
Abstract
Background
Extensive research has been dedicated to exploring the neurobiological underpinnings of schizophrenia, yet there has been comparatively less emphasis on investigating specific markers associated with violent behaviors within this condition.
Aim of the study
This study aimed to compare gray matter thickness and volume and investigate clinical markers for assessing violence risk in schizophrenia.
Results
We enrolled a total of 36 participants, comprising 19 patients with a documented history of violent behaviors in schizophrenia and 17 patients with no such history. Schizophrenia patients with a history of violence exhibited a significant reduction in cortical thickness in the left caudal-middle-frontal gyrus (2.540 ± 0.146 mm) compared to those without such history (2.757 ± 0.126 mm) (P = 0.0301). Similarly, the cortical volume in the right middle temporal gyrus was decreased in patients with a history of violence (15.579 ± 8.790 mm3) compared to non-violent patients (29.941 ± 13.585 mm3) (P = 0.0071). ROC analysis demonstrated promising diagnostic efficiency, with an AUC of 0.876 for left caudal-middle-frontal gyrus thickness (P = 0.000) and 0.794 for right middle temporal gyrus volume (P = 0.003).
Conclusions
Our findings highlight brain cortical assessments as potential diagnostic biomarkers to identify individuals at risk of violent behavior within the schizophrenia population.
Similar content being viewed by others

Background
Schizophrenia is recognized as one of the most severe and prevalent psychiatric disorders worldwide, affecting approximately 1% of the population. This condition is characterized by disruptions in cognition, emotion, thinking, perception, and motor processes [1]. Notably, schizophrenia encompasses negative symptoms, including irritability, anger, resentment, verbal aggression, and other forms of violent behavior. These violent behaviors involve physical attacks on others, oneself, or objects [2]. Extensive research has indicated that prior instances of violent behavior represent a key and enduring risk factor for predicting hospitalization and future violent tendencies in individuals with various mental disorders [3, 4]. Violent behavior signifies an intent to harm or injure another person or damage property, a determination drawn from events preceding or following an act of aggression.
The human cerebral cortex, a thin and intricately folded sheet of gray matter with variable thickness (ranging from one to five millimeters) [5], plays a pivotal role in understanding the structure and function of the human brain when reconstructed from magnetic resonance (MR) images. While cortical thickness, serving as an indicator of cytoarchitectural integrity in specific brain regions, can be influenced by environmental factors in certain contexts [6], it is important to note that heritability studies suggest moderate to high genetic influence on individual variations in cortical thickness. Similarly, the genetic influence on cortical surface area and volume is complex and not uniformly determined [7]. Cortical volume, defined as the product of cortical thickness and surface area, adds another dimension to assessing cortical morphometry, potentially enhancing accuracy and sensitivity for detecting differences in brain structure [8].
In a relevant study, Kumari identified a negative correlation between impulsiveness and reduced orbitofrontal gray matter volume in patients with schizophrenia prone to repetitive violence [9]. However, correlations between brain cortical measurements and schizophrenia patients with a history of violence remain relatively unexplored. Some studies suggest possible biological distinctions between violent and non-violent schizophrenia patients, implying differential brain morphometric development. This study aimed to compare anatomical variations in brain cortical vertex and evaluate clinical factors in schizophrenia patients at risk of violence. A deeper understanding of these structural alterations and their functional implications could facilitate improved evaluation, prevention, and early intervention in cases with a heightened risk of violent behavior.
Methods
Population and study design
Nineteen patients (age range 22–47 years, 5 female, 14 male) diagnosed with schizophrenia and exhibiting violent behaviors (the violent group) were cross-sectionally and consecutively recruited from the inpatient and outpatient departments of our hospital between January 2017 and January 2019. Seventeen patients with schizophrenia (age range 14–50 years, 7 female, 10 male), matched for age and gender but with no history of violent behavior (the non-violent group), were also recruited during the same period for this study. All the participants were informed about the study and provided written informed consent before enrollment in the trial. The authors ensure that the work described has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments.
Inclusion criteria
The inclusion criteria of all patients were as follows:
-
1.
Age from 18 to 60 years.
-
2.
Right-handed.
-
3.
Diagnosis of schizophrenia by a senior psychiatrist with 10 years’ experience, according to the International Classification of Diseases Tenth Revision (ICD-10) criteria, with relevant data collected from medical records.
Exclusion criteria
The inclusion criteria of all patients were as follows:
-
1.
Presence of brain organic diseases.
-
2.
Medical disorders that have impaired neurocognitive functioning.
-
3.
A history of substance abuse or dependence.
-
4.
Contraindication to MRI (i.e., claustrophobia, patients with pace makers or metallic clips).
The following were applied to all patients
-
1.
Complete clinical history and personal history, which should include name, date of birth, sex, education level, and family history.
-
2.
Current medical history, including illness progression, treatment, age of onset, medication dosage.
-
3.
Types of schizophrenia are evaluated clinically through ICD-10 criteria by a senior psychiatrist with 10 years’ experience.
-
4.
The MOAS and PANSS scales were employed to assess violent behavior and Neuropsychiatric symptoms.
-
5.
Magnetic resonance imaging.
Neuropsychological assessments
All patients were assigned to two groups—the “violent group” (19 cases) and the “non-violent” group (17 cases)—based on the Modified Overt Aggression Scale (MOAS). The MOAS [10] records the forms of violence and their severity. It consists of four subscales of increasing severity: verbal attack, attack toward properties, self-attack, and physical attack toward people. Each subscale includes five items scored from 0 to 4; the final score is obtained by multiplying the scores of each subscale by their specific “weight” (1, 2, 3, and 4, respectively), then adding the four obtained values. In this study, patients with violent behavior were defined by the following factors: (1) a MOAS score > 4, and (2) having at least two instances of violent behavior in their case files.
Neuropsychiatric symptoms and their severity in patients with schizophrenia were evaluated using the Positive and Negative Syndrome Scale (PANSS). PANSS comprises the positive symptom scale (7 items), negative symptom scale (7 items), and general psychopathology scale (16 items), totaling up to 30 items in all.
MRI acquisition
The MRI images of the schizophrenia patients were acquired on a 3 Tesla (3T) MRI system utilizing an 8-channel phased array head coil (General Electrics 750 Discovery). A high-resolution 3D T1-weighted inversion-prepared sequence was acquired to assess the cortical thickness and volume. The time between filling out the psychiatric assessment scales and the MRI exam was within one week. The repetition time (TR) was 6.896 ms, the inversion time (TI) was 450 ms, the echo time (TE) was 2.992 ms, the flip angle (FA) was 8°, the field of view (FOV) was 100, the matrix was 256 × 256, the slice thickness was 1 mm, and the number of slices was 176. All images were inspected for clinically relevant abnormalities by a senior radiologist with 8-year experience.
Images processing and analysis
The 3D- T1WIs were processed using the FreeSurfer package 6.0.0 (http://surfer.nmr.mgh.harvard.edu), which uses a set of automated sequences to reconstruct the cortical surface of the entire brain. The measurements of the cortical surface included thickness, volume, and mean curvature. The whole process was completed by the command "-recon-all," including motion correction, skull stripping, segmentation of white matter, the creation of the pial and white/gray junction surfaces, the inflation of the folding surface plane, and topology correction [11]. Next, a manual method provided by FreeSurfer was used to correct any geometric inaccuracies. The cortical thickness at each point is the shortest distance between the pial surface and the white/gray junction. The surface was divided into separate cortical regions using an automated labeling approach, and the mean cortical thickness (in mm) and cortical volume (in mm3) were extracted for 34 bilateral Desikan-Killiany atlas regions [12].
A whole-brain comparative analysis of cortical thickness and volume between schizophrenia with and without violence was performed in FreeSurfer. Each subject's approved cortical thickness and volume maps were first registered to a standard spherical atlas. Then, the cortical surface maps were smoothed, and cortical thickness and volume maps were generated with several different kernel sizes. A general linear model (GLM) was used to examine the two groups' vertex-wise differences in cortical thickness and the relationship with the PANSS scores, controlling for gender and age. The cortical volume also used the GLM to examine the vertex-wise differences in the cortical volume of the two groups and the association with the PANSS scores, controlling for intracranial volume (ICV) and age. The right and left hemispheres were examined separately. A Monte Carlo null-z simulation with 10,000 iterations was used to correct for multiple comparisons. The statistical significance of the cortical thickness for the cluster-forming threshold (CFT) was defined as p < 0.01, and the cluster-wise probability (CWP) was set at p < 0.05 (two-tailed), while the CFT of the cortical volume was set at p < 0.001, and the CWP was p < 0.05 (two-tailed). The data underwent thorough analysis and interpretation by a highly skilled radiologist with 8 years of experience in the field.
Statistical analysis
The data analysis was conducted using the SPSS 22.0 version of statistical software. Sociodemographic data and factor scores were statistically described using the mean, standard deviation, constituent ratio (percentage), and frequency. A t-test was employed to detect statistical differences in age, chlorpromazine equivalents, age of onset, the PANSS scores and the MOAS scores between the violent and non-violent groups, and a chi-square test was utilized to assess statistical differences in categorical variables (i.e., sex, level of education, type of schizophrenia, family history) between the violent and non-violent groups. The ROC curve was used to evaluate the diagnostic efficiency of cortical thickness and volume. All charts and figures were generated using GraphPad PRISM 8.3.0 (GraphPad Software). All the results were adjusted with a significance level set at p < 0.05.
Results
The clinical characteristics of the patients in the two groups
Thirty-six patients (24 men and 12 women) diagnosed with schizophrenia, according to ICD-10 criteria, were included in the study. There were no statistical differences between the two groups regarding sociodemographic and clinical factors except for the chlorpromazine equivalents and MOAS scores (Table 1).
Whole-brain analysis of cortical thickness and volume between violent and non-violent groups
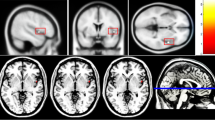
The cortical thickness of the left caudal middle frontal gyrus (lh_caudal-middle-frontal_thickness) showed a decrease in the violent group compared with that of the non-violent group (2.540 ± 0.146 mm vs. 2.757 ± 0.126 mm, Monte Carlo correction, CFT < 0.01, CWP < 0.05). The cortical volume of the right middle temporal gyrus (rh_middletemporal_volume) showed a decrease in the violent group (15.579 ± 8.790mm3 vs. 29.941 ± 13.585mm3, Monte Carlo correction, CFT < 0.001, CWP < 0.05) (Table 2; Figs. 1 and 2).

Differences in cortical thickness and volume in schizophrenia patients with/without violent tendencies. a A Cluster demonstrating decreased cortical thickness in the left caudal middle frontal gyrus among patients with violent tendencies compared to non-violent patients (Monte Carlo correction, CFT < 0.01, CWP < 0.05). b A Cluster indicating decreased cortical volume in the right middle temporal gyrus in patients exhibiting violence compared with non-violent patients (Monte Carlo correction, CFT < 0.01, CWP < 0.05). c Violin plots displaying the distribution of cortical thickness measurements in the left caudal middle frontal gyrus. d Violin plots depicting the distribution of cortical volume measurements in the right middle temporal gyrus. CFT cluster-forming threshold; CWP cluster-wise probability

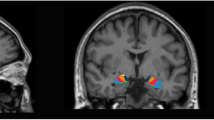
a A 16-year-old male patient clinically diagnosed with paranoid schizophrenia exhibited a MOAS score was 0. Axial 3D-T1WI maps revealed a cortical thickness measurement of 3.039 mm in the left caudal middle frontal gyrus (white arrows). b A 26-year-old female patient clinically diagnosed with undifferentiated schizophrenia presented with a MOAS score of 16. Axial 3D-T1WI maps displayed a thickness measurement of 2.306 mm in the left caudal middle frontal gyrus (white arrows). c A 44-year-old female patient clinically diagnosed with undifferentiated schizophrenia demonstrated a MOAS score of 0. Coronal 3D-T1WI maps depicted a cortical volume measurement of 47 mm3 in the right middle temporal gyrus (white arrows). d A 45-year-old male patient clinically diagnosed with undifferentiated schizophrenia had a MOAS score of 17. Coronal 3D-T1WI maps showed a cortical volume measurement of 7 mm3 in the right middle temporal gyrus (white arrows). MOAS, modified overt aggression scale; 3D-T1WI, three dimension T1 weighted imaging
Diagnostic role of cortical thickness and volume changes in violent/non-violent group patients
To assess the potential of cortical thickness and volume changes, particularly in the left caudal middle frontal gyrus thickness and the right middle temporal gyrus volume, as biomarkers for identifying violent patients within the schizophrenia cohort, ROC analysis was conducted on all schizophrenia patients. The ROC curve analysis demonstrated that the left caudal middle frontal gyrus thickness exhibited high diagnostic accuracy in distinguishing violent patients, with an impressive Area Under the Curve (AUC) of 0.876 (Fig. 3a). Notably, the optimal cutoff value for cortical thickness was determined to be 2.663 mm, with a sensitivity of 76.5% and specificity of 89.5%. Similarly, the ROC curve analysis for the right middle temporal gyrus volume accurately achieved an AUC of 0.794 (Fig. 3b). The optimal cutoff value for cortical volume was identified as 18.5mm3, with a sensitivity of 76.5% and specificity of 73.7%. (Table 3, Fig. 3).

The optimal cut-off point was calculated based on the ROC curve. a The ROC curve of the left caudal middle frontal gyrus thickness; b The ROC curve of the right middle temporal gyrus volume. ROC, receiver operating characteristic curve
Correlation analysis
No significant correlation was found between the PANSS sores and the whole brain thickness of the schizophrenia patients. However, the left supramarginal (r = 0.351, p = 0.036), inferior parietal (r = 0.359, p = 0.032), and right cuneus gyrus (r = 0.505, p = 0.002) volumes showed positive correlations with the negative scores of the PANSS (PANSS-N) in schizophrenia patients (Monte Carlo correction, CFT < 0.001, CWP < 0.05) (Table 4, Fig. 4).

The correlation between whole brain volume clusters and the PANSS-N. a Surface maps showed the clusters of the left supramarginal and inferior parietal gyrus; scatter plots showed the positive correlation between these regions and the PANSS-N. b Surface map showed the cluster of the right cuneus; a scatter plot showed the positive correlation between this region and the PANSS-N. PANSS-N, negative scores of positive and negative symptoms scale
Discussion
Schizophrenia is a severe and complex mental disorder primarily originating from neurodevelopmental disturbances [13]. Patients with violent behavior associated with mental disorders present severe clinical symptoms, posing significant challenges to the normal lives and work of both the patients and their families [14]. In recent years, numerous neuroimaging studies, particularly those focusing on brain structural imaging, have confirmed alterations in brain structures of individuals with schizophrenia. The anatomical brain regions affected by these alterations mainly include the prefrontal cortex, insular cortex, and temporal cortex [6]. Structural magnetic resonance imaging (sMRI) primarily utilizes T1WI sequences, typically employing 3D imaging techniques. It features high resolution, noninvasive examination, and enables quantitative measurement and precise localization of brain regions affected by the disorder.
We utilized 3D high-resolution sMRI combined with Freesurfer to examine the whole-brain cortical thickness and volume in patients with schizophrenia, distinguishing between those exhibiting violent behavior and those without. Our aims were to explore the characteristic changes in cortical thickness and volume in schizophrenia patients with violent behavior and investigate the correlation between alterations in cortical thickness, cortical volume, and clinical symptoms.
In our study, we identified statistical differences in cortical thickness and volume between schizophrenia patients with or without a risk of violence. The ROC curve analysis revealed compelling evidence that the cortical thickness of the left caudal middle frontal gyrus and volume of the right middle temporal gyrus could serve as effective biomarkers for diagnosing the risk of violence in schizophrenia patients. Furthermore, we discovered that cortical volume in the left supramarginal gyrus, inferior parietal gyrus, and right cuneus gyrus exhibited positive associations with PANSS-N scores. These findings underscore the importance of cortical thickness and volume measurements in understanding the risk of violence and associated neuropsychiatric symptoms in schizophrenia patients.
Cortical thickness refers to the distance between the inner and outer surfaces of the cerebral cortex (gray matter), typically measured in millimeters (mm) [15]. The thickness of the cerebral cortex varies across different brain regions, ranging from 1.0 to 4.5 mm, with an average thickness of approximately 2.5 mm [5]. Several factors, including the size, density, and arrangement of neurons, can influence cortical thickness [16]. Additionally, alterations in cortical thickness may result from changes in neuronal dendrites, dendritic spines, and myelin sheaths within specific brain regions [17]. Consequently, changes in cortical thickness serve as quantitative indicators of abnormalities in neuronal cell structure and brain development.
Recent studies have highlighted the significance of cortical thickness changes in the research of psychiatric disorders. Chronic schizophrenia, in particular, has been associated with widespread cortical thinning, affecting key regions such as the prefrontal and temporal cortices, cingulate cortices, and occipital regions [18, 19]. These alterations in cortical thickness are intricately linked to cognitive functioning and may arise from abnormal neuronal activity in the frontal and temporal cortical areas, leading to consequential changes in functional connectivity [20, 21]. The observed involvement of the prefrontal cortex (PFC), including the caudal middle frontal gyrus, aligns with previous research highlighting the PFC's crucial role in regulating aggression and impulse control [22]. Notably, these alterations predominantly occur in the left hemisphere, consistent with lateralization patterns often associated with emotional processing and aggression [23]. Studies investigating impulsivity in individuals with thinner PFC [24] and risk-taking behaviors associated with more significant PFC underscore the importance of cortical thickness in understanding cognitive and behavioral traits. Luckhaus et al. detected increased activity in the medial frontal and cingulate gyri, as well as temporal-occipital regions, in patients with schizophrenia exhibiting violent tendencies [25]. Consistently, our study identified a reduction in cortical thickness in the left caudal middle frontal gyrus among schizophrenia patients at risk of violence. This finding aligns with prior literature and suggests that the reduction in cortical thickness in this region may contribute to heightened activity, potentially contributing to the risk of violence among individuals with schizophrenia.
Patients diagnosed with schizophrenia consistently exhibit global reductions in gray matter volume [26, 27]. Another remarkable discovery in our study was the reduction in cortical volume within the right middle temporal gyrus among individuals diagnosed with schizophrenia and a history of violent behaviors. The right middle temporal gyrus, traditionally associated with language processing and emotion regulation, has emerged as a focal point for structural alterations in schizophrenia patients. Interestingly, prior research has consistently emphasized the role of the temporal lobe in the modulation of aggressive behaviors [28]. Furthermore, the lateralization of these structural changes, specifically to the right hemisphere, adds a unique layer to our understanding of the neural underpinnings of violence risk in schizophrenia. The schizophrenia neurodevelopmental hypothesis posits that structural abnormalities in the brain may manifest as part of a dysconnectivity syndrome within fronto-temporo-limbic circuits [29]. Previous neuroimaging investigations have consistently implicated dysfunctional brain areas located in the medial temporal regions in individuals with histories of aggression and violence [30]. Our finding aligns with prior literature and suggests that the reduction in cortical volume within the right middle temporal gyrus associated with violent behavior may be attributed to reduced activation in the medial temporal regions during response inhibition.
Beyond the inter-group analyses, our study also uncovered positive correlations between the volumes of distinct brain regions—the left supramarginal gyrus, inferior parietal gyrus, and right cuneus gyrus—and scores on the PANSS-N among individuals diagnosed with schizophrenia. The regions exhibiting positive correlations with PANSS-N scores play crucial roles in sensory integration, attention, and visual processing [31,32,33]. These functions highlight the intricate interplay between brain structure and the symptomatic presentation of schizophrenia. The observed associations emphasize the complex nature of this mental disorder and underscore the importance of exploring how alterations in brain structure may contribute to the symptomatology experienced by patients. Our findings resonate with previous research, such as Faerden's study, which emphasized the strong association between negative symptoms and impaired functioning, even from the first episode of psychosis [34]. Additionally, Menahem et al. underscored the intricate connection between depression, impulsivity, and violence, possibly reflecting serotonergic dysfunction in certain violent patients with schizophrenia [35]. These insights underscore the importance of gaining a deeper understanding of schizophrenia with a risk of violence, shedding light on how negative symptoms may significantly influence clinical outcomes.
Limitations
The main limitations of our study are the small sample size of 36 schizophrenia patients, including 19 with a history of violence, and the cross-sectional design, which limits the generalizability of our findings and prevents establishing causal relationships. Longitudinal studies are needed to examine changes in brain structure over time. Additionally, our focus on PANSS-N scores means we did not consider other symptom domains, which could offer a more comprehensive understanding of schizophrenia.
Conclusions
In conclusion, our study reveals critical structural brain differences in schizophrenia patients with a history of violence, specifically reduced cortical thickness in the left caudal middle frontal gyrus and decreased cortical volume in the right middle temporal gyrus. These findings, with promising diagnostic efficiency, highlight potential biomarkers for early detection of violence risk. These biomarkers can improve clinical outcomes by enabling targeted interventions.
Availability of data and materials
The datasets analyzed during the current study are not publicly available due restrictions as they contain information that could compromise the privacy of research participants but are available from the corresponding author on reasonable request.
Abbreviations
- MOAS:
-
Modified overt aggression scale
- ICD-10:
-
International classification of diseases tenth revision
- PANSS:
-
Positive and negative syndrome scale
- PANSS-N:
-
Negative scores of positive and negative syndrome scale
- TR:
-
Repetition time
- TI:
-
Inversion time
- TE:
-
Echo time
- FA:
-
Flip angle
- FOV:
-
Field of view
- GLM:
-
General linear model
- ICV:
-
Intracranial Volume
- CFT:
-
Cluster-forming threshold
- CWP:
-
Cluster-wise probability
- ROI:
-
Region of interest
- MNI:
-
Montreal neurological institute
- GM:
-
Gray matter
- PFC:
-
Prefrontal cortex
- ACC:
-
Anterior cingulate cortex
References
Mothersill O, Knee-Zaska C, Donohoe G (2016) Emotion and theory of mind in schizophrenia-investigating the role of the cerebellum. Cerebellum 15(3):357–368
Sopromadze S, Tsiskaridze A (2018) Violent behavior. Front Neurol Neurosci 42:106–121
Witt K, van Dorn R, Fazel S (2013) Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS ONE 8(2):e55942
Dack C, Ross J, Papadopoulos C, Stewart D, Bowers L (2013) A review and meta-analysis of the patient factors associated with psychiatric in-patient aggression. Acta Psychiatr Scand 127(4):255–268
Seiger R, Ganger S, Kranz GS, Hahn A, Lanzenberger R (2018) Cortical thickness estimations of FreeSurfer and the CAT12 toolbox in patients with Alzheimer’s disease and healthy controls. J Neuroimaging 28(5):515–523
Fani N, Eghbalzad L, Harnett NG, Carter SE, Price M, Stevens JS, Ressler KJ, van Rooij SJH, Bradley B (2022) Racial discrimination associates with lower cingulate cortex thickness in trauma-exposed black women. Neuropsychopharmacology 47(13):2230–2237
Bateni H, Soltani E, Ali K, Zhou H, Shad MU (2023) Effect of transcranial magnetic stimulation on postural control of individuals with major depressive disorder: a case report. SAGE Open Med Case Rep 11:2050313X231153757
Pennington DL, Durazzo TC, Schmidt TP, Abe C, Mon A, Meyerhoff DJ (2015) Alcohol use disorder with and without stimulant use: brain morphometry and its associations with cigarette smoking, cognition, and inhibitory control. PLoS ONE 10(3):e0122505
Kumari V, Barkataki I, Goswami S, Flora S, Das M, Taylor P (2009) Dysfunctional, but not functional, impulsivity is associated with a history of seriously violent behaviour and reduced orbitofrontal and hippocampal volumes in schizophrenia. Psychiatry Res 173(1):39–44
Meyer LF, Telles LEB, Mecler K, Soares A, Alves RS, Valenca AM (2018) Schizophrenia and violence: study in a general psychiatric hospital with HCR-20 and MOAS. Trends Psychiatry Psychother 40(4):310–317
Sederevicius D, Vidal-Pineiro D, Sorensen O, van Leemput K, Iglesias JE, Dalca AV, Greve DN, Fischl B, Bjornerud A, Walhovd KB, Fjell AM (2021) Alzheimers disease neuroimaging initiative: reliability and sensitivity of two whole-brain segmentation approaches included in FreeSurfer-ASEG and SAMSEG. Neuroimage 237:118113
Alexander B, Loh WY, Matthews LG, Murray AL, Adamson C, Beare R, Chen J, Kelly CE, Anderson PJ, Doyle LW, Spittle AJ, Cheong JLY, Seal ML, Thompson DK (2019) Desikan-Killiany-Tourville atlas compatible version of M-CRIB neonatal parcellated whole brain atlas: the M-CRIB 2.0. Front Neurosci 13:34
Winship IR, Dursun SM, Baker GB, Balista PA, Kandratavicius L, Maia-de-Oliveira JP, Hallak J, Howland JG (2019) An overview of animal models related to schizophrenia. Can J Psychiatry 64(1):5–17
Cavalera C, Ferrari C, Bianconi G, Bulgari V, Candini V, Carra G, Clerici M, Conte G, Cricelli M, Ferla MT, Iozzino L, Macis A, Stefana A, Ornaghi A, de Girolamo G (2020) VIORMED-2 group: substance use disorders and violent behaviour in patients with severe mental disorders: a prospective, multicentre study. Aust N Z J Psychiatry 54(12):1212–1223
Gupta CN, Calhoun VD, Rachakonda S, Chen J, Patel V, Liu J, Segall J, Franke B, Zwiers MP, Arias-Vasquez A, Buitelaar J, Fisher SE, Fernandez G, van Erp TG, Potkin S, Ford J, Mathalon D, McEwen S, Lee HJ, Mueller BA, Greve DN, Andreassen O, Agartz I, Gollub RL, Sponheim SR, Ehrlich S, Wang L, Pearlson G, Glahn DC, Sprooten E, Mayer AR, Stephen J, Jung RE, Canive J, Bustillo J, Turner JA (2015) Patterns of gray matter abnormalities in schizophrenia based on an international mega-analysis. Schizophr Bull 41(5):1133–1142
Bogolepova IN, Malofeeva LI, Agapov PA (2021) The brain of an outstanding scientist-inventor: structural organization of area 10 of the frontal cortex. Bull Exp Biol Med 172(1):1–4
Defenderfer MK, Demirayak P, Fleming LL, DeCarlo DK, Stewart P, Visscher KM (2023) Cortical plasticity in central vision loss: cortical thickness and neurite structure. Hum Brain Mapp 44(10):4120–4135
Ren H, Li Z, Li J, Zhou J, He Y, Li C, Wang Q, Chen X, Tang J (2024) Correlation between cortical thickness abnormalities of the olfactory sulcus and olfactory identification disorder and persistent auditory verbal hallucinations in Chinese patients with chronic schizophrenia. Schizophr Bull 5:sbae040
Sun S, Xiao S, Guo Z, Gong J, Tang G, Huang L, Wang Y (2023) Meta-analysis of cortical thickness reduction in adult schizophrenia. J Psychiatry Neurosci 48(6):E461–E470
Chad-Friedman E, Botdorf M, Riggins T, Dougherty LR (2021) Early childhood cumulative risk is associated with decreased global brain measures, cortical thickness, and cognitive functioning in school-age children. Dev Psychobiol 63(2):192–205
Alkan E, Davies G, Evans SL (2021) Cognitive impairment in schizophrenia: relationships with cortical thickness in fronto-temporal regions, and dissociability from symptom severity. NPJ Schizophr 7(1):20
Bounoua N, Spielberg JM, Sadeh N (2022) Clarifying the synergistic effects of emotion dysregulation and inhibitory control on physical aggression. Hum Brain Mapp 43(17):5358–5369
Hoptman MJ (2015) Impulsivity and aggression in schizophrenia: a neural circuitry perspective with implications for treatment. CNS Spectr 20(3):280–286
Tanzer M, Derome M, Morosan L, Salaminios G, Debbane M (2021) Cortical thickness of the insula and prefrontal cortex relates to externalizing behavior: cross-sectional and prospective findings. Dev Psychopathol 33(4):1437–1447
Luckhaus C, Frommann N, Stroth S, Brinkmeyer J, Wolwer W (2013) Training of affect recognition in schizophrenia patients with violent offences: behavioral treatment effects and electrophysiological correlates. Soc Neurosci 8(5):505–514
Wei Q, Li M, Kang Z, Li L, Diao F, Zhang R, Wang J, Zheng L, Wen X, Zhang J, Zhao J, Huang R (2015) ZNF804A rs1344706 is associated with cortical thickness, surface area, and cortical volume of the unmedicated first episode schizophrenia and healthy controls. Am J Med Genet B Neuropsychiatr Genet 168B(4):265–273
Kim S, Jang SK, Kim DW, Shim M, Kim YW, Im CH, Lee SH (2019) Cortical volume and 40-Hz auditory-steady-state responses in patients with schizophrenia and healthy controls. Neuroimage Clin 22:101732
Shen D (2015) HU J, Qiu C: Brain structural imaging study in schizophrenia patients with violent aggressive behaviors. Chinese J Behav Med Brain Sci 12:875–860
MacKay MB, Paylor JW, Wong JTF, Winship IR, Baker GB, Dursun SM (2018) Multidimensional connectomics and treatment-resistant schizophrenia: linking phenotypic circuits to targeted therapeutics. Front Psychiatry 9:537
Widmayer S, Borgwardt S, Lang UE, Stieglitz RD, Huber CG (2018) Functional neuroimaging correlates of aggression in psychosis: a systematic review with recommendations for future research. Front Psychiatry 9:777
Bourgou Gaha S, Halayem Dhouib S, Amado I, Bouden A (2015) Neurological soft signs in early onset schizophrenia. Encephale 41(3):209–214
Zhang F, Li Y, Liu L, Liu Y, Wang P, Biswal BB (2024) Corticostriatal causality analysis in children and adolescents with attention-deficit/hyperactivity disorder. Psychiatry Clin Neurosci 78(5):291–299
Stillova K, Jurak P, Chladek J, Halamek J, Telecka S, Rektor I (2013) The posterior medial cortex is involved in visual but not in verbal memory encoding processing: an intracerebral recording study. J Neural Trans (Vienna) 120(3):391–397
Faerden A, Barrett EA, Nesvag R, Friis S, Finset A, Marder SR, Ventura J, Andreassen OA, Agartz I, Melle I (2013) Apathy, poor verbal memory and male gender predict lower psychosocial functioning one year after the first treatment of psychosis. Psychiatry Res 210(1):55–61
Krakowski MI, Czobor P (2014) Depression and impulsivity as pathways to violence: implications for antiaggressive treatment. Schizophr Bull 40(4):886–894
Acknowledgments
Not applicable.
Funding
No fund.
Author information
Authors and Affiliations
Contributions
YNL contributed to conceptualization, investigation, data curation, formal analysis, writing—original draft, writing—review and editing. WZL contributed to investigation, data curation, writing—review and editing. LYZ contributed to writing—review and editing, resources.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Written informed consent was waived by the Institutional Review Board of Beijing Huilongguan Hospital. And Institutional Review Board approval (No. 2017-72) was obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, Y., Liang, W. & Zhao, L. Quantitative gray matter volumetric analysis in schizophrenia: investigating the risk of violent behaviors through structural MRI. Egypt J Radiol Nucl Med 55, 119 (2024). https://doi.org/10.1186/s43055-024-01289-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01289-w