
Abstract
Background
Over the years, air pollution has garnered increased attention from researchers who continue to provide studies and suggestive data that prove there is an ever-increasing risk of air pollution on the health of humans, terrestrial, and aquatic animals. A measurement involved in the quantity of certain traceable particles within the air, namely: Particulate Matter (PM) 2.5 and 10, ozone (O3), Nitrogen dioxide (NO2), sulfur dioxide (SO2), and carbon monoxide (CO) emissions, all converted to Air Quality Index. Most studies are predominantly from developed nations with limited research conducted in developing nations such as those in Latin America and the Caribbean.
Main body
In this systematic review, we examined the impact of air pollution on public health. A database search produced 1,118 studies, of which four were selected for a quantitative meta-analysis that explored hazard ratios concerning exposure to elevated levels of PM2.5. The meta-analysis results show that exposure to PM2.5 increases the risk of an adverse health event by as much as 2% five days after exposure. Results also indicated a consensus on the negative impacts of air pollution on public health. The results also suggest that more can be done within the region to combat or at the very least minimize the impact of air pollution to public health.
Conclusion
The pooled data from the studies reviewed show that there is an increased risk of an adverse health event on the day of exposure to PM2.5 and every subsequent day after exposure. A pattern exists between hospitalization and air pollution due to increased susceptibility to respiratory infections and asthma development. Combating the harmful effects of air pollution should be a top priority in Latin America and the Caribbean.
Similar content being viewed by others


1 Background
The contamination of water, air, and land through the introduction of harmful biological, chemical, and physical agents is termed pollution. Pollution negatively impacts the environment and public health, leading to morbidity and mortality [1]. Lack of awareness of the different forms of pollution, poor policies and legislation, inadequate or lack of enforcement, and poverty generally make the pollution burden greater in developing countries than in developed countries [2]. Although the negative impact of water and land pollution on public health cannot be underrated, the environmental and public health impacts of air pollution are dire, especially in developing countries [3]. Air pollution is defined as an atmospheric condition in which substances are present in the air above normal levels, creating measurable adverse effects, particularly on animals, humans, and vegetation [4]. Air pollution poses a significant risk to the health of the world’s population, with even short-term exposure linked to numerous respiratory diseases and increased hospitalization rates [5]. Additionally, air pollution affects pollution levels in water and soil via precipitation, potentially leading to harmful chemicals present in produce and livestock used for human consumption [6]. In a recent review, Manisalidis et al. [5] highlighted the numerous health effects of air pollution, including respiratory, reproductive, cardiovascular, neurological, and specific cancers. In addition, environmental impacts were reported to include climate change, ozone depletion, haze, acid rain, and heat-related public health issues. Through the depletion of the ozone layer and global warming, the quality of life on Earth is adversely affected by air pollution. Gaseous pollutants such as carbon monoxide (CO), volatile organic compounds (VOCs), nitrogen oxides, and sulfur oxides enter the environment through various means and distributes within the atmosphere. These primary pollutants are released into the environment primarily due to mining, exploration, population growth, urbanization, industrialization, and natural disasters [2]. In addition, solid waste disposal contributes more than 4.2% of the total air pollution, as reported in EPA emission totals [7, 8].
Air pollution is generally measured using particulate matter (PM2.5 and PM10), ozone (O3), nitrogen dioxide (NO2), sulfur dioxide (SO2), and carbon monoxide (CO) emissions and converted to an Air Quality Index (AQI). An AQI of 100 or below is acceptable, with values above 100 ranging from unhealthy for sensitive populations to hazardous. Air pollutants can come from numerous sources, including traffic, industry, and energy production, which places a higher risk of exposure to air pollution in urban areas [9]. Lower- and middle-income countries, which most countries in Latin America and the Caribbean fall into, are experiencing a boom in urbanization, putting additional risk on a population with an already struggling healthcare system. The World Health Organization (WHO) [10] reported that air pollution is associated with increased mortality and morbidity, killing an estimated seven million people worldwide; its increase does not bode well for public health. Within the last decade, numerous research has found substantial data showing air pollution is associated with a broad number of disease outcomes, ultimately leading to premature death from ischemic heart disease, chronic obstructive pulmonary disease (COPD), lung cancer, and acute lower respiratory infections [11]. Recent reviews of COVID-19 data indicates that air pollution may contribute significantly to higher rates of COVID-19 infections and mortality and its transmission [3, 12]. Relatedly, correlations between air pollution, COVID-19, and rheumatic diseases were established and reported [13,14,15]. Cardiovascular and lung diseases and other serious health challenges have also been reported due to air pollutants. People with pre-existing noncommunicable diseases, older adults, pregnant women, children, and persons living in low socioeconomic communities are more vulnerable to air pollution and its attendant negative health impacts [16].
Although many developed and industrialized nations have researched and reported on the impacts of air pollution on public health, within Latin America and the Caribbean, this area has been somewhat underexplored despite the region having over 100 million residents living in areas exposed to air pollution levels exceeding the World Health Organization guidelines [17]. Air pollution places a significant risk to the public's health, from early disease development to premature death, which also increases health-related expenditure and resources. Thus, it is essential for Latin America and the Caribbean to have more and continuing research in this area to influence policy, reduce public health risk, and reallocate resources and expenses to more needed areas. Although studies show links between air pollution and disease in Latin America and the Caribbean, a systematic review of the evidence of air pollution and its effects on public health is lacking.
Using a systematic review methodology, this paper reviewed the impact of air pollution on public health within Latin America and the Caribbean.
2 Main text
2.1 Methodology
Relevant studies were identified through electronic search of Google Scholar, EBSCOHOST, HINARI, Scielo, PubMed, and Scopus databases. Search combined terms included 'air pollution,' 'public health,' 'Latin America,' 'Caribbean,' 'Central America,' and 'South America.' Rayyan systematic review software was used for uploading and sorting study references.
2.2 Risk of bias in individual studies
Two independent reviewers conducted a qualitative assessment on which studies to include and exclude and classify studies as low or high risk of bias to reduce bias (Table 1, Fig. 1). Additionally, publication bias for included studies was assessed using a funnel plot.

Study identification and selection process
2.3 Summary measures
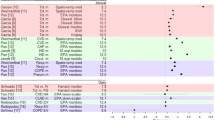
The statistical analysis software, Review Manager 5.4.1, was used to calculate the summary effects of the lag structure (Fig. 2). For analysis, all corresponding lags were grouped for analysis of exposure to PM2.5. Cochrane Q test (significance level: 0.1) and I2 statistic were used to test statistical heterogeneity. I2 statistic quantifies heterogeneity by calculating the proportion of variation that occurred by heterogeneity rather than by chance [18]. For I2, values ranging from 0 to 30, 30 to 50, and > 50 indicated low, moderate, and high heterogeneity, respectively.

Forest plots of hazard ratios A Lag0, B Lag1, C Lag2, D Lag3, E Lag4, F Lag5
3 Results
Database searches produced 1118 studies, of which four were selected for quantitative meta-analysis (Fig. 1). All four studies originated from Brazil and explored exposure to air pollution and its corresponding health risks on the day of exposure and up to at least five days after. Air pollution assessments include CO, O3, NOX, and PM2.5, but only PM2.5 data was used for statistical analysis as it was the only assessment data common among the four studies (Table 2, Fig. 2).
Meta-analysis of the hazard ratios from the day of exposure to PM2.5 shows a 1% increase in the risk of an adverse health event for the day of exposure up to 4 days after exposure, with day 5 showing a 2% increase.
4 Discussion
We conducted a systematic review to explore the impact of air pollution on public health in Latin America and the Caribbean. The aim was to determine if the grouped data expressed the same results and were, for the most part, in consensus with each other. There is an understanding that air pollution negatively impacts health, but does the available data support this assumption, particularly within the Latin American and Caribbean regions?
Using hazard ratios after exposure to PM2.5, the pooled data suggests an increased risk of an adverse health event after exposure to air pollution (Table 2). These findings resonate with studies in developed countries [23]. PM2.5 is fine particulate matter in the air that is less than 2.5 µm in diameter, with the concentrations of PM2.5 being used in calculating the Air Quality Index. PM2.5 has been linked to numerous respiratory issues, as it can penetrate deeply into the lungs and significantly impair lung function [24]. The European Environment Agency (EEA) [25] reported that particulate matter ranks among the top 5 most harmful air pollutants. The pooled data from the four studies showed an increased risk of an adverse health event on the day of exposure to PM2.5 and every subsequent day after exposure (Table 2, Fig. 2). Of note was that the increased risk advanced to 2% on the fifth day after exposure, but with a moderate heterogeneity percentage, suggesting some level of 'uncombinablity' (Table 2, Fig. 2). Despite this, the evidence is still strong in response to the risk associated with exposure to air pollution, showing that the risk exists not only on the day of exposure but can adversely affect public health in the near future.
Furthermore, a pattern was established between hospitalization and air pollution in the four studies evaluated. Using an ecological time-series study, Cesar et al. [20] conducted a study to estimate the association between hospitalization caused by respiratory diseases and air pollutants. By comparing deaths from respiratory diseases and estimated daily levels of air pollutants over an approximate one-year period, their study established an association between exposure to Nitrogen oxides (NOx) and deaths from respiratory diseases. Similarly, the United States Environmental Protection Agency (US-EPA) [16] documented that exposure to NOx, such as NO2, even over short periods, can aggravate respiratory diseases, such as asthma, which leads to increased respiratory symptoms, hospital admission, and emergency room visits. Furthermore, the US-EPA also reported that more prolonged exposure to elevated concentrations of NO2 might contribute to a potential increase in susceptibility to respiratory infections and the development of asthma.
In another ecological time-series study, Nascimento et al. [19] reported that respiratory diseases are influenced by exposure to numerous air pollutants, such as NO2, particulate matter less than PM10, carbon monoxide, and sulfur dioxide, leading to hospitalizations. The study was conducted over one year, with data showing that an increase in PM2.5 concentrations significantly increased the risk of hospitalization due to respiratory diseases such as pneumonia, acute bronchitis, bronchiolitis, and asthma.
Evidence suggests that those with existing respiratory disease conditions are at an increased risk of adverse health effects due to exposure to air pollutants. Machin et al. [21] identified and reported the effects of exposure to fine particulate matter and CO on the number of hospitalizations due to respiratory diseases in the elderly (60 years and older). Their report demonstrated a significant association between exposure to these particles and hospitalizations, with an increased risk of hospitalization of 31.8%. An increased concentration of PM2.5 demonstrated a significant negative impact on respiratory disease exacerbation.
The review results resonate with other studies done worldwide. Slama et al. [26] reported a positive association between ambient air pollution and hospitalization, where PM2.5 and PM10 had the most significant effect. All four studies looked primarily at hospitalization associated with visits for respiratory ailments; however, exposure to particulate matter has other detrimental effects on health. Zhang et al. [27] reported that particulate matter exposure increased hospitalization visits for arrhythmia, high blood pressure, cerebrovascular disease, and ischemic heart disease. This implication to other health-related hospitalizations shows that many individuals with pre-existing health conditions are susceptible to short-term air pollution exposure, increasing public health risk, and public health expenditure, both in the private and public sectors.
The results of this systematic review can help guide policy changes regarding the rise in urbanization within the Caribbean and Latin American regions. However, the review results can also benefit healthcare providers who can educate patients on the health risk of air pollution and implement strategies at the public health level to deal with increases in adverse health events to Unhealthy Air Quality Index levels. Combating the harmful effects of air pollution should be a priority within the LAC region, as it can potentially reduce public health costs by millions in each respective country. An essential first step is to examine available data, which this systematic review provides. Additionally, more studies within the region ought to be done so that additional data can be used to design tailored policies for each country, as what may work for Jamaica may not work for Ecuador.
5 Limitations
Some limitations of this study include a bias risk, as all study data that met the inclusion criteria originated in Brazil. This limitation is partly a result of few regional studies on air pollution and public health, primarily due to the inaccessibility of daily Air Quality Index data. Another limitation is that only PM2.5 was accessed, not the other measurements included in the Air Quality Index. A multivariate analysis would have possibly yielded more robust results, but the researchers were unable to account for the 'uncombinability’ of such a data set. Finally, the various assessment data in each study could not be grouped as one, as the software used could not account for the multivariate nature of such a data set.
6 Conclusion
With a fast rate of development within Latin America and the Caribbean, it is crucial to outline and provide continuous research on the consequences and impact of air pollution on the population of these developing nations. Though there is an overwhelming lack of data and studies on air pollution within the region, the available data revealed a negative impact of air pollution on public health from the day of exposure up to five days after exposure. The 1% increase in the exposure rate to 2% by day 5 is evident in the results of the hazard ratios. Countries within Latin America and the Caribbean need to examine their developmental impacts on air pollution, how it affects public health, and how it can be effectively managed.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- AQI:
-
Air quality index
- CO:
-
Carbon monoxide
- COPD:
-
Chronic obstructive pulmonary disease
- EEA:
-
European Environment Agency
- LAC:
-
Latin America and the Caribbean
- NO2 :
-
Nitrogen dioxide
- NOx :
-
Nitrogen oxides
- O3 :
-
Ozone
- PM:
-
Particulate matter
- SO4 :
-
Sulfur dioxide
- USEPA:
-
United States Environmental Protection Agency
- WHO:
-
World Health Organization
References
Landrigan PJ, Fuller R, Acosta NJR, Adeyi O, Arnold R, Basu N et al (2017) The Lancet Commission on pollution and health. Lancet 391(10119):462512. https://doi.org/10.1016/S0140-6736(17)32345-0
Ukaogo PO, Ewuzie U, Onwuka CV (2020) Environmental pollution: causes, effects, and the remedies. Microorgan Sustain Environ Health. https://doi.org/10.1016/b978-0-12-819001-2.00021-8
Marquès M, Domingo JL (2022) Positive association between outdoor air pollution and the incidence and severity of COVID-19: a review of the recent scientific evidences. Environ Res 203:111930. https://doi.org/10.1016/j.envres.2021.111930
Gordon GE (1987) Atmospheric science: atmospheric chemistry and atmospheric chemistry and physics of Air Pollution. Science 235:4793. https://doi.org/10.1126/science.235.4793.1263b
Manisalidis I, Stavropoulou E, Stavropoulos A, Bezirtzoglou E (2020) Environmental and health impacts of Air Pollution: a Review. Front Public Health. https://doi.org/10.3389/fpubh.2020.00014
Newman JR, Schreiber RK, Novakova E (1992) Air pollution effects on terrestrial and aquatic animals. In: Barker JR, Tingey DT (eds) Air pollution effects on biodiversity. Springer, Boston. https://doi.org/10.1007/978-1-4615-3538-6_10
Kupchik GJ, Franz GJ (1976) Solid waste, air pollution and health. J Air Pollut Control Assoc 26(2):116–118. https://doi.org/10.1080/00022470.1976.10470229
Kebaili FK, Baziz-Berkani A, Aouissi HA, Mihai F-C, Houda M, Ababsa M, Azab M et al (2022) Characterization and planning of household waste management: a case study from the MENA region. Sustainability 14(9):5461. https://doi.org/10.3390/su14095461
Gouveia N, Kephart JL, Dronova I, McClure L, Granados JT, Betancourt RM, O’Ryan AC, Texcalac-Sangrador JL, Martinez-Folgar K, Rodriguez D, Diez-Roux AV (2021) Ambient fine particulate matter in Latin American cities: Levels, population exposure, and associated urban factors. Sci Total Environ 772:145035. https://doi.org/10.1016/j.scitotenv.2021.145035
WHO (2021) Air Pollution. Retrieved February 3, 2022, from https://www.who.int/health-topics/air-pollution#tab=tab_1
Kelly FJ, Fussell JC (2015) Air Pollution and Public Health: emerging Hazards and improved understanding of risk. Environ Geochem Health 37(4):631–649. https://doi.org/10.1007/s10653-015-9720-1
Ali N, Islam F (2020) The effects of air pollution on covid-19 infection and mortality—a review on recent evidence. Front Public Health. https://doi.org/10.3389/fpubh.2020.580057
Misra DP, Agarwal V, Gasparyan AY, Zimba O (2020) Rheumatologists’ perspective on coronavirus disease 19 (COVID-19) and potential therapeutic targets. Clin Rheumatol 39(7):2055–2062. https://doi.org/10.1007/s10067-020-05073-9
Aouissi HA, Belhaouchet I (2021) What about rheumatic diseases and COVID-19? New Microbes New Infect 41:100846. https://doi.org/10.1016/j.nmni.2021.100846
Izadi Z, Gianfrancesco MA, Schmajuk G, Jacobsohn L, Katz P, Rush S, Ja C, Taylor T, Shidara K, Danila MI, Wysham KD, Strangfeld A, COVID-19 Global Rheumatology Alliance Registry (2022) Environmental and societal factors associated with COVID-19-related death in people with rheumatic disease: an observational study. Lancet Rheumatol. https://doi.org/10.1016/S26659913(22)00192-8
US-EPA (2022) Research on Health Effects from Air Pollution. US-EPA. https://www.epa.gov/air-research/research-health-effectsair-pollution#health-effects-vulnerable-pops Accessed 15 May 2022
Riojas-Rodríguez H, Soares da Silva A, Texcalac-Sangrador JL, Moreno-Banda GL (2016) Air pollution management and control in Latin America and the Caribbean: implications for climate change. Rev Panam Salud Publica 40(3):150–159
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560. https://doi.org/10.1136/bmj.327.7414.557
Nascimento LF, Vieira LC, Mantovani KC, Moreira DS (2016) Air pollution and respiratory diseases: ecological Time Series. Sao Paulo Med J 134(4):315–321. https://doi.org/10.1590/1516-3180.2015.0237250216
César AC, Carvalho JA Jr, Nascimento LF (2015) Association between NOX exposure and deaths caused by respiratory diseases in a medium-sized Brazilian city. Braz J Med Biol Res 48(12):1130–1135. https://doi.org/10.1590/1414-431x20154396
Machin AB, Nascimento LF, Mantovani K, Machin EB (2019) Effects of exposure to fine particulate matter in elderly hospitalizations due to respiratory diseases in the south of the Brazilian Amazon. Braz J Med Biol Res. https://doi.org/10.1590/1414-431x20188130
Patto NV, Nascimento LF, Mantovani KC, Vieira LC, Moreira DS (2016) Exposure to fine particulate matter and hospital admissions due to pneumonia: effects on the number of hospital admissions and its costs. Rev Assoc Med Bras 62(4):342–346. https://doi.org/10.1590/1806-9282.62.04.342
Sun Z, Zhu D (2019) Exposure to outdoor air pollution and its human health outcomes: a scoping review. PLoS ONE. https://doi.org/10.1371/journal.pone.0216550
Xing YF, Xu YH, Shi MH, Lian YX (2016) The impact of PM2.5 on the human respiratory system. J Thorac Dis 8(1):E69-74. https://doi.org/10.3978/j.issn.2072-1439.2016.01.19
European Environment Agency (EEA) (2021) European Union emission inventory report 1990–2019: LRTAP 1990 2019. European Environment Agency. https://www.eea.europa.eu/publications/lrtap-1990-2019 Accessed 13 May 2022
Slama A, Śliwczyński A, Woźnica J, Zdrolik M, Wiśnicki B, Kubajek J, Turżańska-Wieczorek O, Gozdowski D, Wierzba W, Franek E (2019) Impact of air pollution on hospital admissions with a focus on respiratory diseases: a Time-series multi-city analysis. Environ Sci Pollut Res 26(17):16998–17009. https://doi.org/10.1007/s11356-019-04781-3
Zhang Y, Ma Y, Feng F, Cheng B, Wang H, Shen J, Jiao H (2021) Association between PM10 and specific circulatory system diseases in China. Sci Rep. https://doi.org/10.1038/s41598-021-91637-x
Acknowledgments
Not applicable.
Funding
No funding was received in regards to this review or its publication.
Author information
Authors and Affiliations
Contributions
DCH conceptualized the study, provided supervision, reviewed, edited, and finalized the final draft. KR and DB conducted literature search and data analysis and wrote the first draft. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Husaini, D.C., Reneau, K. & Balam, D. Air pollution and public health in Latin America and the Caribbean (LAC): a systematic review with meta-analysis. Beni-Suef Univ J Basic Appl Sci 11, 122 (2022). https://doi.org/10.1186/s43088-022-00305-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43088-022-00305-0