
Abstract
Background
Amyand’s hernia is characterized as an inguinal hernia in which the hernia sac contains the appendix. It is highly atypical for the appendix structure to be contained within the hernia sac. Patients with Amyand’s hernia are typically asymptomatic and are frequently identified intraoperatively. Rarely seen in medical literature, this case report details the incidental finding of Amyand’s hernia and the successful preoperative diagnosis.
Case presentation
A 61-year-old male presented to the urology clinic for his urinary tract complaint. An incidental finding of Amyand’s hernia was found in a non-contrast computerized tomography of the abdomen. Following the evaluation of computed tomography scan images showing the condition of the appendix and radiological findings regarding Amyand’s hernia, the surgeon planned the patient’s herniorrhaphy with mesh.
Conclusions
Amyand’s hernia is often overlooked; therefore, radiologic examination can help to confirm this diagnosis.
Similar content being viewed by others


Background
Amyand’s hernia is characterized as an inguinal hernia in which the hernia sac contains the appendix. As reported in numerous publications, the occurrence of the appendix structure within the hernia sac is exceedingly uncommon, ranging from 0.19 to 1.7% [1]. Amyand’s hernia patients are typically asymptomatic and are frequently identified intraoperatively [2]. Preoperative diagnosis and confirmation of Amyand’s hernia can be facilitated through the utilization of radiologic modalities. In this study, we report an infrequently documented case of Amyand's hernia that was incidentally discovered during a non-contrast CT of the abdomen performed as a follow-up for another medical condition. The successful preoperative diagnosis of the hernia is also detailed.
Case presentation
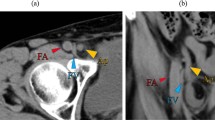
A 61-year-old male presented to the urology clinic with chief complaint of frequent urination which was felt disturbing at night. The patient said this complaint began to bother him in the last 1 month. The patient said that urination often felt interrupted and incomplete. The patient denied any blood or sandy urine. The patient said there was a history of surgery with ureteroscopy (URS) and lithotripsy for indication of sinistra distal urinary tract stone in 2018. On physical examination, costovertebral angle tenderness was not found. From the urology clinic, the patient was planned for a non-contrast CT of the abdomen examination. On a non-contrast CT of the abdomen examination, a herniated appendix and peritoneal fat structure were found in the right inguinal canal, with an appendix diameter of ± 0.58 cm (Figs. 1 and 2). In addition, an enlarged prostate (volume ± 55 cc) was found accompanied by calcification, and no stones were seen in the ureter.

CT scan, a axial reformat, b sagittal reformat, an extension of the appendix (white arrow) into the right inguinal hernia (white circle)

CT scan, coronal-oblique reformat, structure appendix (white arrow) originates proximally from the caecum and extends distally into the right inguinal hernia (white circle)
Afterward, the surgeon scheduled the patient for herniorrhaphy with mesh, and the patient was discharged from the hospital on the third day after the surgery.
Discussion
Amyand’s hernia is characterized as an inguinal hernia in which the hernia sac contains the appendix [1]. The initial identification of this condition was made by C. Amyand in 1735, following the observation of an 11-year-old male patient with an incarcerated inguinal hernia that contained a perforated appendix [1]. Variations in the literature indicate that Amyand’s hernia occurs between 0.19 and 1.7% of hernia cases which have been reported [3]. According to a study by D’Alia et al. [4], Amyand’s hernia mostly occurs on the right side and only affects males.
Although the exact pathophysiologic mechanism underlying Amyand’s hernia remains unclear, numerous hypotheses have been proposed. One explanation by Michalinos et al. suggests that congenital herniation of the appendix occurs when there are both a patent vaginal process and a fibrous link between the appendix and testis [5]. An alternative theory indicated a congenital weakness of the right colon. According to this explanation, the herniation cases involved both the caecum and the appendix [5, 6].
Losanoff and Basson categorized Amyand’s hernia into four distinct varieties, along with management recommendations. For cases classified as type 1, it is advisable to do mesh repair or hernia reduction if the appendix is found to be normal. Acute appendicitis occurring within an inguinal hernia sac characterizes type 2–4, which are treated with appendectomy and primary repair (without mesh). In type 3, abdominal irrigation laparotomy is performed in conjunction with the primary repair and appendectomy; conversely, in type 4, abdominal pathology whether related or unrelated is investigated as required [7, 8].
Supporting Losanoff and Basson classification, Constantine et al. utilized abdominal CT to classify four subtypes of Amyand’s hernia in 2019. Type 1 may go undiagnosed due to the normal appearance of the appendix. A type 2 Amyand’s hernia is distinguished by the presence of inflammation in the surrounding adipose tissue and a distended and inflamed appendix. Diagnosis of type 3 is difficult due to the presence of severe inflammatory alterations, which may obstruct the appendix and even spread intra-abdominally. Type 4 is ultimately associated with additional intra-abdominal findings [8, 9].
To better understand the various kinds of hernias, radiology as a diagnostic tool might be helpful. For example, in diagnostic imaging, direct inguinal hernias manifest medially to the inferior epigastric vessels, whereas indirect hernias occur laterally to the inferior epigastric vessels [10]. On occasion, a CT scan may detect an obturator hernia, which manifests as a bowel herniating through the obturator foramen and is positioned between the pectineus muscle and the obturator externus muscle [11]. Additionally, a femoral hernia presents itself in the medial aspect of the femoral canal, which sometimes manifests as a hernia sac with femoral vein compression.
Due to the similarity in clinical symptoms between inguinal hernia and Amyand’s hernia, the diagnosis of Amyand’s hernia is commonly established after surgery, but the use of radiological modalities such as ultrasound (US) and abdominal computerized tomography scan can confirm the suspicion of Amyand’s hernia [12]. Although ultrasound is the least invasive modality, its effectiveness is exceptionally reliant on the skill of the examiner. When detecting complex hernias or other etiologies of groin masses, computerized tomography scanning can aid in the better delineation of the anatomy of the groin [13].
Ultrasound imaging reveals an elongated, blind-ended tubular cord with a thick adventitial lining that communicates with the caecum while enclosed within the hernia sac. In contrast, the abdominal CT scan reveals the presence of a tubular cord that is blind-ended, originating proximally from the caecum, and invaginating distally into an inguinal hernia sac [12]. The administration of contrast material is critical, and sagittal and coronal reformats on CT scans are extremely useful for diagnosis [8].
In our patient, Amyand’s hernia was found incidentally (Figs. 1 and 2) with a non-contrast CT of the abdomen examination performed to confirm other diagnoses. Surgery has been performed, and intraoperatively no appendiceal structure was found in the hernia sac. We suspect this case is a reduceable hernia so that intraoperatively, the appendix does not appear in the hernia sac but in the intra-abdominal. The hernia’s type and the sac’s size determine whether this is possible [14]. Furthermore, this case was found in a patient of male gender and the hernia was found on the right side, which aligns with the study by D’Alia et al. and Gurer et al. [4, 15]. Based on the Losanoff and Basson classification, this Amyand’s hernia case can be classified in type 1 so that according to the actions taken the patient was performed herniorrhaphy with mesh.
Conclusion
Amyand’s hernia is an inguinal hernia that is exceedingly rare. Preoperative identification of Amyand’s hernia is challenging due to the similarity between its clinical manifestations and those of inguinal hernia. The diagnosis is thus frequently conducted during the surgical procedure. By detecting appendical structures inside the hernia sac, radiology may aid in the diagnosis of Amyand’s hernia. Two radiologic modalities—ultrasound and CT—are capable of verifying whether the appendix is present within the hernia sac. However, the use of US still depends on the examiner’s skill, so a CT scan can be an option to provide a more detailed picture of Amyand's hernia, especially for identifying additional causes of a groin mass or in cases of complicated hernias. The management approach for Amyand’s hernia may be modified in accordance with the radiologic findings and the CT scan images revealing the condition of the appendix.
Availability of data and materials
Not applicable.
Abbreviations
- CT:
-
Computerized tomography
- URS:
-
Ureteroscopy
- US:
-
Ultrasound
References
Patoulias D, Kalogirou M, Patoulias I (2017) Amyand’s hernia: an up-to-date review of the literature. Acta Med (Hradec Kralove) 60:131–134
Khalid H, Khan NA, Aziz MA (2021) Amyand’s hernia a case report. Int J Surg Case Rep 86:106332
Morales-Cárdenas A, Ploneda-Valencia CF, Sainz-Escárrega VH et al (2015) Amyand hernia: case report and review of the literature. Ann Med Surg (Lond) 4:113–115
Dalia C, Schiavo L, Tonante MG et al (2003) Amyand’s hernia: case report and review of the literature. Hernia 7:89–91
Michalinos A, Moris D, Vernadakis S (2014) Amyand’s hernia: a review. Am J Surg 207:989–995
Ranganathan G, Kouchupapy R, Dias S (2011) An approach to the management of Amyand’s hernia and presentation of an interesting case report. Hernia 15:79–82
Losanoff JE, Basson MD (2007) Amyand hernia: what lies beneath–a proposed classification scheme to determine management. Am Surg 73:1288–1290
Fezoulidi G, Argyrouli V, Adamopoulos E, Makridis KG, Zourntou SE, Fezoulidis IV (2021) Amyand’s hernia: presumptive diagnosis by CT and literature review. Radiol Case Rep 16:911–915
Constantine S (2009) Computed tomography appearances of amyand hernia. J Comput Assist Tomogr 33:359–362
Lee GH, Cohen AJ (1993) CT imaging of abdominal hernias. AJR Am J Roentgenol 161:1209–1213
Khaladkar SM, Kamal A, Garg S, Kamal V (2014) Bilateral obturator hernia diagnosed by computed tomography: a case report with review of the literature. Radiol Res Pract 2014:1–4
Shekhani HN, Rohatgi S, Hanna T, Johnson J-O (2016) Amyand’s hernia: a case report. J Radiol Case Rep 10:7–11
Lassandro F (2011) Abdominal hernias: radiological features. World J Gastrointest Endosc 3:110
AhmedAlenazi A, Alsharif MM, Hussain MA et al (2017) Prevalence, risk factors and character of abdominal hernia in Arar City, Northern Saudi Arabia in 2017. Electron Phys 9:4806
Gurer A, Ozdogan M, Ozlem N et al (2006) Uncommon content in groin hernia sac. Hernia 10:152–155
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
The authors confirm contribution to the paper as follows: F. Susilo and M.A. Charlee contributed to study conception and design; F. Susilo and Ronny contributed to data acquisition; Ronny and Y. Simargi performed data analysis and/or interpretation; M.A. Charlee, F. Susilo, and Ronny performed draft manuscript preparation. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Susilo, F., Charlee, M.A., Simargi, Y. et al. Incidental finding of Amyand’s hernia in a non-contrast CT of the abdomen: a case report. Egypt J Radiol Nucl Med 55, 75 (2024). https://doi.org/10.1186/s43055-024-01246-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01246-7