
Abstract
Background
Conventional transarterial chemoembolization (cTACE) has emerged as a major treatment modality for unresectable hepatocellular carcinoma (HCC). Efforts have recently been made to identify biomarkers of HCCs that can potentially predict the response of lesions to transarterial chemoembolization (TACE) therapy. The goal of these efforts is to simplify the decision-making process on whether a patient should choose cTACE or pursue other treatment options. Among these, computed tomography (CT) based lipiodol retention analysis has shown promise in providing valuable insights into post-TACE outcomes. This study aimed to investigate the value of CT-based lipiodol retention pattern in predicting recurrence after a state of complete response (CR) according to modified Response Evaluation Criteria in Solid Tumors (mRECIST) guideline post-cTACE.
Methods
From January 2022 to June 2023, a cohort of 30 patients with 40 HCCs who received a primary cTACE session were identified. The study included patients who underwent 1st cTACE session with no more than three HCCs. Ten HCC lesions were eliminated owing to different reasons (illustrated in the flow chart). Tumor response was evaluated based on mRECIST on 1st follow-up CT with a particular focus on tumors demonstrating a complete response. Patterns of lipiodol retention within these tumors were categorized as complete lipiodol retention pattern (C-Lip), covering the whole tumor, or incomplete lipiodol retention pattern (I-Lip). Recurrence was defined when reappearance of enhancement on arterial-phase images of the treated lesion with subsequent washout on portal/delayed phase images occurred corresponding to findings of restricted diffusion on follow-ups DCE-MRI.
Results
A total of 30 HCCs with a CR were classified into 21 (70%) with C-Lip and 9 (30%) with I-Lip. After a median follow-up of 6.00 ± 2.27 months (3–9 months), 8/9 (88.9%) I-Lip and 5/21 (23.8%) C-Lip showed recurrence on follow-up (DCE-MRI), (p < 0.01), with no significant difference in the time of progression (mean 5.57 ± 2.69 for C-Lip vs. 6.00 ± 2.27 months for I-Lip, with (p < 0.5).
Conclusions
HCCs exhibit complete lipiodol retention alongside mRECIST CR possess a reduced susceptibility of recurrence, thereby potentially benefiting from MRI during subsequent evaluations. Conversely, the presence of incomplete lipiodol retention in conjunction with mRECIST CR is an indication of a high risk of recurrence and may require further treatment.
Similar content being viewed by others


Background
Hepatocellular carcinoma (HCC) is a primary liver cancer in adults that ranks as the fifth most frequent cancer and the second highest contributor to cancer-related morbidity and mortality globally [1]. Conventional transarterial chemoembolization (cTACE) has emerged as a crucial therapeutic option for HCC, especially for those patients who fall under the intermediate stage Barcelona clinic liver cancer (BCLC) B stage (HCC) category, with level 1A proof [2, 3]. One of the classification systems widely used for the assessment of treatment response post-cTACE is modified Response Evaluation Criteria in Solid Tumors (mRECIST), according to which, the absence of a hypervascular component following cTACE in contrast-enhanced computed tomography (CECT) or dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) signifies necrosis of the tumor [4]. A state of complete response (CR) is attained when all hypervascular components are no longer present [5].
Although achieving CR after the first cTACE has been introduced as the most robust predictor for favorable outcomes in HCC [6], recurrence after CR presents and rates have been recorded [7,8,9]. Predicting this recurrence is critical for treatment planning and deciding early whether a patient should receive primary or repeated TACE or alternative forms of treatment to eliminate recurrence patterns [10], thus efforts have been recently made to identify biomarkers that may predict lesion response following cTACE treatment [11], one of which, is lipiodol.
The rationale behind investigating lipiodol retention stems from its established role as a crucial imaging marker for necrosis post-CTACE [12, 13]. It is widely acknowledged that the degree of lipiodol retention could be indicative of treatment efficacy [14]. However, its precise predictive value for recurrence post-complete response has not been comprehensively evaluated.
We hypothesized that post-cTACE HCCs exhibiting a CR with a complete lipiodol retention pattern (C-Lip) may differ in progression from CR with incomplete lipiodol retention (I-Lip).
This study aimed to fill the gap in knowledge about the predictive role of lipiodol retention patterns and contribute to a more refined approach in managing HCC patients who have achieved a complete response following cTACE.
Methods
Study design
From January 2022 to June 2023, a prospective study was conducted on patients advised to have cTACE by a multidisciplinary tumor board with written informed consent and institutional review board permission. It was a multicentric study, conducted at the National Hepatology and Tropical Medicine Research Institute and Benha University.
Participants' inclusion criteria were: (1) the presence of at least one and not more than three HCC lesions defined according to liver imaging reporting and data systems (LI-RADS), (2) participants undergoing the cTACE procedure according to BCLC for the first time, and (3) the presence of triphasic abdominal CT or DCE-MRI before cTACE procedure. The study excluded participants whose HCCs were not classified as LR-5, i.e., lesions exhibited hypoenhancement during the arterial phase and/or possessed infiltrative characteristics.
The study was conducted on 30 patients who fulfilled the criteria (19 male and 11 female [63.3% vs. 36.7%] respectively; mean age 66.1 ± 6.2 years old) with 40 HCC lesions (mean 28.4 ± 11.73 mm [13–60 mm]).
On 1st follow-up CT, according to mRECIST, 3 lesions were eliminated (in 2 patients, one with double lesions and the other with a solitary lesion) for not showing CR. On 1st month DCE-MRI following 1st follow-up CT, 2 lesions were eliminated in 1 patient with triple lesions for progression of the disease in one of them, the patient underwent a 2nd cTACE session. On 3rd month DCE-MRI, 2 lesions were eliminated (in 2 patients, one with double lesions for progression of the disease in one of them and the other with a solitary lesion for death). On 6th month DCE-MRI, 3 lesions were eliminated (in 3 patients, two patients each had double lesions for the progression of the disease in one of them, and one patient with a solitary lesion for missing the follow-up). As 10 HCCs were eliminated during the study period, the study was conducted on a total of 30 HCCs. The Study design was presented in a flowchart (Fig. 1).

Study design. cTACE: conventional transarterial chemoembolization, C-Lip: complete lipiodol retention, CR: complete response, CT: computed tomography, DCE-MRI: dynamic contrast-enhanced magnetic resonance imaging, HCC: hepatocellular carcinoma, I-Lip: incomplete lipiodol retention, mRECIST: modified response evaluation criteria in solid tumors, N: number, PD: progressive disease
cTACE procedure
All cTACE procedures were executed in adherence to our established institutional protocol. Under local anesthesia, using a 5F introducer sheath and the Seldinger method, a femoral approach was achieved. Each target lesion and its vascular feeders were identified using digital subtraction angiography. A 5F Cobra or Simmons angiographic catheter was used to catheterize the celiac trunk or superior mesenteric artery. The procedure was performed with either selective or superselective with an infusion of a combination of chemotherapy (with a maximum dosage of 50 mg of doxorubicin, commercially known as Adriamycin; manufactured by Pharmacia Upjohn), 10 mg of emulsified iodized oil (marketed as Lipiodol and produced by Gerbet), and 10 mg of saline (consisting of sodium chloride 0.9%). In superselective procedures, an additional embolization was carried out by injection of Gelitaspon, a gelatin sponge manufactured by Gelita Medical B.V.
CT protocol
All pre- and post-cTACE contrast-enhanced abdominal computed tomography scans were conducted using MDCT (160 slices Canon, Aquilion Prime CT machine). Following a non-enhanced abdominal scan, a nonionic iodinated contrast agent with a concentration of 350 mg/mL was infused intravenously through a 16–18 gauge cannula to conduct a multiphase acquisition. Antecubital vein injection of contrast agent averaged 2 mL/kg at a rate of 4 mL/sec. Following the infusion, acquisitions of the arterial, portal-venous, and delayed phases were obtained at 35, 80, and 180 s, respectively. For each acquisition, a maximum thickness of 3mm per slice was obtained.
MRI protocol
A 1.5 Tesla (Philips, Ingenia MRI machine) was utilized in adherence to our institute standard protocol including (1) T2-weighted spin echo sequence, (2) In-phase and out-of-phase gradient echo sequences (3) non-enhanced and contrast-enhanced T1-weighted gradient echo sequences after injection of gadolinium-based contrast agent, 0.1 mmol per kg of body weight, hepatic arterial phase (20 s), portal venous phase (70 s) and delayed phase (3 min) post-contrast injection, and (4) diffusion-weighted sequence with apparent diffusion coefficient images.
Image analysis
Pre-cTACE image analysis
Triphasic abdominal CT images or DCE-MRI images, obtained within 1-month prior to cTACE procedure, were assessed by two senior radiologists with experience of 13 and 20 years in the field of medical imaging who assessed the cases collaboratively. The images were subjected to a process of consensus review on (PaxeraUltima Health) picture archiving and communication system (PACS). Every lesion was inspected for various fundamental characteristics, which include: (a) location categorized as left/right lobes, (b) the largest diameter (measured in millimeters), (c) the presence of a capsule, and (d) the presence of portal vein thrombosis.
Post-cTACE image analysis
First follow-up CT
Within 4–6 weeks post-cTACE, 1st follow-up CT was performed. Contrast-enhanced images were assessed for tumor response in a tumor-by-tumor analysis and classified according to mRECIST [15] into complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). Examiners assigned lesions with CR by the disappearance of arterial enhancement in all target lesions, while eliminating HCCs with responses other than CR. Non-enhanced images were also assessed to evaluate the lipiodol retention pattern. Images were compared with pre-cTACE contrast-enhanced CT images to explore the whole tumor volume. The extent of hyperattenuation observed in the nodular area due to lipiodol deposition was used to classify lipiodol retention as C-Lip or I-Lip, where C-Lip denoted entire hyperattenuating lesion while I-Lip denoted partial hyperattenuating lesion.
Successive follow-ups by DCE-MRI
Dynamic contrast-enhanced magnetic resonance imaging was used as a gold standard for the assessment of HCCs with CR in follow-up sessions. Each tumor was followed by the application of mRECIST criteria on DCI-MRI 1,3,6, and 9 month(s) following 1st CT post-cTACE. Progression of disease (PD) was defined by the emergence of enhancement in arterial phase images with washing out on portal-venous or delayed phase images accompanied by restricted diffusion within a lesion previously diagnosed as CR.The interval between the cTACE session and the occurrence of recurrence was documented and every patient was re-assessed for further repeated cTACE sessions or other therapeutic procedures. If a participant had multiple lesions with different responses, i.e., one or more lesion(s) showed PD while the other lesion(s) showed CR, lesions with PD were included in the study, while lesions with CR were eliminated as the participant would undergo a 2nd cTACE session. If a follow-up DCE-MRI revealed no local tumor recurrence for at least 9 months post-cTACE, the response was titled as a persistent CR.
Final non-enhanced CT
At the end of the study period time for each tumor, final non-enhanced CT images were obtained and analyzed for lipiodol retention pattern in comparison with the pattern defined on the 1st non-enhanced follow-up CT images. Examiners commented on retention patterns by either no change, reduced size, or vanished lipiodol retention.
Statistical analysis
Where applicable, data was presented using measures like means, standard deviations, and ranges, or alternatively, the number of patients and frequencies. The comparison of frequencies was performed using a Chi-square test, while the comparison of continuous variables was conducted through the independent t-test. Univariate logistic regression analyses were performed to identify predictors of recurrence. The odds ratio (OR) was employed to weigh the correlation between the pattern of lipiodol retention and recurrence. Tests of sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were used to assess the performance of lipiodol retention patterns in predicting recurrence. The time interval between the cTACE session and the initial occurrence of recurrence was recognized as a time to recurrence. p values more than 0.05 were considered non-significant; p-values less than 0.05 were considered significant; and p-values less than 0.01 were considered highly significant.
Results
Demographic data and lesions baseline characteristics
This study was carried out on 30 patients with 40 HCC lesions. Patients' gender was 19 male and 11 female (63.3% vs. 36.7%) respectively. The age range was between 53 and 75 Years with a mean ± SD of 66.1 ± 6.2. All 30 patients had cirrhosis with a positive history of HCV. Patients had a variable number of HCCs, as 21/30 patients had a solitary HCC lesion, 8/30 patients had 2 lesions, and 1/30 patients had 3 lesions representing (70.0%, 26.7%, and 3.3%) respectively. HCCs had a mean of 28.4 ± 11.73 mm in diameter, a range of (13–60mm). Alpha-fetoprotein (AFP) of the studied cases was between 440 and 960 ng/ml with a mean ± SD of 722 ± 158 ng/ml. Patients' serum albumin was between 20 and 58 g/L with a mean ± SD of 39.16 ± 12 g/L, while serum bilirubin ranged between 34 and 62 µmol/L with a mean ± SD of 47.7 ± 8.8 µmol/L (Table 1).
cTACE characteristics
The procedure of cTACE was conducted as a selective procedure without injecting an embolic agent in 13/30 (43.3%) patients, and a superselective procedure with an injection of Gelfoam in 17/30 (56.7%) patients. The dose of Adriamycin mixture with lipiodol was unified to 70 mg and delivered to (100.0%) patients of the study.
Lipiodol retention pattern and cTACE response
Out of the total 30 HCCs showed CR on the 1st follow-up CT, lipiodol retention was identified as C-Lip in 21 of them, which accounts for 70%, while the remaining 9 tumors, which make up 30%, were considered to have I-Lip. Alpha-fetoprotein levels in the two groups showed a mean ± SD of 709 ± 148 ng/ml in the C-Lip group and 753 ± 185 ng/ml in the I-Lip group with a p-value of 0.501. The average dimensions of tumors that displayed C-Lip and I-Lip were at a mean ± SD of 23.9 ± 9.56 mm and 38.89 ± 9.66 mm, respectively, with a significance level of p = 0.001. Out of 21 C-lip lesions, 14/21 (66.7%) were located at the right lobes, while 7/21 (33.3%) were located at the left lobes, compared to I-Lip lesions where 5/9 (55.6%) were located at the right lobes, while 4/9 (44.4%) were located at the left lobes, with a significance of p = 0.563. The capsule appeared in 16/21 (76.2%) C-Lip lesions, while appeared only in 3/9 (33.3%) I-Lip lesions, with p = 0.026. Superselectivity of cTACE procedure was associated with 15/21 (71.4%) C-Lip lesions, and 2/9 (22.2%) I-Lip lesions, with a significance level of p = 0.013 (Table 2).
The outcome of CR follow-up post cTACE by DCE-MRI
During DCE-MRI follow-ups, tumor progression was reported in 13/30 (43.3%) lesions with an initial CR, as in case (1), presented in Fig. 2A–C while the tumors maintained a complete response without any recurrence were 17/30 (56.7%) lesions as in case (2), presented in Figs. 3A–C. Recurrence group vs. no recurrence group showed AFP levels with a mean ± SD of 743 ± 179 ng/ml and 706 ± 144 ng/ml, respectively, with a p-value of 0.534. The dimensions of tumors that displayed recurrance were at a mean ± SD of 34.69 ± 11.19 mm versus 38.89 ± 9.66 mm compared with lesions that displayed no recurrance, with a significance of p = 0.001. Among 13 lesions that exhibited recurrence, 7/13 (53.8%) were located at the right lobes, while 6/13 (46.2%) were positioned at the left lobes. In comparison, lesions with no recurrence were detected in the right lobes in 12 out of 17 lesions (70.6%) and in the left lobes in 5 out of 17 cases (29.4%), with a p-value of 0.346. The presence of a capsule was observed in 5/13 (38.5%) recurrence group, whereas it was present in 14/17 (82.4%) no recurrence group, with p = 0.013. The superselectivity of the cTACE procedure was associated with 4/13 (30.8%) lesions with recurrence, while 13/17 (76.5%) lesions with no recurrence, with a level of significance of p = 0.012 (Table 3).

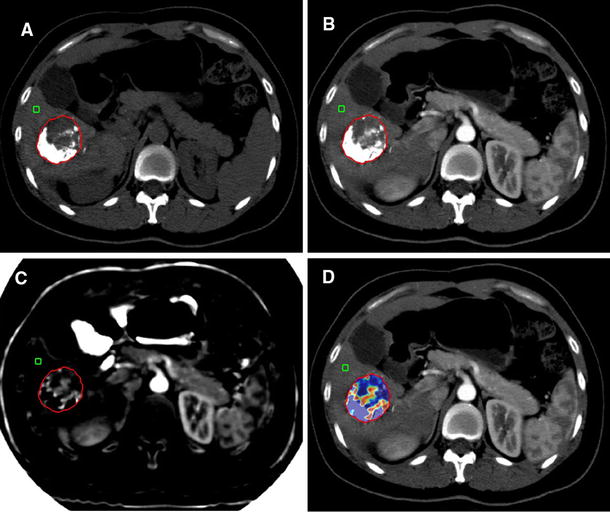
Case (1) (A) CT study, A 60-year-old female patient with cirrhosis and mild ascites had shown an HCC lesion with CR according to mRECIST accompanied by incomplete lipiodol retention. a Pre-TACE baseline post-contrast axial CT image showed heterogenous enhanced HCC lesion at segment VII measuring 2.5 × 2 × 1 cm (white arrow). b, c On initial follow-up CT, the lesion displayed incomplete lipiodol retention (yellow arrow) on a pre-contrast image (b), whereas the hepatic arterial phase image (c) did not exhibit any residual enhancement. Non-enhanced CT image obtained on the 6th month post-cTACE (d) showed a reduced size of retained lipiodol (blue arrow). Case (1) (B) (e–n) On 1st-month follow-up DCE-MRI serial images, the lesion showed in-phase (e) and out-of-phase (f) T1WI hypointensity, no contrast enhancement in all contrast phases (g–k); arterial (h), portal (i), venous (j), and delayed (k) phases. Lesion displayed T2WI (l) hyperintensity and free diffusion in DWI (m) and ADC (n) images, denoting complete response. Case (1) (C) On 6th-month follow-up DCE-MRI serial images, the HCC lesion showed in-phase (o) and out-of-phase (p) T1WI hypointensity, pre-contrast phase (q) hypointensity, while in contrast phases (r–u) it showed faint enhancement in the arterial phase (r), with washout in the portal (s), venous (t), and delayed (u) phases (yellow arrows). Lesion displayed faint high signal intensity in T2WI (v). On DWI (w) and ADC (x) images, it showed restricted diffusion (blue arrows), denoting recurrence. A newly developed high-grade dysplastic nodule (red arrow) has emerged into segment VII, with rounded shape, measured less than 1 cm, showed in-phase (o) and out-of-phase (p) T1WI hyperintensity, pre-contrast phase (q) hyperintensity, while in contrast phases (r–u) it showed faint enhancement in the arterial phase (r), without washout in the portal (s), venous (t), or delayed (u) phases. It displayed hypointensity in T2WI (v) with free diffusion on DWI (w) and ADC (x) images

Case (2) (A) 67-year-old male patient with cirrhosis had shown an HCC lesion with CR according to mRECIST accompanied by complete lipiodol retention. (a–j) Baseline Pre-TACE DCE-MRI serial images showed a focal lesion in segment VI/VII, measuring 2 × 1 × 1 cm, displaying in-phase (a) and out-of-phase (b) T1WI hypointensity, T2WI (c) moderate hyperintensity, arterial enhancement with delayed washout (d–h) (yellow arrows), and restricted diffusion in DWI (i) and ADC (j) images(blue arrows). Case (2) (B) (K–m) On initial follow-up CT, the lesion displayed complete lipiodol retention (yellow arrow) on a pre-contrast image (k), whereas images of the hepatic arterial phase (l) did not exhibit any residual enhancement. Non-enhanced CT image obtained on the 9th-month post-cTACE (m) showed almost no appreciable changes in lipiodol pattern compared to the 1st follow-up CT (blue arrow). Case (2) (C) On 9th-month follow-up DCE-MRI serial images, the lesion showed in-phase (n) and out-of-phase (o) T1WI hypointensity, T2WI (p) hyperintensity, pre-contrast phase image (q) hypointensity, no contrast enhancement in all contrast phases (r–u); arterial (r), portal (s), venous (t), delayed (u) phases. On DWI (v) and ADC (w) images, free diffusion was denoted, assuring persistent complete response
After being observed for a period of 6.0 ± 2.27 months on average, and compared to the results of 1st follow-up CT, 8/9 (88.9%) and 5/21 (23.8%) of tumors with I-Lip and C-Lip, respectively, exhibited recurrence (p < 0.01). There was no significant difference in the time taken for recurrence (p = 0.743) between the two groups (Table 4).
Factors influenced recurrence in CR tumors
Factors of lesion diameter larger than 28 mm, non-capsulation of HCC lesion, and selective cTACE procedures demonstrated a highly significant association with recurrence with p-values of 0.003, 0.019, and 0.016, respectively, and odds ratios of 15.556, 7.467, and 7.312, respectively. Incomplete lipiodol retention exhibited the strongest association with recurrence among the examined variables, with a remarkably low p-value of 0.006 and an exceptionally high OR of 25.600 (Table 5).
Performance of the lipiodol retention pattern as a predictor for recurrence
The sensitivity of the lipiodol retention pattern in identifying cases of incomplete lipiodol retention with recurrence was found to be 61.54% (95% CI 31.58–86.14%). In terms of specificity, the lipiodol retention pattern demonstrated a high value of 94.12% (95% CI 71.31–99.85%). The positive predictive value (PPV) of the lipiodol retention pattern was calculated to be 88.89% (95% CI 53.25–98.25%), while the negative predictive value (NPV) was determined to be 76.19% (95% CI 61.43–86.54%).
Overall, the accuracy of the lipiodol retention pattern in predicting recurrence was found to be 80.00% (95% CI 61.43–92.29%).
Discussion
The prediction of the treatment response of HCC following cTACE has been a subject of growing importance in the era of precision oncology [10, 11]. Specifically, predicting recurrence after a complete response is as crucial as it affects the design of treatment planning [7, 8]. The aim of our study was to determine if lipiodol retention patterns could be used as an imaging marker for predicting recurrence in HCC lesions previously diagnosed as CR post-cTACE. Our study showed that almost all CR lesions with incomplete lipiodol retention had a recurrence later, while only one-fourth of lesions with complete lipiodol retention developed it.
Several publications have concentrated on the predictive significance of lipiodol retention patterns following cTACE. Kinugasa et al. [16] showed that early-stage HCC patients who have undergone cTACE are at a higher risk of recurrence if they have a heterogenous lipiodol pattern. Also, Minami et al. [17] showed that the accumulation of inadequate iodized oil on cone-beam CT after cTACE treatment was an adverse predictor for treated HCC lesions. Yang et al. [14] stated that compared to those with negative lipiodol deposition, patients who had positive lipiodol deposition in their portal vein tumor thrombus showed better overall survival rates. These results are in coincidence with our study suggesting that the appearance of lipiodol uptake on follow-up CT has a predictive role in expecting recurrence.
Our study categorized lipiodol retention patterns into C-Lip and I-Lip. A number of different categorizations have been suggested by a number of studies [18,19,20]. One of the early trials was the pictorial essay which classified iodized oil patterns into four types: homogeneous accumulation, partial defective accumulation, faint accumulation, and no or slight accumulation [18]. Another study suggested a 5-grade scale system for evaluating by visual assessment of the percentage of uptake [19]. A study identified homogeneity, sparsity, and rim deposition as the three imaging features used to characterize the overall pattern of each lesion [20]. Being clear, simplified, and feasible, our study adopted the classification of Burgio et al. [21].
As our study was conducted on 21 lesions with C-Lip and 9 lesions with I-Lip, the difference in uptake pattern between different lesions could be explained by the fact that lipiodol is administered intra-arterially, so the more vascularized the lesion the higher lipiodol deposition, while avascular, necrotic, or fibrotic nodules fail to take up lipiodol. Incomplete catheterization of tumor feeders and arterioportal shunts in large HCCs may hinder retention [22].
Top of form
The study was dependent on DCE-MRI as a gold standard for following treatment response post cTACE in order to assess the predictivity of CT-based lipiodol retention pattern. MRI has been proposed by certain authors as an alternative tool to CT for evaluating tumor response post-cTACE. The study conducted by Hunt et al. [23] indicates that MR imaging is more accurate than CT imaging for post-TACE follow-up in terms of overall accuracy, sensitivity, and specificity for identifying viable tumors. While MR is deemed more precise than CT in identifying tumoral remnants due to the absence of lipiodol retention, CT is still the preferred imaging method for follow-up after chemoembolization due to its availability, affordability, and simplicity. Most of the teams still routinely perform CT alone for follow-up imaging after TACE treatment. CT is recommended over MRI for evaluating lipiodol accumulation, recommending the use of MRI primarily for patients with hypersensitivity to iodinated contrast agents or when CT-based evaluation of residual tumor can’t be achieved [24].
Study results underscored the clinical relevance of the lesion's largest diameter as a potent predictor of recurrence with a cut-off point > 28mm. This result coincided with the study stated that in patients with HCC sizes less than 3cm, the achievement of radiological CR after TACE can be predicted significantly by complete lipiodol retention and the absence of residual tumor enhancement, unlike HCC sizes greater than 3 cm [22]. Also, our study revealed that non-capsulation as a predictor factor of recurrence, which is supported by a study that proved that lesions of HCC that exhibit a well-defined and encapsulated morphology, demonstrate a superior response to TACE in comparison to non-capsulated and infiltrative lesions [25]. Selective treatment, compared to superselective one, also exhibited a significant impact on recurrence. This result is advocated by publication showed that superselective cTACE conducted with a microcatheter placed as close to the tumor as feasible; improves outcomes by maximizing anti-tumoral action while reducing collateral harm to the adjacent liver tissue [26].
The remarkable result of our study was the emergence of incomplete lipiodol retentsion as a particularly powerful predictor for recurrence post-CR. Incomplete lipiodol retention displayed the strongest association with recurrence among other factors, with 95% CI (2.544–257.566) underscoring the robustness of this association. Thus, our study emphasized that lesions with incomplete lipiodol retention, even previously diagnosed CR post-cTACE, should now be considered incompletely treated and may require another imaging modality or a second TACE session.
The results of our study provided important insights into the performance of the lipiodol retention pattern in predicting recurrence. With a sensitivity of (61.5%), lipiodol retention patterns were fairly sensitive in detecting cases where recurrence is present. However, the specificity was quite high (94.12%), indicating high accuracy in identifying cases of complete lipiodol retention without recurrence.
Considering PPV of (88.9%), this was a strong indicator of the reliability of patterns in predicting recurrence, meanwhile, NPV of (76.19%) was reasonably high.
An accuracy of 80% indicated a reasonably good performance of lipiodol retention patterns in predicting recurrence. However, there is room for improvement, especially in increasing sensitivity. Further research and potentially refining the test methodology could enhance its clinical utility for this specific outcome.
Our study was a multicentric prospective study design; however, it had many limitations. The sample size was relatively small compared with the majority of studies; this can be explained by our narrow inclusion criteria. We didn’t focus on overall survival. To accurately assess progress, we limited our study to patients with a maximum of three tumors, as assessing progression in multifocal HCC cases would be too challenging.
Conclusions
Complete lipiodol retention in HCCs with CR has a reduced susceptibility for recurrence and, thereby will potentially benefit from DCE-MRI during subsequent evaluations. Conversely, the presence of incomplete lipiodol retention is an indication of a high risk of recurrence and may require earlier or another plan of treatment.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BCLC:
-
Barcelona clinic liver cancer
- CECT:
-
Contrast-enhanced computed tomography
- CT:
-
Computed tomography
- C-Lip:
-
Complete lipiodol retention
- CR:
-
Complete response
- cTACE:
-
Conventional transarterial chemoembolization
- DCE-MRI:
-
Dynamic contrast-enhanced magnetic resonance imaging
- HCC:
-
Hepatocellular carcinoma
- I-Lip:
-
Incomplete lipiodol retention
- LI-RADS:
-
Liver imaging reporting and data systems
- mRECIST:
-
Modified response evaluation criteria in solid tumors
- PD:
-
Progressive disease
References
Reghupaty SC, Fisher PB, Sarkar D (2021) Hepatocellular carcinoma (HCC): epidemiology, etiology and molecular classification. Adv Cancer Res 149(1):1–61
Han K (2015) Transarterial chemoembolization in hepatocellular carcinoma treatment: barcelona clinic liver cancer staging system. World J Gastroenterol 21(1):10327–10335
Galle PR, Forner A, Llovet JM et al (2018) EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 69(1):182–236
Sahani D, Hayano K, Lee S (2015) Imaging for assessment of treatment response in hepatocellular carcinoma: current update. Indian J Radiol Imaging 25(2):121–128
Bargellini I, Bozzi E, Campani D et al (2013) Modified RECIST to assess tumor response after transarterial chemoembolization of hepatocellular carcinoma: CT–pathologic correlation in 178 liver explants. EMJ Radiol 82(1):E212–E218
Kim BK, Kim SU, Kim KA et al (2015) Complete response at first chemoembolization is still the most robust predictor for favorable outcome in hepatocellular carcinoma. J Hepatol 62(6):1304–1310
Young S, Sanghvi T, Sharma S et al (2022) Local recurrence following complete radiologic response in patients treated with transarterial chemoembolization for hepatocellular carcinoma. Diagn Interv Imaging 103(3):143–149
Jeong SO, Kim EB, Jeong SW et al (2017) Predictive factors for complete response and recurrence after transarterial chemoembolization in hepatocellular carcinoma. Gut Liver 11(3):409–416
Kim D, Clark P, Heimbach J et al (2014) Recurrence of hepatocellular carcinoma: importance of mRECIST response to chemoembolization and tumor size. Am J Transpla 14(6):1383–1390
Guo Z, Zhong N, Xu X et al (2021) Prediction of hepatocellular carcinoma response to transcatheter arterial chemoembolization: a real-world study based on non-contrast computed tomography radiomics and general image features. J Hepatocell Carcinoma 8(1):773–782
Wang Z, Wei J (2019) Establishment of a predictive model for short-term efficacy of transcatheter arterial chemoembolization treatment in hepatocellular carcinoma and its clinical application. J Cancer Res Ther 15(4):941–946
Chen CS, Li FK, Guo CY et al (2016) Tumor vascularity and lipiodol deposition as early radiological markers for predicting risk of disease progression in patients with unresectable hepatocellular carcinoma after transarterial chemoembolization. Oncotarget 7(1):7241–7252
Burgio MD, Ronot M, Bruno O et al (2016) Correlation of tumor response on computed tomography with pathological necrosis in hepatocellular carcinoma treated by chemoembolization before liver transplantation. Liver Transpl 22(1):1491–1500
Yang Z, Zou R, Zheng Y et al (2019) Lipiodol deposition in portal vein tumor thrombus predicts treatment outcome in HCC patients after transarterial chemoembolization. EMJ Radiol 29(1):5752–5762
Lencioni R, Llovet J (2010) Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis 30(1):52–60
Kinugasa H, Nouso K, Takeuchi Y et al (2011) Risk factors for recurrence after transarterial chemoembolization for early-stage hepatocellular carcinoma. J Gastroenterol 47(1):421–426
Minami Y, Takita M, Tsurusaki M et al (2016) Semiquantitative prediction of early response of conventional transcatheter arterial chemoembolization for hepatocellular carcinoma using postprocedural plain cone-beam computed tomography. Hepatol Res 47(3):E113–E119
Lim HK, Jeong Y, Kang HK et al (2006) Imaging features of hepatocellular carcinoma after transcatheter arterial chemoembolization and radiofrequency ablation. AJR Am J Roentgenol 187(4):W341–W349
Gaba RC, Lewandowski RJ, Hickey R et al (2016) Transcatheter therapy for hepatic malignancy: standardization of terminology and reporting criteria. J Vasc Interv Radiol 27(1):457–473
Stark S, Wang C, Savic LJ et al (2020) Automated feature quantification of lipiodol as imaging biomarker to predict therapeutic efficacy of conventional transarterial chemoembolization of liver cancer. Sci Rep 10(1):18026
Burgio MD, Sartoris R, Libotean C et al (2019) Lipiodol retention pattern after TACE for HCC is a predictor for local progression in lesions with complete response. Cancer Imaging 19(1):75
Lee SW, Lee TY, Cheng YC et al (2021) The Correlation with tumor radiological characteristics and prognosis of patients with early-stage hepatocellular carcinoma receiving transcatheter arterial chemoembolization. Medicine 100(26):E26414
Hunt SP, Yu W, Weintraub JL et al (2009) Radiologic monitoring of hepatocellular carcinoma tumor viability after transhepatic arterial chemoembolization: estimating the accuracy of contrast-enhanced cross-sectional imaging with histopathologic correlation. J Vasc Interv Radiol 20(1):30–38
Cho Y, Choi JW, Kwon H et al (2023) Transarterial chemoembolization for hepatocellular carcinoma: 2023 Expert Consensus-based practical recommendations of the Korean Liver Cancer Association. Korean J Radiol 24(7):606–625
Zhang W, Xu A, Wang W et al (2019) Radiological appearance of hepatocellular carcinoma predicts the response to transarterial chemoembolization in patients undergoing liver transplantation. BMC Cancer 19(1):1041
Baere T, Ronot M, Chung JW et al (2022) Initiative on superselective conventional transarterial chemoembolization results (INSPIRE). Cardiovasc Intervent Radiol 45(1):1430–1440
Acknowledgements
No Acknowledgements.
Funding
This research did not receive specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MS, ES and AS wrote the manuscript and is responsible for correspondence to journal. MS, WA and ES collected patient data and was responsible for image processing and collection of patient’s images. ES and MS, WA and AS participated in the design of the study and performed the statistical analysis. TK, ES, WA and AS conceived of the study and participated in its design and coordination, and was responsible for the review of the draft from a clinical point of view. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of the National liver institiuiue with ethical committee approval dated 6-2022, with serial number 6/22. Informed written consent was taken from all subjects.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within this study.
Competing interests
No financial or non-financial competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sweed, E.M., Moustafa, M.S., Shafei, A.S. et al. Value of computed tomography-based lipiodol retention pattern in the assessment of hepatocellular carcinoma complete response following conventional transarterial chemoembolization. Egypt J Radiol Nucl Med 55, 19 (2024). https://doi.org/10.1186/s43055-024-01187-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01187-1