
Abstract
Background
Telmisartan is a non-peptide angiotensin II receptor antagonist which acts by ACE/AngII/AT1 axis blockade (ARB). In the last years increasing evidence of its metabolic benefits pointed out this drug as the most promising ARB for nonalcoholic fatty liver disease (NAFLD) treatment. The aim of the present study was to investigate the Telmisartan effect on treating NAFLD in mice fed with a high-fat diet evaluating liver gene modulation. Twenty-four male mice were divided into four groups and fed for 60 days with a standard diet (ST), standard diet plus TEL (ST+TEL 5 mg/kg/day by gavage for 4 weeks), high-fat diet (HFD), or high-fat diet plus TEL (HFD+TEL 5 mg/kg/day by gavage for 4 weeks). Body weight, lipid profile, insulin, alanine transaminase, and aspartate aminotransferase were evaluated. Liver histology was analyzed. US imaging was performed to access liver dimension and echogenicity and also epididymal fat pad thickness. The expression of proinflammatory resistin/TRL4/MYD88 pathway was analyzed.
Results
The main findings showed that TEL reduced the resistin, TRL4, and Myd88 liver expression in the HFD + TEL group when compared to the obese control group (HFD). Decreased hepatic steatosis in the HFD + TEL group demonstrated by US measurements of the liver longitudinal axis and echogenicity were observed. In addition, TEL reduced epididymal adipose pad thickness, body weight, transaminases, and improved glucose tolerance test and HDL cholesterol.
Conclusions
We observed that Telmisartan treatment improved metabolism, decreasing NAFLD.
Graphical Abstract
Telmisartan improves metabolic and lipid profile and liver steatosis of obese mice

Similar content being viewed by others


Background
The diet and lifestyle changes in the last decades culminated in a worldwide increase in the metabolic syndrome (MetS) prevalence; a complex disorder associated with multiple clinical components such as obesity, hypertension, dyslipidemia, glucose intolerance, and insulin resistance (type 2 diabetes) [1]. Non-alcoholic fatty liver disease (NAFLD) is now considered the hepatic component of MetS since both conditions share the same risk factors [2]. With a global prevalence estimated to be 25.2% of the total population and with wide geographical variation across the world [3, 4], NAFLD stands out as one of the main causes of chronic liver pathology and is defined as a fatty hepatocyte infiltration, excluding alcohol abuse situations (women ≤20 g/d, men ≤30 g/d). The excessive fat culminates in increased oxidative stress, which starts a cycle of injury, inflammation, and fibrosis in the hepatic parenchyma. Some patients reach the most serious spectrum of the disease, with nonalcoholic steatohepatitis (NASH) and/or liver cirrhosis and its clinical consequences, including carcinogenesis [5].
As a clinically silent condition and with nonspecific laboratory markers, NAFLD diagnosis is imaging-based or by histological techniques [6, 7]. The NAFLD pharmacotherapy priority is to improve the disease pathophysiology preventing the NAFLD evolution into NASH the most serious form of liver disease [8]. Thus, telmisartan has been shown to be a powerful ally for this goal, demonstrating positive results in hepatic steatosis, insulin resistance, inflammation, and fibrosis [9, 10].
Telmisartan (TEL) is one of the main drugs widely used for the systemic arterial hypertension treatment improving the hypertension-related cardiovascular end-organ damage. TEL acts as an angiotensin type I receptor blocker (ARB) and presents excellent tolerance and safety [11]. Recent studies highlighted possible TEL metabolic effects improving MetS parameters and patients’ glycemic control [12]. Animal studies also demonstrate promising hepatoprotective effects with this ARB against fat infiltration and inflammation of liver parenchyma [13].
Toll-like receptors (TRLs) are a family of pattern recognition receptors, being identified as 11 TLRs in humans with several ligands [14]. TRL receptors participate in the defense against many pathogens and play a crucial role in the innate immune system function by activating NF-kB and other signaling pathways to produce inflammatory cytokines. The TLR4 is the most studied receptor [15, 16], and its intracellular signaling produces the complex TLR4/myeloid differentiation factor 2 (MD2) through human myeloid differentiation factor 88 (MyD88) resulting in the migration of nuclear factor-κB (NF-κB) transcription factor [17], which modulates inflammation.
Another important proinflammatory molecule is the resistin, which is now considered a protein “found in the inflammatory zone” (FIZZ), that actively participates in the inflammation process by inducing and responding to several stimuli-like cytokines, mitogens, and endotoxins [18]. Its levels are increased in some conditions such as chronic liver diseases, obesity [19], lung diseases [20], atherosclerotic plaques [9], arthritis [21], and kidney disease [22]. It has been demonstrated strong correlation of resistin with other inflammatory markers such as C-reactive protein, tumor necrosing factor (TNF-α) [23], interleukin-6 (IL-6), and soluble vascular adhesion molecules, so its reduction has been faced as a promising predictive tool in chronic diseases [10].
In this context, the present study aimed to investigate the TEL treatment ability to improve NAFLD in high-fat fed mice evaluating liver anti-inflammatory effects associated with gene expression.
Material and methods
Animals
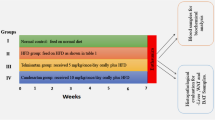
The experiment was conducted with 24 male FVB/N mice (4 weeks old), which were randomly divided into four groups (n = 6) and fed with the following experimental diets for 4 weeks with control diets or a high-fat diet and then treated for additional 4 weeks with TEL 5 mg/kg/d by gavage being divided as follows: standard diet (ST), standard diet plus TEL (ST+ TEL), high-fat diet (HFD), and high-fat diet plus TEL (HFD+ TEL). Metabolic effects of TEL have been demonstrated especially when it was given at doses ≥ 5 mg·kgbw-1·day-1 [24]. This study was approved by the Ethics Committee of Experimentation and Animal Welfare of Unimontes, Montes Claros, Brazil (process no. 022/2012).
Diets
The control group animals were fed with a diet that presented an energetic value of 2.18 Kcal per 1 g of diet, containing the following components: 50.30% carbohydrate, 41.90% protein, and 7.80% fat (Labina, Purina, St. Louis, MO, USA) [25]. The high-fat diet was composed of 24.55% of carbohydrates, 14.47% of proteins, and 60.98% of fats, presenting a total of 5.28 kcal per 1 g of diet [26]. All the high-fat diet components were purchased from Rhoster LTDA (São Paulo, Brazil).
Measurements of body weight, food intake, and tissue collection
The mice were individually housed and the food intake was measured twice per week during treatment to determine food efficiency (food intake/body weight). Overnight-fasted mice were sacrificed with ketamine (130 mg/kg) and xylazine (0.3 mg/kg) after anesthesia [25, 26]; sample tissues were collected, weighted, and immediately frozen in liquid nitrogen and stored at −80 °C for posterior analysis.
Ultrasound imaging (US)
Animals were studied in a supine position, on the day before the sacrifice, by the same trained radiologist, using Medison® ultrasound equipment (Seoul, South Korea), with a multifrequency linear transducer (7.0 to 12 MHz). All imaging was performed in fundamental brightness mode (B mode), with optimization of the gain and the time gain compensation settings, which were kept constant throughout the experiment. The acoustic focus was placed in the center of the target organs (liver and epididymal fat pad), with the measurement of liver echogenicity, size (longitudinal axis), and epididymal fat pad thickness. Liver echogenicity was analyzed using the public domain Java image processing program ImageJ (Wayne Rasband, Research Services Branch, National Institute of Mental Health, Bethesda, Maryland, USA). A region of interest (ROI) was determined arbitrarily in the constant area of ultrasound images of the liver parenchyma, covering a wide area and excluding large vessels as far as possible. The average intensity in the ROI was measured and relative values were compared.
Determination of blood measurements
The animal’s lipid and hepatic profiles were analyzed by measuring the serum levels of total cholesterol, high-density lipoprotein (HDL), triacylglycerol, and aspartate and alanine transaminases (AST and ALT). For the aforementioned measurements, serum was obtained after blood centrifugation at 3200 rpm for 10 min at 4 °C. All analyzes were performed using specific enzymatic kits (Wiener Laboratories, Rosario, Argentina).
Hematoxylin and eosin staining
Liver samples were fixed in formaldehyde solution (10%) and embedded in paraffin serially sectioned at 5 mm, stained with hematoxylin and eosin (HE), and evaluated under a conventional light microscope using an Olympus BX50 microscope (Tokyo, Japan) under the 20 × optical magnification. For each slide, images from the three most affected fields (×20 objective lenses) were considered. Biopsy analyses were classified according to Hübscher (2006) depending on fat accumulation [27].
Analysis of proinflammatory gene expression in the liver
In order to verify the anti-inflammatory effects of TEL in NAFLD, specific liver inflammatory process genes were evaluated. Hepatic tissue fragments were used to obtain total RNA using TRIzol Reagent (Thermo Fisher Scientific, Waltham, MA, USA). The total RNA obtained was treated with DNAse (Promega), and the RNA transcription into cDNA was obtained via reverse transcription M-MLV (Invitrogen Corp.) using random hexamer primers.

Food intake, energy intake, and body weight in mice treated with Telmisartan and fed with a standard and high-fat diet (ST, ST+TEL, HFD, HFD+TEL). Food intake (a), energy intake (b), body weight (c), and area under the curve (d). Data are presented as mean ± SEM; *p<0.05, **p<0.01, and ***p<0.001
Gene expression was normalized to endogenous glyceraldehydes-3-phosphate dehydrogenase (GAPDH). The mRNA levels of the genes were determined by qRT-PCR and amplified using specific primers and reagent SYBR green (Applied Biosystems, USA) on 384-well Quant Studio 6 flex equipment (Applied Biosystems). The primer sequences are detailed in Table 1.
For the relative quantification, the standard dietary group (control group) was employed as a calibrator. The results were quantified as cycle threshold (Ct) values, where Ct was defined as the PCR threshold cycle in which the amplified product is first detected and defined as relative gene expression (the target/endogenous ratio). The relative gene expression was analyzed by the 2ΔΔCt method [28].
Statistical analysis
All data were transferred to GraphPad Prism software (Version 5.0, GraphPad Software Inc., San Diego, CA, USA) and analyzed with confidence 95% and considered P < 0.05 was statistically significant. All the data reported in the present study are presented as the mean ± standard deviation (SD) and analyzed via one-way ANOVA followed by Bonferroni post-test.
Results
Mice fed with HFD had a higher energy intake than those fed with an STD diet, and treatment with TEL did not reduce their energy intake (ST:2.69 ± 0.07; ST+TEL:2.40 ± 0.05; HFD:3.20 ± 0.13; HFD+TEL:3.25 ± 0.15) (Fig. 1a, b). ST animals had lower body weight when compared with HFD animals during all the experiments, and treatment with TEL significantly decreased body weight in the HFD group but not in the ST group (ST:281.4 ± 5.51; ST+TEL:317.5 ± 11.25; HFD:373.6 ± 11.25; HFD+TEL:326.6 ± 15.12) (Fig. 1c, d).
Epididymal fat pad weight was higher in the HFD group when compared with the ST group, and treatment with TEL significantly reduced this weight in the HFD+TEL group (ST:0.007 ± 0.001; ST+TEL:0.01 ± 0.0006; HFD:0.02 ± 0.002; HFD+TEL:0.013 ± 0.001) (Fig. 2c). US measurements of the epididymal fat pad thickness show similar results, with higher measures in HFD animals than in ST animals, and with a significant reduction in epididymal fat pad thickness in the HFD+TEL group in relation to the HFD group (ST, 0.667 ± 0.0667; ST+TEL, 0.733 ± 0.066; HFD, 0.967 ± 0.033; HFD+TEL, 0.600 ± 0.058) (Fig. 2a, b).

Adiposity, epididymal, and mesenteric adipose tissues in mice treated with Telmisartan and fed with a standard and high-fat diet (ST, ST+TEL, HFD, HFD+TEL). Epididymal US images (a), epididymal fat pad thickness accessed by US (b), epididymal adipose tissue weight (c), mesenteric adipose tissue weight (d), and adiposity (e). Arrows in A indicate the epididymal fat pad. Data are presented as mean ± SEM; *p<0.05, **p<0.01
Mesenteric adipose tissue also had significantly reduced weight in the HFD + TEL group when comparing with the HFD group (ST, 0.004 ± 0.001; ST+TEL, 0.005 ± 0.0004; HFD, 0.08 ± 0.02; HFD+TEL, 0.004 ± 0.0004) (Fig. 2d). Total adiposity was higher in the HFD group in comparison with the ST groups and was significantly reduced in the HFD+TEL group when compared with the HFD group (ST, 0.013 ± 0.001; ST+TEL, 0.016 ± 0.001, HFD, 0.031 ± 0.002; HFD+TEL, 0.018 ± 0.001 (Fig. 2e).
A low-glucose tolerance was observed in HFD mice when compared with STD animals, and this parameter was significantly improved in the HFD + TEL group (ST, 27314 ± 3393; ST+TEL, 32355 ± 1214; HFD, 49454 ± 2439; HFD+TEL, 39802 ± 1401) (Fig. 3a). Although insulin sensitivity test showed this same tendency, no statistical significance was observed (Fig. 3b). Triacylglycerols did not significantly differ between the groups (ST, 111.8 ± 6.29; ST+TEL, 125.7 ± 10.49; HFD, 128.3 ± 9.304; HFD+TEL, 142.0 ± 13.53) (Fig. 3c). The HFD+TEL group had higher concentrations of HDL cholesterol than the ST and HFD groups (ST, 64.08 ± 4.40; ST+TEL, 56.20 ± 4.02; HFD, 65.98 ± 2.94; HFD+TEL, 83.33 ± 3.44) (Fig. 3e). Regarding parameters related to liver damage, values of ALT (ST, 33.0 ± 2.1; ST+TEL, 38.67 ± 2.40; HFD, 42 ± 1.79; HFD+TEL, 20.75 ± 3.35; P = 46.56) were significantly reduced in the HFD+TEL group (Figs. 3f, g and 4).

Insulin sensitivity and glucose tolerance tests, lipid parameters, and hepatic enzymes in mice treated with Telmisartan and fed with a standard and high-fat diet (ST, ST+TEL, HFD, HFD+TEL). Glucose tolerance test (a), insulin sensitivity test (b), triglycerides (c), total cholesterol (d), high-density lipoprotein (e), aspartate aminotransferase (f), and alanine transferase (g). Data are presented as the mean ± SEM; *p<0.05, **p<0.01, and ***p<0.001 versus the group indicated

Liver ultrasonography (US), weight, and hematoxylin/eosin staining in mice treated with Telmisartan and fed with a standard and high-fat diet (ST, ST+TEL, HFD, HFD+TEL). Scale bar, 200 μm. Liver US images (a), longitudinal axis measured by US (b), echogenicity (c), weight (d), fat infiltration (e), and hematoxylin/eosin staining (f). Arrows in A indicate the liver. Data are presented as the mean ± SEM; *p<0.05, **p<0.01, and ***p<0.001 versus the group indicated
In addition, the analysis indicated that the HFD group had a substantial increase in total liver weight in relation to ST mice and that HFD+TEL significantly reduced this weight (ST, 1.833 ± 0.105; ST+TEL, 1.889 ± 0.07; HFD, 2.233 ± 0.012; HFD+TEL, 1.405 ± 0.065) (Fig. 5). US examination of liver size demonstrated higher measurements of the liver longitudinal axis in HFD when comparing with ST animals, with a substantial decrease in the HFD+TEL group in relation to the HFD group (ST, 1.467 ± 0.088; ST+TEL, 2.000 ± 0.200; HFD, 2.233 ± 0.088; HFD+TEL, 1.467 ± 0.120) (Fig. 5a, b). US analysis of liver echogenicity showed elevated mean gray values in the HFD group, with a significant reduction of this parameter after TEL treatment in the HFD+TEL group when compared with HFD animals (ST, 78.68 ± 3.894; ST+TEL, 97.1 ± 5.556; HFD, 130.9 ± 0.012; HFD+TEL, 94.27 ± 9.199) (Fig. 5a–c). This result was subjectively observed by the radiologist during the exam by an increase in the brightness of the hepatic parenchyma in the HFD group and a decrease in this parameter in the HFD+TEL group (Fig. 5a). The histologic analysis displayed steatosis in the hepatocytes of mice fed a high-fat diet as compared to the standard-fed animals (Fig. 5f). The study also evaluated the effect of telmisartan in the hepatocyte’s fat accumulation in obese mice, revealing that TEL significantly reduced the fat accumulation in the high-fat + TEL-treated animals (ST, 0.159 ± 0.049; ST+TEL, 1.253 ± 0.388; HFD, 2.080 ± 0.659; HFD+TEL, 0.642 ± 0.050) (Fig. 5e, f).

Liver resistin/toll like-4 (TRL-4) and myeloid differentiation primary response 88 (Myd88) mRNA expression performed by qRT-PCR analyses (a, b, c). Data are presented as the mean ± SEM; *p<0.05, **p<0.01, and ***p<0.001 versus the group indicated
The HFD+TEL group significantly reduced the expression of resistin (HFD, 2699± 6071; HFD+TEL, 1203±1128, of TRL4 (HFD, 1.347±0.242; HFD+TEL, 0.153±0.028) and of Myd88 (HFD, 7.630±0.756; HFD+TEL, 0.220±0.137) when compared to the HFD control group (Fig. 5a–c).
Discussion
The present study evaluated the Telmisartan (TEL) efficacy on improving NAFLD in obese mice by modulating resistin, TRL4, and Myd88 inflammatory signaling expression. Despite all the advances in NAFLD/NASH pathophysiology, it is important to emphasize that until today there is no consolidated pharmacological treatment for this hepatic condition, especially considering evidence-based medicine protocols [29].
The main results of the present study showed that TEL effectively protects obese mice against NAFLD and ameliorates several metabolic parameters. The results are in consonance with previous studies which pointed to TEL as the most promising ARB for NAFLD treatment in terms of both safety and efficacy [30]. The pathological changes found in NAFLD may help to understand these findings considering that this hepatic disorder is associated with the renin-angiotensin-system (RAS) inflammatory arm activation [10]. NAFLD is commonly linked to obesity and insulin resistance, which leads to liver fat import and export imbalance [31]. Other relevant cytokines are altered producing an imbalance between pro- and antioxidant actions and pro- and anti-inflammatory effects, which may contribute to the NAFLD progression to aggravated liver disease such as NASH and fibrosis [32].
The present data demonstrated that HFD mice present a worse glucose profile when compared with ST animals, with a lower glucose tolerance, which was significantly improved by TEL treatment. Concerning insulin sensitivity, a similar tendency was observed despite no statistical significance, which might be explained by the relatively short experiment duration.
The renin-angiotensin system (RAS) has been faced as a two-arms balance with opposite effects on the body composition. Several disease processes are able to unbalance this system. The ACE2/Ang-(1–7)/Mas axis is the antagonist arm with protective effects counteracting the deleterious effects of ACE/Ang II/AT1R axis excessive activation [33]. Evidence suggests that obesity activates the inflammatory RAS arm composed (ACE/Ang II/AT1R) [34] pointing to Angiotensin II (Ang II) as a key piece in the abnormal hepatic lipid metabolism observed in NAFLD [35], which modifies intracellular insulin signaling by several mechanisms that ultimately result in worsening of insulin resistance. Ang II also induces the generation of reactive oxygen species (ROS), that initiates and propagates the pro-inflammatory mediator’s production, such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α) and plasminogen activator inhibitor-1 (PAI-1), resulting in inflammation and additional impairment of insulin signaling, creating a vicious cycle of steatosis, necroinflammation, and fibrosis [31]. On the other hand, increasing evidence has shown the beneficial effects of the ACE2/Ang-(1-7)/Mas axis on liver function and metabolism, with an important anti-obesity role in improving insulin sensitivity, glucose tolerance, and type 2 diabetes; modulating body fat; increasing adiponectin production; and reverting hyperleptinemia [32, 36].
Concerning AT1R-independent effects, it is important to emphasize the relationship between TEL and peroxisome proliferator-activated receptor gamma (PPAR-γ) activation. The nuclear PPARγ receptor is a transcription factor that regulates genes related to adipogenesis, lipid metabolism, and insulin sensitivity. TEL, unlike other ARBs, can work as a partial agonist of PPAR-γ [13], increasing insulin sensitivity, high-density lipoprotein levels, and decreasing inflammation, oxidative stress, cell proliferation, migration, fatty acid, and triglyceride levels. This effect occurs without the side effect of liquid retention produced by full PPAR-γ agonists such as pioglitazone or rosiglitazone [37].
TEL not only modulates RAS in order to inhibit AngII/AT1R deleterious effects, but also increases the activity of ACE2/Ang-(1-7)/Mas arm [33], beyond its PPAR-γ partial agonistic effects [34] and has been consistently proven to reduce insulin resistance [12]. We demonstrated a significant improvement in liver size and hepatic lipid droplet infiltration in the HFD group treated with TEL, in accordance with previous studies [13]. The morphological findings were positively correlated with the liver ultrasound (US) exam on the day before the sacrifice. Ultrasound was effective in demonstrating a higher liver size in the HFD group and a substantial decrease in this parameter when the HFD animals were treated with TEL. Also, US analysis of liver echogenicity showed elevated mean gray values in the HFD group, with a significant reduction of this parameter after TEL treatment in the HFD+TEL group. As in humans, hepatic steatosis in rodents is classically described on US as a diffuse increase in hepatic echogenicity, or “bright liver,” due to increased reflection of US from the liver parenchyma, which is caused by intracellular accumulation of fat vacuoles [35]. Another parameter, such as reduced visualization of the diaphragm and of small peripheral vessels, with no changes in the liver surface, can also be utilized [38].
We also demonstrated that TEL reduces the adiposity and the mesenteric and epididymal adipose tissue weights in the HFD+TEL group when compared with the HDF group. Liao et al. [37] used measurements of epididymal fat pad thickness echography to successfully access the amount of this adipose tissue deposition. Kudo et al. [39] showed for the first time that TEL decreases the adipocyte size and upregulates the adiponectin secretion without affecting food intake in a murine NASH model, reducing the accumulation of visceral fat. Moreover, TEL but not the ARB Valsartan, increased the expression of both nuclear-encoded and mitochondrial-encoded genes in the skeletal muscle known to play important roles in mitochondrial energy metabolism.
Thus, in addition to a class effect of ARBs in modulating adipocyte size, the present findings raise the possibility that TEL may have a particularly strong impact on fat cell volume and fat accumulation and stand out in its metabolic effects, which may help to protect against dietary-induced visceral obesity and weight gain. The efficacy of TEL in reducing visceral fat mass may be relevant for patients since an increase in visceral fat is related to hypertension, dyslipidemia, and an impaired metabolic pattern, but also works as an independent predictor of mortality in humans [40].
Telmisartan effectively reduced liver expression of the pro-inflammatory resistin/TRL4/MYD88 pathway in HFD animals. Resistin is an important adipokine in an obesity setting and is positively correlated with increased fat mass and with a proinflammatory state, as reported in chronic liver diseases [41]. Resistin modulates the synthesis and secretion of essential proinflammatory cytokines such as TNF-α and IL-6 by an NF-κB-dependent pathway [42]. Santos et al. [43] showed that rats with HFD-induced obesity presented increased hepatic expression of resistin/TRL4/MAPK/NF-KB pathway developing insulin resistance, glucose intolerance, hyperinsulinemia, and dyslipidemia.
Toll-like receptors (TRLs) are expressed in immune cells and works in the immunological response to microbial agents. The activation of TRLs induces antimicrobial pathways of the innate defense, upregulation of antigen-presentation molecules, and secretion of cytokines that influence adaptive immune response. Inappropriate activation of TRL pathways by endogenous or exogenous ligands may lead to the initiation and/or perpetuation of autoimmune responses and tissue damage [14]. It has recently been reported that the TRL4 signaling pathway plays an important role in the progression of hepatic inflammation and fibrosis. This effect occurs by triggering the expression of proinflammatory cytokines through mydd88-dependent activation that in turn is mediated by interleukin receptor-associated kinase IL-1 (IRAK), factor 6 associated with tumor necrosis factor receptor (TRAF6) and kinase 1 activated by transforming growth factor 1, which activates IkB kinase (IKK), leading to transcription of the NF-kB [44]. Alquami et al. [45] corroborated these findings by demonstrating that rats fed with a high-fructose diet showed hepatic TRL4 overexpression.
The antifibrotic and hepatoprotective effects of TEL in different animal models [38] and human have been reported in several studies. TEL has been shown to have hepatoprotective effects on NAFLD decreasing hepatic fibrosis via its antioxidant and anti-inflammatory activity by preventing NF-kB signaling pathway stimulation [45]. Similar results were described in humans were TEL reduced hepatic oxidative stress and fibrogenesis in patients with NAFLD and chronic hepatitis C [1].
Telmisartan reduced liver damage resulting from type I diabetes mellitus [38] and when associated with propranolol reduced the liver fibrosis signs in a murine model of primary sclerosing cholangitis (PSC) [46]. Yi et al. showed that TEL was also able to prevent liver fibrosis in a rat bile duct ligation model [47]. In mice fed with a high-fat diet treated with streptozotocin (STZ) low dose (2 days after birth), treatment with TEL reduced liver inflammation and fibrosis [48]. Similarly, TEL reduced short- or long-term diet-induced hepatic fibrosis in rats [49] preventing hepatocellular carcinoma [50]. The anti-inflammatory activity of TEL can be partly explained by the RAS blockade (AngII/AT1R), which plays an important role in the induction and maintenance of inflammation and oxidative stress [51,52,53].
Conclusion
In conclusion, the present study indicates that oral treatment with Telmisartan offers a protective effect against liver damage in NAFLD and improves lipid and glucose metabolism in high-fat fed mice. Telmisartan effectively reduced hepatic pro-inflammatory resistin/TRL4/MYD88 expression in obese animals, which could explain, at least in part, the positive effects on improving liver fat deposition.
Availability of data and materials
All data generated or analyzed during this study are included in this article and its supplementary information.
Abbreviations
- ARB:
-
Angiotensin type I receptor blocker
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- GAPDH:
-
Endogenous glyceraldehyde 3-phosphate dehydrogenase
- HDL:
-
High-density protein
- HE:
-
Hematoxylin and eosin
- HFD:
-
High-fat diet
- IKK:
-
IkB kinase
- IL-1:
-
Interleukin-1
- IL-6:
-
Interleukin-6
- IRAK:
-
Interleukin receptor-associated kinase IL-1
- LDL:
-
Low-density protein
- MD2:
-
Myeloid differentiation factor 2
- MetS:
-
Metabolic syndrome
- MyD88:
-
Myeloid differentiation factor 88
- NAFLD:
-
Non-alcoholic fatty liver disease
- NASH:
-
Nonalcoholic steatohepatitis
- NF-κb:
-
Nuclear factor-κB
- PAI-1:
-
Plasminogen activator inhibitor-1
- PPAR-γ:
-
Peroxisome proliferator-activated receptor gamma
- PSC:
-
Primary sclerosing cholangitis
- SD:
-
Standard deviation
- ST:
-
Standard diet
- TEL:
-
Telmisartan
- TNF-α:
-
Tumor necrosis factor-alpha
- TRAF6:
-
Tumor necrosis factor receptor
- TRLs:
-
Toll-like receptors
- RAS:
-
Renin-angiotensin-system
- ROS:
-
Reactive oxygen species
- STZ:
-
Streptozotocin
References
Enjoji M, Kotoh K, Kato M et al (2008) Therapeutic effect of ARBs on insulin resistance and liver injury in patients with NAFLD and chronic hepatitis C: a pilot study. Int J Mol Med 22(4):521–527. https://doi.org/10.3892/ijmm_00000051
Byme CD, Targher G (2015) NAFLD: a multisystem disease. J Hepatol 62(1 Suppl):S47–S64. https://doi.org/10.1016/j.jhep.2014.12.012https://pubmed.ncbi.nlm.nih.gov/?term=Byrne+CD&cauthor_id=25920090
Mitra S, De A, Chowdhury A (2020) Epidemiology of non-alcoholic and alcoholic fatty liver diseases Transl. Gastroenterol Hepatol 5:16. https://doi.org/10.21037/tgh.2019.09.08
Younossi Z, Marchesini G, Pinto-Cortez H, Petta S (2019) Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: Implications for Liver Transplantation. Transplantation 103(1):22-27. https://doi.org/10.1097/TP.0000000000002484
Kramer H, Pickhardt PJ, Kliewer MA et al (2017) Accuracy of Liver Fat Quantification With Advanced CT, MRI, and Ultrasound Techniques: Prospective Comparison With MR Spectroscopy. AJR Am J Roentgenol 208(1):92–100. https://doi.org/10.2214/AJR.16.16565
Hernaez R, Lazo M, Bonekamp S et al (2011) Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology 54(3):1082–1090. https://doi.org/10.1002/hep.24452
Schwimmer JB, Dunn W, Norman GJ et al (2010) SAFETY study: alanine aminotransferase cutoff values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology 138(4):1357–1364. https://doi.org/10.1053/j.gastro.2009.12.052
Chalasani N, Younossi Z, Lavine JE et al (2012) The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 55:2005–2023. https://doi.org/10.1002/hep.25762
Jung HS, Park KH, Cho YM et al (2006) Resistin is secreted from macrophages in atheromas and promotes atherosclerosis. Cardiovasc Res 69(1):76–85. https://doi.org/10.1016/j.cardiores.2005.09.015
Efstathiou SP, Tsiakou AG, Tsioulos DI et al (2007) Prognostic significance of plasma resistin levels in patients with atherothrombotic ischemic stroke. Clin Chim Acta 378(1-2):78–85. https://doi.org/10.1016/j.cca.2006.10.023
Mehta SR, Thomas EL, Patel N et al (2010) Proton magnetic resonance spectroscopy and ultrasound for hepatic fat quantification. Hepatol Res 40(4):399–406. https://doi.org/10.1111/j.1872-034X.2009.00620.x
Guimaraes GG, Santos SH, Oliveira ML et al (2012) Exercise induces renin-angiotensin system unbalance and high collagen expression in the heart of Mas-deficient mice. Peptides 38(1):54–61. https://doi.org/10.1016/j.peptides.2012.05.024
Michel MC, Brunner HR, Foster C, Huo Y (2016) Angiotensin II type 1 receptor antagonists in animal models of vascular, cardiac, metabolic and renal disease. Pharmacol Ther 164:1–81. https://doi.org/10.1016/j.pharmthera.2016.03.019
Fang J, Fang D, Silver PB et al (2010) The role of TLR2, TRL3, TRL4, and TRL9 signaling in the pathogenesis of autoimmune disease in a retinal autoimmunity model. Invest Ophthalmol Vis Sci 51(6):3092–3099. https://doi.org/10.1167/iovs.09-4754
Takeda K, Akira S (2007) Toll-like receptors. Curr Protoc Immunol 14(14):12. https://doi.org/10.1002/0471142735.im1412s109
Kawai T, Akira S (2007) TLR signaling. Semin Immunol 19(1):24–32. https://doi.org/10.1016/j.smim.2006.12.004
Akashi-Takamura S, Miyake K (2006) Toll-like receptors (TLRs) and immune disorders. J Infect Chemother 12:233–240. https://doi.org/10.1007/s10156-006-0477-4
Tarkowski A, Bjersing J, Shestakov A, Bokarewa MI (2010) Resistin competes with lipopolysaccharide for binding to toll-like receptor 4. J Cell Mol Med 14(6b):1419–1431. https://doi.org/10.1111/j.1582-4934.2009.00899.x
Bertolani C, Sancho-Bru P, Failli P et al (2006) Resistin as an intrahepatic cytokine: overexpression during chronic injury and induction of proinflammatory actions in hepatic stellate cells. Am J Pathol 169(6):2042–2053. https://doi.org/10.2353/ajpath.2006.060081
Holcomb IN, Kabakoff RC, Chan B et al (2000) FIZZ1, a novel cysteine-rich secreted protein associated with pulmonary inflammation, defines a new gene family. Embo j 19(15):4046–4055. https://doi.org/10.1093/emboj/19.15.4046
Senolt L, Housa D, Vernerova Z et al (2007) Resistin in rheumatoid arthritis synovial tissue, synovial fluid and serum. Ann Rheum Dis 66(4):458–463. https://doi.org/10.1136/ard.2006.054734
Axelsson J, Bergsten A, Qureshi AR et al (2006) Elevated resistin levels in chronic kidney disease are associated with decreased glomerular filtration rate and inflammation, but not with insulin resistance. Kidney Int 69(3):596–604. https://doi.org/10.1038/sj.ki.5000089
Yagmur E, Trautwein C, Gressner AM, Tacke F (2006) Resistin serum levels are associated with insulin resistance, disease severity, clinical complications, and prognosis in patients with chronic liver diseases. Am J Gastroenterol 101(6):1244–1252. https://doi.org/10.1111/j.1572-0241.2006.00543.x
Shiota A, Shimabukuro M, Fukuda D et al (2012) Telmisartan ameliorates insulin sensitivity by activating the AMPK/SIRT1 pathway in skeletal muscle of obese db/db mice. Cardiovasc Diabetol 11(139). https://doi.org/10.1186/1475-2840-11-139
Mendes KL, Lelis DF, Freitas DF et al (2021) Acute oral treatment with resveratrol and Lactococcus Lactis Subsp. Lactis decrease body weight and improve liver proinflammatory markers in C57BL/6 mice. Mol Biol Rep 48(2):1725–1734. https://doi.org/10.1007/s11033-021-06190-7
Ribeiro NG, Dos Santos FR, Oliveira JR et al (2021) Hepatotoxic Effect of Lafoensia pacari A. St. Hil. (Lythraceae) on a Diet-Induced Obese Mice Model. Protein Pept Lett 28(7):781–787. https://doi.org/10.2174/0929866528666210127151803
Hübscher SG (2006) Histological assessment of non-alcoholic fatty liver disease. Histopathology 49(5):450–465. https://doi.org/10.1111/j.1365-2559.2006.02416.x
Livak KJ, Schmittgen TD (2001) Analysis of relative gene expression data using realtime quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 25(4):402–408. https://doi.org/10.1006/meth.2001.1262
Takahashi Y, Sugimoto K, Inui H, Fukusato T (2015) Current pharmacological therapies for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. World J Gastroenterol 21(13):3777–3785. https://doi.org/10.3748/wjg.v21.i13.3777
Gitto S, Vitale G, Villa E, Andreone P (2015) Treatment of nonalcoholic steatohepatitis in adults: present and future. Gastroenterol Res Pract 2015:732870. https://doi.org/10.1155/2015/732870
Duseja A, Singh SP, Saraswat VA et al (2015) Non-alcoholic Fatty Liver Disease and Metabolic Syndrome-Position Paper of the Indian National Association for the Study of the Liver, Endocrine Society of India, Indian College of Cardiology and Indian Society of Gastroenterology. J Clin Exp Hepatol 5(1):51–68. https://doi.org/10.1016/j.jceh.2015.02.006
Oliveira Andrade JM, Paraiso AF, Garcia ZM et al (2014) Cross talk between angiotensin-(1-7)/Mas axis and sirtuins in adipose tissue and metabolism of high-fat feed mice. Peptides 55:158–165. https://doi.org/10.1016/j.peptides.2014.03.006
Pereira RM, dos Santos RA, da Costa Dias FL, Teixeira MM, Simo Ese Silva AC (2009) Renin-angiotensin system in the pathogenesis of liver fibrosis. World J Gastroenterol 15(21):2579–2586. https://doi.org/10.3748/wjg.15.2579
Moreira de Macedo S, Guimaraes TA, Feltenberger JD, Sousa Santos SH (2014) The role of renin-angiotensin system modulation on treatment and prevention of liver diseases. Peptides 62:189–196. https://doi.org/10.1016/j.peptides.2014.10.005
Koplay M, Sivri M, Erdogan H, Nayman A (2015) Importance of imaging and recent developments in diagnosis of nonalcoholic fatty liver disease. World J Hepatol 7(5):769–776. https://doi.org/10.4254/wjh.v7.i5.769
Santos SH and Simoes e Silva AC (2014) The therapeutic role of Renin-Angiotensin System blockers in obesity- related renal disorders. Curr Clin Pharmacol 9(1):2-9. https://doi.org/10.2174/15748847112079990050.
Liao AH, Ma WC, Wu MF (2013) Evaluation of ultrasound combined with chitosan for the control of weight and local fat in mice. Ultrasound Med Biol 39(10):1794–1803. https://doi.org/10.1016/j.ultrasmedbio.2013.04.025
Lessa AS, Paredes BD, Dias JV et al (2010) Ultrasound imaging in an experimental model of fatty liver disease and cirrhosis in rats. BMC Vet Res 6:6. https://doi.org/10.1186/1746-6148-6-6
Kudo H, Yata Y, Takahara T et al (2009) Telmisartan attenuates progression of steatohepatitis in mice: role of hepatic macrophage infiltration and effects on adipose tissue. Liver Int 29(7):988–996. https://doi.org/10.1111/j.1478-3231.2009.02006.x
Kuk JL, Katzmarzyk PT, Nichaman MZ, Church TS, Blair SN, Ross R (2006) Visceral fat is an independent predictor of all-cause mortality in men. Obesity (Silver Spring) 14(2):336–341. https://doi.org/10.1038/oby.2006.43
Rocha VZ, Libby P (2009) Obesity, inflammation, and atherosclerosis. Nat Rev Cardiol 6(6):399–409. https://doi.org/10.1038/nrcardio.2009.55
Santiago NM, Guimaraes PS, Sirvente RA et al (2010) Lifetime overproduction of circulating Angiotensin-(1-7) attenuates deoxycorticosterone acetate-salt hypertension-induced cardiac dysfunction and remodeling. Hypertension 55(4):889–896. https://doi.org/10.1161/HYPERTENSIONAHA.110.149815
Santos SH, Andrade JM, Fernandes LR et al (2013) Oral Angiotensin-(1-7) prevented obesity and hepatic inflammation by inhibition of resistin/TLR4/MAPK/NF-kappaB in rats fed with high-fat diet. Peptides 46:47–52. https://doi.org/10.1016/j.peptides.2013.05.010
Miura K, Seki E, Ohnishi H, Brenner DA (2010) Role of toll-like receptors and their downstream molecules in the development of nonalcoholic Fatty liver disease. Gastroenterol Res Pract 2010:362847. https://doi.org/10.1155/2010/362847
Alqarni I, Bassiouni YA, Badr AM, Ali RA (2019) Telmisartan and/or chlorogenic acid attenuates fructose-induced non- alcoholic fatty liver disease in rats: Implications of cross-talk between angiotensin, the sphingosine kinase/sphingoine-1-phosphate pathway, and TLR4 receptors. Biochem Pharmacol 164:252–262. https://doi.org/10.1016/j.bcp.2019.04.018
Georgescu EF, Ionescu R, Niculescu M, Mogoanta L, Vancica L (2009) Angiotensin-receptor blockers as therapy for mild-to-moderate hypertension-associated non-alcoholic steatohepatitis. World J Gastroenterol 15(8):942–954. https://doi.org/10.3748/wjg.15.942
Yi ET, Liu RX, Wen Y, Yin CH (2012) Telmisartan attenuates hepatic fibrosis in bile duct-ligated rats. Acta Pharmacol Sin 33(12):1518–1524. https://doi.org/10.1038/aps.2012.115
Cynis H, Kehlen A, Haegele M et al (2013) Inhibition of Glutaminyl Cyclases alleviates CCL2-mediated inflammation of non-alcoholic fatty liver disease in mice. Int J Exp Pathol 94(3):217–225. https://doi.org/10.1111/iep.12020
Nakagami H, Kiomy Osako M, Nakagami F et al (2010) Prevention and regression of non-alcoholic steatohepatitis (NASH) in a rat model by metabosartan, telmisartan. Int J Mol Med 26(4):477–481. https://doi.org/10.3892/ijmm_00000488
Tamaki Y, Nakade Y, Yamauchi T et al (2013) Angiotensin II type 1 receptor antagonist prevents hepatic carcinoma in rats with nonalcoholic steatohepatitis. J Gastroenterol 48(4):491–503. https://doi.org/10.1007/s00535-012-0651-7
Mario EG, Santos SH, Ferreira AV, Bader M, Santos RA, Botion LM (2012) Angiotensin-(1-7) Mas-receptor deficiency decreases peroxisome proliferator-activated receptor gamma expression in adipocytes. Peptides 33(1):174–177. https://doi.org/10.1016/j.peptides.2011.11.014
Ueda S, Masumori-Maemoto S, Ashino K et al (2000) Angiotensin-(1-7) attenuates vasoconstriction evoked by angiotensin II but not by noradrenaline in man. Hypertension 35(4):998–1001. https://doi.org/10.1161/01.hyp.35.4.998
Marui N, Offermann MK, Swerlick R et al (1993) Vascular cell adhesion molecule-1 (VCAM-1) gene transcription and expression are regulated through an antioxidant-sensitive mechanism in human vascular endothelial cells. J Clin Invest 92(4):1866–1874. https://doi.org/10.1172/JCI116778
Acknowledgements
We thank Centro Universitário FIPMoc (Montes Claros, Minas Gerais, Brazil) for supporting the ultrasound analysis. This swork was partially supported by the Coordenadoria de Aperfeiçoamento do Pessoal de Nível Superior (CAPES) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação de Amparo a Pesquisa do Estado de Minas Gerais (FAPEMIG).
Funding
Coordenadoria de Aperfeiçoamento do Pessoal de Nível Superior (CAPES). Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). Fundação de Amparo a Pesquisa do Estado de Minas Gerais (FAPEMIG).
Author information
Authors and Affiliations
Contributions
Conception, design, acquisition of data, analysis and interpretation of data, and write the manuscript: LMAB, DFF, ASM, AFP, and BVC: Luciana Mendes Araújo Borém, Daniela Fernanda de Freitas, Amanda Souto Machado, Alanna Fernandes Paraíso, and Bruna Viana Caldas; writing and critical review of the manuscript: João Felício Rodrigues Neto, Juliana Pinto Lima, André Luiz Sena Guimarães, and Alfredo Maurício Batista de Paula; conception, design, analysis, and interpretation of the data and writing of the manuscript: Sérgio Henrique Sousa Santos. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The animal studies were previously approved under number: 022/2012 by the ethical committee CEEBEA - Unimontes.
Consent for publication
The authors approved the publication process conducted by the corresponding author.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Borém, L.M.A., Freitas, D.F., Machado, A.S. et al. Angiotensin II type 1 receptor (AT1) blockade by Telmisartan attenuates hepatic steatosis in high-fat fed mice reducing Resistin, TRL4, and Myd88 expression. Egypt Liver Journal 12, 55 (2022). https://doi.org/10.1186/s43066-022-00216-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-022-00216-w