
Abstract
Background
Methotrexate (MTX) is well known as the first-line therapy for rheumatoid arthritis (RA) patients. Its prolonged usage necessitates frequent assessing for adverse impacts, most importantly hepatotoxicity. Since there are no set standards for verifying liver damage in RA patients; transient elastography (TE) is emerged as a non-intrusive technique for identifying and evaluating liver fibrosis, alongside with serum procollagen III amino terminus propeptide (PIIINP). The objective of this study is to investigate liver fibrosis in 60 patients with RA patients on MTX therapy and 30 healthy individuals by TE and PIIINP, in addition, to recognize the prognostic indicators for liver fibrosis.
Results
This study compared 60 adult RA patients who had been on MTX for at least 1 year to 30 matched age and sex heathy individuals. Liver fibrosis was measured using TE and PIIINP. A cutoff point of 7.1 kPa was declared abnormal, suggesting substantial liver fibrosis, while PIIINP > 170 ng/ml indicating elevated PIIINP levels. Based on TE results, liver fibrosis was reported in 20 patients (33.3%) with 14 patients (23.3%) who had significant liver fibrosis, 4 patients (6.7%) had advanced liver fibrosis, and 2 patients (3.3%) had liver cirrhosis. Meanwhile, five of the controls had mild liver fibrosis with highly statistically significant difference between patients and controls. The patient group had significantly higher level of PIIINP when compared to the healthy group with a specificity and sensitivity for detecting liver fibrosis of 85% and 82.5%, respectively.
Conclusions
MTX usage in RA patients was correlated with an overall increase in liver fibrosis. Cumulative dosage of MTX, the presence of fatty liver and elevated serum PIIINP levels are all significant predictors of liver stiffness in RA. TE is organ specific and could be helpful in assessing true liver status rather than PIIINP level which is not organ specific. TE is superior to serum PIIINP and is recommended as a routine investigation for RA patients on MTX therapy particularly those with fatty liver.
Similar content being viewed by others


Background
Methotrexate (MTX) was used as a first-line medication for treating rheumatoid arthritis (RA) for many years [1]. Since the early 1970s, MTX-induced hepatic damage has been a well-documented phenomenon that has been extensively studied, with most of the studies focusing on retrospective cohorts [2, 3].
As a matter of fact, histological abnormalities are not consistent well with conventional liver enzymes [4]. Although hepatic biopsy is still the most reliable method for staging hepatic fibrosis, it poses significant hazards [5] and is associated with serious complications in more than 1% of patients [6, 7]. There is certainly a need for a valid, accurate, and reliable non-intrusive assessment tool to identify early cases with hepatic fibrosis [8]. Transient elastography (TE) or fibroscan, a non-invasive approach, had been identified in numerous chronic hepatic disorders as an alternate to hepatic biopsy [9,10,11] and associated enormously with histological result [12,13,14].
Furthermore, it has been suggested that assessing amino terminus levels of type III procollagen (PIIINP) is a useful diagnostic modality for ongoing process of hepatic fibrosis, which may avoid liver biopsies. The vast majority of studies trials and published recommendations regarding its application have been carried out on patients with psoriasis and psoriatic arthritis with a little evidence in RA [15].
The main objective of this work was to determine the frequency of hepatic fibrosis in RA patients treated via MTX by TE and PIIINP, in addition, to recognize the prognostic indicators for liver fibrosis.
Methods
Patients: This study involved 60 patients diagnosed according to 2010 ACR/EULAR classification criteria for RA [16], matched to 30 healthy individuals by age and sex. Patients recruited were either inpatients or outpatients at the Department of Rheumatology and Rehabilitation, Minia University Hospital, between February 2020 and May 2021. Patients were considered eligible if they were over eighteen and had been receiving MTX treatment for at least 1 year. Exclusion was done if there were one or more of the following: current or previous liver disease, congestive heart failure, diabetes mellitus, alcohol intake, malignancy, or use of leflunomide or sulfasalazine. An informed consent was obtained from all participants and approval was obtained from the local research ethics committee (No. 386:1/2020).
Clinical evaluation: Each patient had a full history taking and thorough comprehensive clinical assessment. Examination of joint tenderness was performed by Ritchie articular index [17]. Body weight and height were measured for both patients and controls to calculate the body mass index (BMI). Special consideration was given to the duration of MTX therapy, the precise dose of MTX to calculate the cumulative dose, and the course and form of MTX therapy.
Disease Activity Assessment: Activity of RA was scored using disease activity score 28 (DAS 28-ESR) [18].
Investigations: Complete blood count, 1st-hour erythrocyte sedimentation rate, rheumatoid factor by Latex fixation, serum AST and ALT, total and direct bilirubin, serum albumin, serum gamma glutamyl transferase level, alkaline phosphatase, prothrombin time, serum creatinine, and blood urea. Viral markers for hepatitis B and C (HBsAg, HBcAb, and HCVAb) were performed to exclude cases with hepatitis. Serum PIIINP was measured using the standard ELISA method. A serum level of PIIINP > 170 ng/ml was considered elevated [19].
Abdominal ultrasonography: Abdominal conventional ultrasonography was carried out to all participants to assess liver structure and presence or absence of portal hypertension. Abdominal ultrasonography was performed using ultrasound device Aplio 500 system (Toshiba, Tokyo, Japan) using B-mode and Doppler ultrasonography to evaluate liver structure and portal hypertension. Assessment of portal hypertension was based on assessment of the portal vein caliber, hepatopetal unidirectional flow, velocity, preserved or disrupted pulsatility, splenomegaly, or presence of ascites.
Transient elastography: This was performed by a consultant radiologist with 20 years of experience in ultrasonography. All patients and controls underwent liver stiffness measurement via TE using the Aplio 500 ultrasound system (Toshiba, Tokyo, Japan), which measures the amount of hepatic stiffness between 25 and 65 mmbelow the skin`s surface in the volume of a cylinder that is 1 cm broad and 4 cm long. The examination was performed in the right lobe of the liver in an intercostal space in the midaxillary line, after at least 6 h fasting, while each subject lay supine with his right arm in full abduction and breathing normally, with holding the breath for few seconds during the acquisition. The vibration wave is generated by the using the Extra Large (XL) probe, 2.5 MHz, and a gentle “flick” is felt by the patient each time. The transducer was placed perpendicular to the skin, and the region of interest (ROI) was set between 25 and 65 mm from the surface. Ten readings are taken at the same setting, and the median of these readings was considered to determine the stage. Significant fibrosis, severe fibrosis, and cirrhosis are classified using cutoffs more than or equal to 7.1, 9.5, and 12.5 kPa, respectively [20].
Statistical analysis: Data were analyzed using Statistical Package for the Social Sciences software (SPSS) version 26. The data were presented as numbers, percentage, or mean, range, and standard deviations. Comparison between groups was done by independent sample t test and Chi-square test. Correlation was done using Spearman correlation coefficient. A stepwise logistic regression analysis was carried out to identify predictors of hepatic fibrosis. Additionally, the serum PIIINP's sensitivity, specificity, accuracy, negative predictive value (NPV), and positive predictive value (PPV) were determined.
Results
Among the 60 studied patients, there were 51 females (85%) and 9 males (15%). Their age ranged between 21 and 65 years with a mean of 46.46 ± 11.97 years versus 43.40 ± 14.18 years of the control (p = 0.285). The mean age of disease onset was 39.96 ± 11.32 (ranging from 19 to 61 years), and the mean duration of the disease was 6.50 ± 5.51 years ranging from 1 to 25 years. BMI of RA patients ranged from 19.47 to 38.95 kg/m2 with a mean of 25.68 ± 4.48 versus 25.49 ± 4.88 in the control group.
All RA patients were treated with MTX for at least 1 year. The cumulative dose of MTX ranged from 600 to 12,960 mg with a mean of 3,199.77 ± 2,600.57 mg, and the duration of MTX intake ranged from 1 to 18 years with a mean of 3.80 ± 3.22 years. Fifty patients (83.3%) were receiving MTX through the injection form while 10 patients (16.7%) were receiving it via both injection and oral routes. Its course was continuous in 44 patients (73.3%) and intermittent in 16 patients (26.7%). Fifty-five patients (91.7%) were receiving folic acid, 45 patients (75%) were taking antimalarials, and 12 patients (20%) were on oral corticosteroids at the time of the study.
Abdominal ultrasonography of the RA patients showed fatty liver in 18 patients (30%) with accompanied mild hepatomegaly in 10 patients (16.7%), while cirrhotic liver was detected in only 1 patient (1.7%) with no evidence of portal hypertension in any studied cases.
Based on TE assessment and as it is illustrated in Table 1, liver fibrosis was reported in 20 patients (33.3%) with 14 patients (23.3%) who had significant liver fibrosis (Fig. 1), 4 patients (6.7%) had advanced liver fibrosis (Fig. 2), and 2 patients (3.3%) had liver cirrhosis (Fig. 3).

Transient elastography showing increased liver tissue stiffness in patient with significant liver fibrosis. The patient measures about 7.5 kPa denoting mild fibrosis

Transient elastography showing increased liver tissue stiffness in patient with advanced liver fibrosis. The patient measures about 10 kPa denoting severe stiffness

Transient elastography showing increased liver tissue stiffness in cirrhotic patient. The patient measures about 15 kPa denoting cirrhosis
RA patients who had hepatic fibrosis were significantly older, had a longer disease duration, a higher articular index, and more active disease (p < 0.001) than RA patients without hepatic fibrosis. In addition, higher BMI patients tend to have more advanced hepatic fibrosis. Cumulative dose of MTX in the fibrosis group was significantly higher with longer duration (p < 0.001) than RA patients without hepatic fibrosis, with no significant difference between the two groups regarding age at onset or number of swollen joints (Table 2).
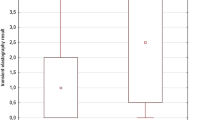
There was no statistically significant difference between the two groups regarding laboratory parameters, except for the serum AST level and serum PIIINP. Moreover, 16 patients (80%) of RA patients who had liver fibrosis were positive for serum PIIINP, while only 8 patients (20%) out of 40 RA patients without hepatic fibrosis were positive for serum PIIINP. The mean level of serum PIIINP was statistically significantly higher (131.69 ± 101.39) ng/ml than mean level of the controls (82.30 ± 76.73) ng/ml (p < 0.05).
There was a statistically significant correlation between the level of PIIINP and body weight (r = 0.294; p = 0.023), duration of the disease (r = 0.646; p < 0.001), duration of MTX therapy (r = 0.720; p < 0.001), cumulative dosage of MTX (r = 0.708; p < 0.001), and disease activity (r = 0.527; p < 0.001) (Table 3).
Table 4 demonstrates a positive statistically significant correlation between value of TE, DAS 28-ESR (r = 0.396, p < 0.001), AST level (r = 0.281, p < 0.05), PIIINP level (r = 0.700, p < 0.001), elevated PIIINP > 170 ng/ml (r = 0.634, p < 0.001), fatty liver (r = 0.536, p < 0.001), MTX cumulative dose (r = 0.714, p < 0.001), MTX duration (r = 0.731, p < 0.001), and disease duration (r = 0.600, p < 0.001).
There was no significant correlation between value of TE, ALT level (r = 0.146, p = 0.266), serum albumin level (r =− 0.025, p = 0.849), BMI (r = 0.173, p = 0.186), age (r = 0.145, p = 0.287), sex (r = − 0.225, p = 0.083), age at onset (r = − 0.139, p = 0.291), antimalarial intake (r = − 0.045, p = 0.736), corticosteroid intake (r = 0.152, p = 0.247), and folic acid intake (r = − 0.229, p = 0.078).
When we applied stepwise logistic regression analysis, cumulative dose of MTX was the highest significant predictor (p < 0.001) of hepatic fibrosis, followed by fatty liver detected by abdominal sonography (p < 0.001), followed by increased serum PIIINP (p < 0.001) (Table 5). Neither the duration of MTX nor the duration of the disease was predictive of liver fibrosis.
The ROC curve analysis suggests that PIIINP levels above 170 ng/mL have a relatively high sensitivity (85%) for detecting liver fibrosis risk, while maintaining a reasonably good specificity (82.5%). The PPV and NPV values indicate that a positive test result is moderately predictive of liver fibrosis risk, while a negative result provides a strong indication of the absence of risk. The overall accuracy of 83.33% suggests that the test performs well in correctly classifying individuals based on the chosen cutoff value (Table 6, Fig. 4).

ROC curve of serum PIIINP level for prediction of liver fibrosis risk. ROC curve of serum PIIINP level with the area under the curve (AUC) of 0.89 where a cut-off PIIINP value of > 170 ng/ml provided 85% sensitivity and 82.5% specificity for predicting liver fibrosis
Discussion
MTX is the most often prescribed therapy for RA because of its low cost and effectiveness [21]. In comparison with other DMARDs, it is a long-term safe and effective treatment [22]. One of the most serious adverse effects is hepatotoxicity which is monitored in most cases by serum aminotransferase levels, which could, but does not always, accurately represent the degree of hepatic damage. Liver fibrosis can progress silently, often without a corresponding increase in serum aminotransferase levels [23, 24]. However, there is a risk of morbidity and even mortality with liver biopsy, which highlights the need for innovative, less invasive methods [25].
TE, a non-invasive approach for evaluating liver stiffness, is commonly used to identify liver fibrosis, particularly in individuals with viral hepatitis [26]. It is comparable to a liver biopsy in a number of studies, and it has a somewhat higher specificity and sensitivity for fibrosis detection [26, 27]. An indicator of the severity of the fibrosis process in humans is assessment of serum PIIINP [15, 28,29,30]. Its value was found to evaluate liver toxicity of methotrexate in psoriatic patients; however, just a few numbers of studies have been conducted on RA patients [31].
The objective of this work was to determine the frequency of liver fibrosis in RA patients on MTX by both TE and PIIINP, as well as the prognostic indicators for liver fibrosis.
Our study included 60 adult RA patients who all treated with MTX, and 30 age- and sex-matched healthy individuals. The presence of hepatic fibrosis is well-documented in some of RA patients in contrast to general population. In the present work, hepatic fibrosis was detected in 20 RA patients (33.3%) compared with only 5 controls (16.7%) using a 7.1 kPa cutoff. However, in other studies, the prevalence of hepatic fibrosis in RA patients was lower, ranging from 16 to 26.8% [20, 31]. Furthermore, the average hepatic fibrosis as determined by TE was 6.83 ± 2.33 kPa in RA patients and 4.95 ± 2.09 kPa in the healthy group (p < 0.001) which is higher compared with other studies. Kumar et al. reported a mean liver stiffness of 4.8 kPa in the RA patients and 4.7 kPa in the healthy individuals [32]. Another study by Laharie et al., which included 149 RA patients, reported the mean FibroScan score was 4.3 kPa [33]. Other study which evaluated liver affection in patients with HCV-related vasculitis using the same cutoff value with 38.5% had severe cases of hepatic fibrosis, and 42.3% had mild-to-moderate cases [34].
The primary reason for this disparity is most likely that other studies excluded obesity based on BMI more than 30 while we did not. Other reasons for such variability that Fibroscan validation studies do not follow the rigorous requirements for applicability as there is variation according to probe position, beside it is an operator dependent [35]. Additionally, measurement disparity between using different probes as the Medium (M) and XL probes, as there might be a basic technological difference, as the two probes differ significantly in terms of energy and ultrasonic frequency [36].
Measurement of BMI in our series is also comparable with other reports, it was ranged from 19.47 to 38.95 kg/m2 with a mean of 25.68 ± 4.48 kg/m2 in the patient`s group versus 25.49 ± 4.88 kg/m2 in the control group. Our results came in accordance with Bafna et al. results who studied 75 RA patients on MTX to evaluate the prevalence of hepatic fibrosis and found that the mean of BMI was 24.8 ± 3.9 kg/m2 [20]. Obesity is a major predictor of advanced liver fibrosis or cirrhosis, which is linked to more than threefold increase in all causes of liver-related mortality [37, 38]. Liver fibrosis advances in obese individuals due to increased adiposity and insulin resistance. It is believed that a profibrotic milieu in the liver is fostered by a rise in the number of dead hepatocytes, an increase in reactive oxygen radicals, and changes in the production of adipokines and cytokines [39].
In this study, serum PIIINP was ranging from 22.0 to 436.0 ng/ml with a mean of 131.69 ± 101.39 ng/ml in RA patients' group which was significantly higher than healthy individuals (82.30 ± 76.73 ng/ml). Our result is in accordance with Amer et al. who conducted a research on 30 RA patients receiving alternative treatments and 60 RA patients receiving MTX in order to assess the validity of PIIINP in the detection of hepatic fibrosis brought on by long-term MTX therapy and found that mean PIIINP on MTX group was 120 ng/ml with the same cutoff point which is more than 170 ng/ml [19]. Our results also showed that serum PIIINP was elevated above threshold of fibrosis (170 ng/ml) in 24 patients (40%), on agreement with Frankowski et al. who studied 96 RA patients aiming to measure hepatic fibrosis in RA patients by evaluating non-invasive diagnostic techniques and discovered that PIIINP was elevated in 44.8% of their patients [25].
In the present work and based on stepwise logistic regression, the cumulative dosage of MTX, fatty liver, and serum PIIINP > 170 ng/ml was found to be predictor factors for hepatic fibrosis on agreement with Lertnawapan et al. who found the cumulative dosage of MTX and fatty liver as predictors of liver fibrosis [40], Arena et al. who found cumulative dose of MTX as predictor of hepatic fibrosis [23]. On the contrary, laharie et al. noticed no relation between the cumulative dosage of MTX and TE on regression analysis [33].
The current study evaluated the sensitivity and specificity of a single serum PIIINP measurement in patients receiving MTX therapy, with results of 85.0% and 82.5%, respectively. These values are a little higher than those reported by Maybury et al., who evaluated the same parameters and found rates of 74% and 77%, respectively [41], PIIINP is not organ specific, and RA activity as well as other variables may affect its reading.
This study has some limitations: Firstly, exclusion of high BMI could not be done as 43.3% of our patients had BMI above normal value (≥ 25 kg/m2) and obesity is one of the factors that increases liver stiffness, secondly; the cutoff point for measurement of hepatic fibrosis on elastography was not unique in whole studies.
Conclusions
Transient elastography and PIIINP are recommended for the routine investigations for RA patients on MTX therapy to detect liver fibrosis even if they are asymptomatic. Transient elastography is superior to PIIINP for evaluating the progress of the disease and the effectiveness of treatment. We recommend using of fibroscan as a monitoring for RA patients on MTX therapy, specifically patients with fatty liver. Better control of body weight and RA disease activity is necessary to reduce hepatic fibrosis risk in those patients.
Availability of data and materials
The data are available on request.
Abbreviations
- ACR:
-
American College of Rheumatology
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- DAS:
-
Disease activity score
- EULAR:
-
European alliance of associations for rheumatology
- kPa:
-
Kilopascal
- M:
-
Medium
- MTX:
-
Methotrexate
- NPV:
-
Negative predictive value
- PIIINP:
-
Serum procollagen III amino terminal propeptide
- PPV:
-
Positive predictive value
- RA:
-
Rheumatoid arthritis
- ROI:
-
Region of interest
- SPSS:
-
Statistical Package for the Social Sciences
- TE:
-
Transient elastography
- XL:
-
Extra large
References
Friedman B, Cronstein B (2019) Methotrexate mechanism in treatment of rheumatoid arthritis. Joint Bone Spine 86(3):301–307
Kremer JM, Lee JK (1986) The safety and efficacy of the use of methotrexate in long-term therapy for rheumatoid arthritis. Arthritis Rheum 29(7):822–831
Lanse SB, Arnold GL, Gowans JD, Kaplan MM (1985) Low incidence of hepatotoxicity associated with long-term, low-dose oral methotrexate in treatment of refractory psoriasis, psoriatic arthritis, and rheumatoid arthritis. An acceptable risk/benefit ratio. Dig Dis Sci 30(2):104–109
Yoneda M, Imajo K, Eguchi Y, Fujii H, Sumida Y, Hyogo H et al (2013) Noninvasive scoring systems in patients with nonalcoholic fatty liver disease with normal alanine aminotransferase levels. J Gastroenterol 48(9):1051–1060
West J, Card TR (2010) Reduced mortality rates following elective percutaneous liver biopsies. Gastroenterology 139(4):1230–1237
Kremer JM, Alarcón GS, Lightfoot RW Jr, Willkens RF, Furst DE, Williams HJ et al (1994) Methotrexate for rheumatoid arthritis. Suggested guidelines for monitoring liver toxicity. American College of Rheumatology. Arthritis Rheum 37(3):316–328
Campbell MS, Reddy KR (2004) The evolving role of liver biopsy. Aliment Pharmacol Ther 20(3):249–259
Bravo AA, Sheth SG, Chopra S (2001) Liver biopsy. N Engl J Med 344(7):495–500
Arena U, Vizzutti F, Abraldes JG, Corti G, Stasi C, Moscarella S et al (2008) Reliability of transient elastography for the diagnosis of advanced fibrosis in chronic hepatitis C. Gut 57(9):1288–1293
Nahon P, Kettaneh A, Tengher-Barna I, Ziol M, de Lédinghen V, Douvin C et al (2008) Assessment of liver fibrosis using transient elastography in patients with alcoholic liver disease. J Hepatol 49(6):1062–1068
Hashemi SA, Alavian SM, Gholami-Fesharaki M (2016) Assessment of transient elastography (FibroScan) for diagnosis of fibrosis in non-alcoholic fatty liver disease: a systematic review and meta-analysis. Caspian J Intern Med 7(4):242–252
Castéra L, Vergniol J, Foucher J, Le Bail B, Chanteloup E, Haaser M et al (2005) Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology 128(2):343–350
Foucher J, Chanteloup E, Vergniol J, Castéra L, Le Bail B, Adhoute X et al (2006) Diagnosis of cirrhosis by transient elastography (FibroScan): a prospective study. Gut 55(3):403–408
Sandrin L, Fourquet B, Hasquenoph JM, Yon S, Fournier C, Mal F et al (2003) Transient elastography: a new noninvasive method for assessment of hepatic fibrosis. Ultrasound Med Biol 29(12):1705–1713
Khan S, Subedi D, Chowdhury MM (2006) Use of amino terminal type III procollagen peptide (P3NP) assay in methotrexate therapy for psoriasis. Postgrad Med J 82(967):353–354
Aletaha D, Neogi T, Silman A, Funovits J, Felson D, Bingham Iii C et al (2010) Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheum 62(9):69–81
Ritchie DM, Boyle JA, McInnes JM, Jasani MK, Dalakos TG, Grieveson P et al (1968) Clinical studies with an articular index for the assessment of joint tenderness in patients with rheumatoid arthritis. Q J Med 37(147):393–406
Prevoo ML, Van’t Hof MA, Kuper HH, Van Leeuwen MA, Van De Putte LB, Van Riel PL (1995) Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum 38(1):44–48
Amer H, Ghareeb H, Mohamed NL, El-Azizi NO, Mansour AM (2020) Procollagen III amino terminal propeptide (PIIINP) A noninvasive marker of methotrexate induced liver fibrosis in Rheumatoid arthritis patients. QJM Int J Med 113(1):12–18
Bafna P, Sahoo R, Hazarika K, Manoj M, Rungta S, Wakhlu A (2021) Prevalence of liver fibrosis by Fibroscan in patients on long-term methotrexate therapy for rheumatoid arthritis. Clin Rheumatol 40(9):05–13
Smolen JS, Landewé RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A et al (2020) EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis 79(6):685–699
El-Zorkany BK, Gamal SM, El-Mofty SA (2013) Frequency and causes of discontinuation of methotrexate in a cohort of Egyptian patients. Egypt Rheumatol 35(2):53–57
Arena U, Stasi C, Mannoni A, Benucci M, Maddali-Bongi S, Cammelli D et al (2012) Liver stiffness correlates with methotrexate cumulative dose in patients with rheumatoid arthritis. Dig Liver Dis 44(2):149–153
Erre GL, Cadoni ML, Meloni P, Castagna F, Mangoni AA, Piga M et al (2019) Methotrexate therapy is not associated with increased liver stiffness and significant liver fibrosis in rheumatoid arthritis patients: a cross-sectional con-trolled study with real-time two-dimensional shear wave elastography. Eur J Intern Med 69:57–63
Frankowski M, Swierkot J, Gomułkiewicz M, Korman L, Skoczyńska M, Starba A (2022) Usefulness of noninvasive diagnostic procedures for assessment of methotrexate hepatotoxicity in patients with rheumatoid arthritis. Rheumatol Int 42(4):631–638
European Association for Study of Liver; Asociacion Latinoamericana para el Estudio del Higado (2015) EASL-ALEH clinical practice guidelines: non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol 63(1):237–264
Mikolasevic I, Orlic L, Franjic N, Hauser G, Stimac D, Milic S (2016) Transient elastography (FibroScan®) with controlled attenuation parameter in the assessment of liver steatosis and fibrosis in patients with nonalcoholic fatty liver disease—Where do we stand? World J Gastro-enterol 22(32):7236–7251
Zachariae H, Heickendorff L, Søgaard H (2001) The value of amino-terminal propeptide of type III procollagen in routine screening for methotrexate-induced liver fibrosis: a 10-year follow-up. Br J Dermatol 144(1):100–103
Chládek J, Šimková M, Vanečková J, Hroch M, Vávrová J, Hůlek P (2013) Assessment of methotrexate hepatotoxicity in psoriasis patients: a prospective evaluation of four serum fibrosis markers. J Eur Acad Dermatol Venereol 27(8):1007–1014
Lindsay K, Fraser AD, Layton A, Goodfield M, Gruss H, Gough A (2009) Liver fibrosis in patients with psoriasis and psoriatic arthritis on long-term, high cumulative dose methotrexate therapy. Rheumatology 48(5):569–572
van der Voort EAM, Wakkee M, Veldt-Kok P, Darwish Murad S, Nijsten T (2017) Enhanced liver fibrosis test in patients with psoriasis, psoriatic arthritis and rheumatoid arthritis: a cross-sectional comparison with procollagen-3 N-terminal peptide (P3NP). Br J Dermatol 176(6):1599–1606
Kumar A, Vasdev V, Manrai M, Bhayana A, Hegde A, Arjun MN et al (2018) Assessment of hepatic fibrosis in patients with rheumatoid arthritis on long-term methotrexate therapy using transient elastography. Indian J Rheumatol 13(4):246–251
Laharie D, Seneschal J, Schaeverbeke T, Doutre MS, Longy-Boursier M, Pellegrin JL et al (2010) Assessment of liver fibrosis with transient elastography and fibroTest in patients treated with methotrexate for chronic inflammatory diseases: a case-control study. J Hepatol 53(6):1035–1040
Shahin AA, Zayed HS, El Shazly RI, Said M (2014) Evaluation of the liver condition in chronic hepatitis C virus patients with and without vasculitis. Egypt Rheumatol 36:187–193
Ingiliz P, Chhay KP, Munteanu M, Lebray P, Ngo Y, Roulot D et al (2009) Applicability and variability of liver stiffness measurements according to probe position. World J Gastroenterol 15(27):3398–3404
Durango E, Dietrich C, Seitz HK, Kunz CU, Pomier-Layrargues GT, Duarte-Rojo A et al (2013) Direct comparison of the FibroScan XL and M probes for assessment of liver fibrosis in obese and nonobese patients. Hepat Med 4(5):43–52
Ekstedt M, Hagström H, Nasr P, Fredrikson M, Stål P, Kechagias S et al (2015) Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 61(5):1547–1554
Angulo P, Kleiner DE, Dam-Larsen S, Adams LA, Bjornsson ES, Charatcharoenwitthaya P et al (2015) Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 149(2):389–397
Chiang DJ, Pritchard MT, Nagy LE (2011) Obesity, diabetes mellitus, and liver fibrosis. Am J Physiol Gastrointest Liver Physiol 300(5):G697-702
Lertnawapan R, Chonprasertsuk S, Siramolpiwat S (2019) Association between cumulative methotrexate dose, non-invasive scoring system and hepatic fibrosis detected by Fibroscan in rheumatoid arthritis patients receiving methotrexate. Int J Rheum Dis 22(2):214–221
Maybury C, Samarasekera E, Douiri A, Barker J, Smith C (2014) Diagnostic accuracy of noninvasive markers of liver fibrosis in patients with psoriasis taking methotrexate: a systematic review and meta-analysis. Br J Dermatol 170(6):1237–1247
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
Rasha M Ghaleb designed the study and participating in writing the study. Doaa M Mohamed collected the clinical data. Ahmed Hamed analyzed the results. Zaki M Zaki interpreted the laboratory parameters. Nadia El Ameen performed abdominal ultasongraphy and fibroscan.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Scientific Ethical Committee of the faculty of medicine, Minia University, Minia, Egypt.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ghaleb, R.M., Mohamed, D.M., Zaki, Z.M. et al. Assessment of liver fibrosis by transient elastography and procollagen III amino terminal propeptide in rheumatoid arthritis patients treated with methotrexate. Egypt J Radiol Nucl Med 55, 147 (2024). https://doi.org/10.1186/s43055-024-01323-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01323-x