data. We also would like to thank the following teaching assistants’ team at the department of clinical pharmacy and pharmacy practice for helping and guiding the students during data collection phase: Hala Abu-El Hassan, Zeyad Beshara, Hadeer El Sayed, Rana Sharkawy, Alyaa Ahmed, and Nourhan Gamal.
Funding
The manuscript did not receive any pharmaceutical or industrial support.
Author information
Authors and Affiliations
Contributions
HA conceived of the presented idea. ABK and HA developed the theory and performed the statistics. HA contributed to the interpretation of the results. Both ABK and HA involved in writing the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript. All authors discussed the results and contributed to the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by the ethics committee of the faculty of pharmacy, Pharos university in Alexandria, Egypt (Study number: PUA01202106203024). All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration. Participation in the study was voluntary. The participants were informed that the data obtained would be used for research purposes only and data obtained were confidentially analyzed. Informed consent was then obtained from all individuals included in the study.
Consent for publication
Not applicable.
Competing interests
They authors declare no conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Moustafa, H.A.M., Kassem, A.B. COVID-19-related health literacy and preparedness to what may come: a cross-sectional study. Beni-Suef Univ J Basic Appl Sci 12, 114 (2023). https://doi.org/10.1186/s43088-023-00452-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43088-023-00452-y