
Abstract
Background
Acute liver failure (ALF) is a serious condition that refers to the development of synthetic function impairment after severe acute liver injury in an individual without pre-existing liver disease. Understanding the epidemiology of ALF in children constitutes a cornerstone in its preventive and treatment plans. Nevertheless, there is a lack of information about its epidemiology in Egypt.
Objective
The aim of this study was to assess the epidemiologic data of ALF in Egyptian children.
Patients and methods
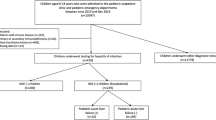
The medical records of children with ALF aged from 6 months to 18 years who were admitted from 2015 to 2020 were analyzed to identify the patient’s epidemiologic, laboratory, and investigational data together with their outcome.
Results
The study included 154 patients who fulfilled the definition of ALF were included. Their age ranged from 7 months to 17 years, with a median of 5.8 years. Hepatitis A virus (HAV) was the most commonly identifiable etiology (37.7%). Mortality was the outcome for 73 patients (47.4%). The prognostic factors associated with mortality were elevated international normalized ratio (INR), total bilirubin (TB), creatinine, and ammonia levels at presentation with cutoff values (2.97, 21.15, 0.385, and 212, respectively).
Conclusion
Hepatitis A virus is the most commonly identified etiology of ALF in Egyptian children. The mortality rate is high, and most of the deaths occurred early in the first 5 days of admission. So, early preparation for liver transplantation is recommended. Higher values of INR, TB, and creatinine above the cutoff levels at presentation may be potential markers for predicting death in affected children.
Similar content being viewed by others

Introduction
Acute liver failure (ALF) is a life-threatening morbidity. The Pediatric Acute Liver Failure (PALF) study group defines ALF in pediatrics as clinical and laboratory evidence of severe liver dysfunction in a child with unknown evidence of chronic liver disease. It is characterized biochemically by hepatic-based coagulopathy, with a prothrombin time (PT) ≥ 20 s or international normalized ratio (INR) ≥ 2 not corrected by vitamin K administration irrespective of the presence or absence of hepatic encephalopathy (HE), or a PT ≥ 15 s or INR ≥ 1.5 not corrected by vitamin K administration in the presence of HE [1].
Epidemiology is the study of the distribution (frequency, pattern) and explanatory factors (causes, risk factors) of health-related states and events (health outcomes) in specified populations at a particular time. Health outcomes are the main focus of epidemiological research [2].
The overall incidence of ALF in children is unknown. In the United States of America (USA), there were no significant regional variations in the incidence of ALF in children, the type of liver transplant, or outcomes [3].
The etiology of ALF plays an important role in the management and survival of patients. Specific etiologies of ALF in pediatrics can be broadly categorized as infectious, immunologic, metabolic, vascular, and toxin- or drug-related [4].
The etiology of ALF varies according to the age of patients and the development of the country. In the first year of life, metabolic and infectious diseases are prevalent, and in adolescence, Wilson disease (WD) and acetaminophen overdose are common [5]. In resource-rich countries, drug-induced ALF is usually the most common etiology in children, while in resource-limited countries, infectious etiologies are dominant, among which hepatitis A virus (HAV) is the most common [6].
Acute liver failure can lead to many devastating complications, such as sepsis, coagulopathy, cerebral edema, renal and/or respiratory failure, hemodynamic instability, and aplastic anemia [7]. Cerebral edema and multiple organ dysfunction syndromes are the two major leading causes of death [8].
Management of ALF in pediatrics requires a multidisciplinary approach and is directed at establishing the etiology, monitoring, and managing the multisystem complications that usually occur [9]. A high index of suspicion, early referral to a liver transplantation (LT) center, and adequate supportive management remain the cornerstones for the management [10].
Patients and methods
Study population
The study was conducted on all children who fulfilled the PALF study group definition [1] within the age from 6 months up to 18 years who were admitted between January 2015 and December 2020. Patients below 6 months were excluded as the mechanism and etiology of ALF are different. Neonatal acute liver failure begins at a different liver starting point than ALF or PALF. In those 2 conditions, the starting point is a developed and functioning liver to which an insult is applied, resulting in liver failure, whereas, in neonatal acute liver failure the insult may have been applied in fetal life before the liver has developed and had a chance to function normally [11]. All procedures were performed in compliance with relevant laws and institutional guidelines and have been approved by the Institutional Review Board of the National Liver Institute (NLI-IRB 00003413 FWA0000227), Menoufia University (approval number: 00435). Informed consent was obtained from the patient’s guardians before starting the study.
There were 154 children diagnosed with ALF whose medical charts were analyzed, recording their demographic and clinical data, grades of HE, and laboratory parameters. The studied patients were categorized according to their outcome into two groups: the deceased group (47.4%) and the recovered group (52.6%).
Data of the recruited cases were retrieved from the inpatient and outpatient files and included descriptive data (age, sex, and consanguinity), time (seasonality), and place. According to age, patients were categorized into early infancy (6 months to 1 year), toddlers (> 1–3 years), preschool (> 3–6 years), school age (> 6–12 years), and adolescence (> 12–18 years). The geographic distribution was studied in Egypt’s regional units. Egypt is divided into five regions as follows: the Greater Cairo region, the Alexandria region, the Delta region, the Suez Canal region, and the Upper Egypt region.
Analytical data (laboratory and radiological investigations) was concerned with reporting the etiology, predisposing factors, frequency, and mortality rate of the disease.
Fulminant Wilson was diagnosed by normal or low serum alkaline phosphatase, high bilirubin to alkaline phosphatase ratio, low serum ceruloplasmin levels, Kayser-Fleischer rings seen by slit-lamp examination, serum copper, 24-h urinary copper excretion before and after challenge with D-penicillamine, neuropsychiatric disturbances, and acute episodes of Coombs-negative hemolysis [4].
The indeterminate etiology was recorded after exclusion of the routine basic diagnostic screen including blood, urine and stool cultures, viral markers and PCR of hepatotropic viruses, autoantibodies (ANA, anti-SMA, and anti-LKM-1), serum total IgG, and metabolic screening using extended metabolic screen and urinary organic acids. Since the start of COVID-19 outbreaks, CoV2 was also excluded by RT-PCR testing. Undiagnosed patients were labeled as early death interfered with completing the diagnostic workup.
Statistical analysis
Quantitative data were presented as mean ± standard deviation (SD) or median (minimum–maximum), while qualitative data were presented as frequency and percentage. For both normally distributed and not normally distributed quantitative data, significance was tested by either the Student t-test or the Mann-Whitney U test, respectively. The chi-square test, or Fisher’s exact test, was used for the measurement of the qualitative data association. Significance was set at a p value < 0.05.
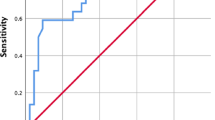
A receiver operating characteristic (ROC) curve was done for statistically significant variables to identify the cutoff values that can be used as predictors for the risk of mortality in the studied patients. Sensitivity, specificity, positive and negative predictive values, and diagnostic accuracy were calculated. Statistical analysis was performed using (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. Released 2013).
Results
The current study included 154 (2.3%) children diagnosed with ALF out of 6453 patients admitted within the study duration. Their age ranged between 0.6 and 17 years and 54.5% were males (Table 1).
The recovered group and deceased group were comparable for baseline clinical and laboratory characteristics at presentation. The timing of death for 63% of the deceased group occurred within the first 5 days of admission.
Regarding clinical findings, all patients had jaundice at presentation. Hepatomegaly and splenomegaly were found in 53.9% and 50.6% of patients, respectively, while ascites was detected in about 41.6%.
Most of the studied patients were from the Delta Region (n = 60 patients), followed by the Greater Cairo Region (n = 47 patients) (Fig. 1). ALF was more frequent in winter, followed by autumn and spring (29%, 26%, and 25%, respectively). There was no significant association between seasonality or geographical distribution and the patient’s outcome.

Comparison between deceased and recovered groups according to geographic distribution in regional units of Egypt: there was no significant association between geographical distribution and the patient’s outcome
The most commonly identified etiology was HAV (37.7%), followed by indeterminate hepatitis (33.8%) (Fig. 2). ALF etiologies were significantly associated with the outcome (p-value 0.002). Survival was 100% for cytomegalovirus (CMV) and 87.5% for autoimmune hepatitis (AIH). On the other hand, mortality was 92.86% for the undiagnosed, 75% for WD, 66.7% for shock liver and drug-induced ALF, and 43.1% for HAV.

Etiology of acute liver failure: the most commonly identified etiology of pediatric ALF was HAV (37.7%), followed by indeterminate hepatitis (33.8%)
There was a statistically significant difference among different etiologies of ALF according to age (p-value < 0.001). Shock liver was detected more frequently in the youngest age group, while WD was detected more frequently in adolescence (Fig. 3). HAV was the most common etiology in preschool age (3–6 years) and toddler age (1–3 years) (61.5% and 37.5%, respectively).

Age distribution among different etiologies of ALF. The box-and-whisker plot shows the etiology of acute liver failure according to age: Shock liver was detected more frequently in the youngest age group, while WD was detected more frequently in adolescence. There was a statistically significant difference among different etiologies of ALF according to age (p-value < 0.001). The box-and-whisker plot with every box representing IQR (Q1 (25th), median, and Q3 (75th)), whiskers representing minimum and maximum patient age in one etiology, circles representing an outlier that was more than 1.5 × IQR of distance from Q3, the y-axis representing the age of the patients in years, and the x-axis representing the etiology of ALF in the studied patients
Complications were significantly associated with mortality (76.7% in the deceased group versus 59.3% in the recovered group) (p-value = 0.021). Sepsis and pneumonia were the most common complications. Moreover, there were significant associations between pneumonia, renal insult, and brain edema and the patients’ mortality (p values of 0.003, < 0.001, and 0.009, respectively).
Hepatic encephalopathy was significantly associated with mortality (76.7% in the deceased group versus 43.2% in the recovered group). Moreover, advanced grades of HE (grades 3 and 4) were higher in the deceased group (47.9%) than in the recovered group (11.1%) (p-value < 0.001).
Prothrombin time was significantly higher in the deceased group in comparison with the recovered group (p-value < 0.001). TB was significantly higher in the deceased group (p-value = 0.019). On the other hand, serum albumin, total protein, and aspartate transaminase (AST) were significantly higher in the recovered group (p-value = 0.012, 0.007, and 0.021, respectively). Serum ammonia was significantly higher in the deceased group (p-value < 0.001), while serum alpha-fetoprotein (AFP) was significantly higher in the recovered group (p-value 0.003) (Table 2).
The diagnostic performance of INR, PTT, TB, AST, albumin, total protein, ammonia, creatinine, ionized calcium, and AFP on admission significantly discriminates between the recovered and deceased groups (Table 3).
Discussion
This study has demonstrated that HAV infection is the main etiology of ALF in Egyptian children. Socioeconomic conditions and poor sanitary conditions make infections, including HAV, the most probable cause of ALF in pediatric age in developing countries, e.g., Egypt [12]. Also, the estimated prevalence of HAV-induced ALF in countries with routine HAV immunization was markedly lower than the estimated prevalence in countries without routine HAV immunization. In Argentina, the prevalence of HAV-induced ALF prior to routine immunization was approximately 50%, compared with approximately 1% after immunization was introduced [13].
The high mortality rate in the first 5 days of admission may be due to the inability to identify the etiology in undiagnosed cases in addition to a lack of awareness about the disease and delayed reference of cases. Also, in developing countries, there is a shortage and lack of required investigations needed for diagnosis.
In the present study, different ALF etiologies were significantly associated with mortality. This agrees with Jain and Dhawan [14], who highlighted the association between the etiology of ALF in children and prognosis. In the present study, 87.5% of AIH-induced ALF survived with their native liver without the need for LT, which agrees with Di Giorgio et al. [15], who demonstrated that AIH-induced ALF may have a high transplant-free survival rate when diagnosed and treated promptly. Response to steroid therapy in AIH is so universal that documented treatment response is used as a diagnostic criterion [16].
There was a statistically significant difference among the different etiologies of ALF regarding age. HAV was detected more in the preschool age group (3–6 years). The etiology of ALF in children varies significantly according to age and worldwide location [17].
Preschool-age children are often more affected because they may not be able to follow instructions or make decisions to keep them away from infections. Children have more contact with others, and they have less developed immune systems to fight off infections which may explain why they are more likely to catch an illness that can spread from person to person [18].
In this study, the timing of death for 63% of the deceased group occurred within the first 5 days of admission. So, rapid transfer to a transplant center and early preparation of donors for LT are important to decrease mortality rates. This is in accordance with Ng et al. [19], who reported that 58% of deaths occurred in the first 7 days after admission.
In the current study, the mortality rate recorded was 47.4%, which is high when compared to 4.6% in the USA [4], 16% in Denmark [20], and 38% in Germany [21], but in accordance with the mortality rate of 42.2% reported in India [22]. It is lower than the 51.2% reported in central Africa [23]. This may be explained by improved ALF treatment and easy accessibility to LT centers in the Western world. Unfortunately, in developing countries, high mortality due to ALF may be related to delayed access to specialized care, intensive care units, experienced LT centers, and delayed donor preparation [23].
Children with ALF and HE have a higher risk of mortality and more often require emergent liver transplantation. The best clinical care for these patients takes place at an experienced center [24]. The majority of the patients (37.4%) were presented with HE grade I, and they had a better prognosis than those who presented with other grades. In the present study, HE was significantly associated with mortality. Death occurred in 27% of patients who presented without HE. This emphasized that the presence of HE is unnecessary for the diagnosis of ALF in pediatrics. HE is difficult to assess in children and, in fact, may never become clinically apparent in the setting of ALF. So, the PALF study group specified a coagulopathy-based definition of ALF in children.
Serum alpha-fetoprotein (AFP) is a glycoprotein produced by the embryonic yolk sac and fetal liver, and its serum concentration declines throughout pregnancy and after birth [25]. In this study, AFP was significantly higher in the recovered group. This is similar to Chien et al. [26], who reported that increasing AFP levels during the clinical course was related to better outcomes. This increase was thought to be associated with hepatic regeneration. This could be attributed to the fact that regenerating hepatocytes have features that resemble those of fetal hepatocytes [27, 28].
The present study demonstrated a significantly higher chance of death if INR exceeds 2.97 with best sensitivity (84%), specificity (70%), and area under the receiver operating characteristic curve (AUROC) (0.826). Other laboratory variables including serum albumin, ammonia, and creatinine were significant predictors of death. These results are in accordance with Kathemann et al. [21], who reported that serum ammonia and albumin levels could predict ALF outcomes in pediatrics. Radaelli et al. [23] demonstrated that the main prognostic determinants were young age (< 14.5 months), hepatic encephalopathy (III–IV), INR (> 4.55), ALT (< 219 IU/l), and pallor.
In conclusion, ALF is a rapidly progressive clinical condition with high mortality (47.4%) that occurs mainly in the first 5 days of admission. High values of INR, PTT, TB, ammonia, and creatinine at presentation may be a potential marker for predicting mortality in ALF in children. So, early referral of patients to a pediatric-hepatology specialized center with experience in pediatric liver transplantation is recommended. Moreover, immediate donor preparation is advised because about half of mortality occurs within the first 5 days of admission.
Increasing disease awareness, vaccination, and all measures for the prevention of HAV, which is the most common cause of ALF in Egyptian children are crucial to eliminate this preventable disease and its complications.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AFP:
-
Alpha-fetoprotein
- AIH:
-
Autoimmune hepatitis
- ALF:
-
Acute liver failure
- ANA:
-
Antinuclear antibody
- CMV:
-
Cytomegalovirus
- HAV:
-
Hepatitis A virus
- HE:
-
Hepatic encephalopathy
- INR:
-
International normalized ratio
- LKM-1:
-
Liver kidney microsome type-1
- LT:
-
Liver transplantation
- PALF:
-
Pediatric Acute Liver Failure
- PT:
-
Prothrombin time
- ROC:
-
Receiver operating characteristic
- SD:
-
Standard deviation
- SMA:
-
Smooth muscle antibody
- TB:
-
Total bilirubin
- WD:
-
Wilson disease
References
Alonso EM (2017) Acute liver failure. In: D. A. K. MD (ed) Diseases of the liver and biliary system in children. The Liver Unit Birmingham Children’s Hospital NHS Foundation Trust and University of Birmingham, Birmingham, pp 271–287
Bouter L, Zeegers M, and Lee T (2023): Textbook of epidemiology, Second edition, John Wiley & Sons Ltd. https://WWW.welly.com. ch.1, Epidemiology, 2–13
Kulkarni S, Perez C, Pichardo C, Castillo L, Gagnon M, Beck-Sague C, Gereige R, Hernandez E (2015) Use of Pediatric Health Information System database to study the trends in the incidence, management, etiology, and outcomes due to pediatric acute liver failure in the United States from 2008 to 2013. Pediatr Transplant 19:888–895
Squires JE, Alonso EM, Ibrahim SH, Kasper V, Kehar M, Martinez M, Squires RH (2022) North American society for pediatric gastroenterology, hepatology, and nutrition position paper on the diagnosis and management of pediatric acute liver failure. J Pediatr Gastroenterol Nutr 74:138–158
Bhatt H, Rao GS (2018) Management of acute liver failure: a pediatric perspective. Curr Pediatr Rep 6:246–257
Narkewicz MR, Horslen S, Hardison RM, Shneider BL, Rodriguez-Baez N, Alonso EM, Ng VL, Leonis MA, Loomes KM, Rudnick DA (2018) A learning collaborative approach increases specificity of diagnosis of acute liver failure in pediatric patients. Clin Gastroenterol Hepatol 16:1801–1810
Berardi G, Tuckfield L, DelVecchio MT, Aronoff S (2020) Differential diagnosis of acute liver failure in children: a systematic review. Pediatr Gastroenterol Hepatol Nutr 23:501–510
Mataya LA, Srinivasan V, Rand EB, Alcamo AM (2021) Multiple organ involvement and ICU considerations for the care of acute liver failure (ALF) and acute on chronic liver failure (ACLF) in children. Transl Pediatr 10:2749–2762
Bhatt H, and Rao GS (2019) Medical management of acute liver failure. Pediatr Criti Care Curr Controversies 6:155–173
Lutfi R, Abulebda K, Nitu ME, Molleston JP, Bozic MA, Subbarao G (2017) Intensive care management of pediatric acute liver failure. J Pediatr Gastroenterol Nutr 64:660–670
Taylor SA, Whitington PF (2016) Neonatal acute liver failure. Liver Transpl 22:677–685
Riebensahm C, Ka D, Sow A, Semmo N, Wandeler G (2019) A closer look at the spectrum of drug-induced liver injury in sub-Saharan Africa. Expert Rev Clin Pharmacol 12:875–883
Patterson J, Hussey HS, Silal S, Goddard L, Setshedi M, Spearman W, Hussey GD, Kagina BM, Muloiwa R (2020) Systematic review of the global epidemiology of viral-induced acute liver failure. BMJ Open 10:37–47
Jain V, Dhawan A (2016) Prognostic modeling in pediatric acute liver failure. Liver Transpl 22:1418–1430
Di Giorgio A, Bartolini E, Calvo P, Cananzi M, Cirillo F, Della Corte C, Dionisi-Vici C, Indolfi G, Iorio R, Maggiore G (2021) Diagnostic approach to acute liver failure in children: a position paper by the SIGENP liver disease working group. Dig Liver Dis 53:545–557
Steinmann S, Lohse AW (2023) Treatment of autoimmune hepatitis: budesonide does not solve our problems. Hepatology 77:1071–1073
Squires JE, McKiernan P, Squires RH (2018) Acute liver failure: an update. Clin Liver Dis 22:773–805
Côté SM, Petitclerc A, Raynault MF, Xu Q, Falissard B, Boivin M, Tremblay RE (2010) Short-and long-term risk of infections as a function of group child care attendance: an 8-year population-based study. Arch Pediatr Adolesc Med 164:1132–1137
Ng VL, Li R, Loomes KM, Leonis MA, Rudnick DA, Belle SH, Squires RH (2016) Outcomes of children with and without hepatic encephalopathy from the Pediatric Acute Liver Failure (PALF) Study Group. J Pediatr Gastroenterol Nutr 63:357–360
Nordmann Winther T, Nielsen AY, Lund A, Larsen FS, Jørgensen MH (2023) High yield on aetiology using a systematic diagnostic approach to paediatric acute liver failure, analysis of a nationwide cohort. Acta Paediatr 112:1082–1090
Kathemann S, Bechmann LP, Sowa J-P, Manka P, Dechêne A, Gerner P, Lainka E, Hoyer PF, Feldstein AE, Canbay A (2015) Etiology, outcome and prognostic factors of childhood acute liver failure in a German Single Center. Ann Hepatol 14:722–728
Alam S, Khanna R, Sood V, Lal BB, Rawat D (2017) Profile and outcome of first 109 cases of paediatric acute liver failure at a specialized paediatric liver unit in India. Liver Int 37:1508–1514
Radaelli S, Houndjahoue G, Bogning Mejiozem O, Mattei V, Galloni D, Martin C (2021) Pediatric acute liver failure in Central African Republic: epidemiology and prognostic modeling. Pediatr Ther 11:1–7
Bartlett JA, and Kohli R (2023) Hepatic Encephalopathy in Children. Indian J Pediatr 91:1–6
Gayathri P, Krishnamoorthy S, Chandra S, Pillai MK, Menon R, Iyer MS (2021) Prognostic markers in acute liver failure-Alpha feto protein. Arch Med Health Sci 9:55–59
Chien MM, Chang MH, Chang KC, Lu FT, Chiu YC, Chen HL, Ni YH, Hsu HY, Wu JF (2019) Prognostic parameters of pediatric acute liver failure and the role of plasma exchange. Pediatr Neonatol 60:389–395
Yang S-S, Cheng K-S, Lai Y-C, Wu C-H, Chen T-K, Lee C-L, Chen D-S (2002) Decreasing serum alpha-fetoprotein levels in predicting poor prognosis of acute hepatic failure in patients with chronic hepatitis B. J Gastroenterol 37:8–10
da Silva Silvestre JP, da Cruz Coelho LM, Póvoa PMSR (2010) Impact of fulminant hepatic failure in C-reactive protein? J Crit Care 25:657–670
Acknowledgements
Not applicable.
Funding
The study was funded by the National Liver Institute, Menoufia University, Egypt, without any particular role in the study design, recruitment of individuals, data analysis, or writing of the report.
Author information
Authors and Affiliations
Contributions
BB, AS, and OF were involved in the study concept and design. NM, AS, and OF were involved in the recruitment of patients and follow-up and contributed to the data acquisition. SE and NM performed the statistical analysis. NM, AS, and OF performed the interpretation of results and wrote the manuscript. All the authors reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study procedures were carried out and approved by the Ethical Committee of the National Liver Institute and in accordance with the Declaration of Helsinki.
Informed written consent was obtained from legal guardians.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mansour, N.S., Behairy, B.ES., Sira, A.M. et al. Epidemiology of acute liver failure in Egyptian children. Egypt Liver Journal 14, 39 (2024). https://doi.org/10.1186/s43066-024-00346-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-024-00346-3