
Abstract
Background
Acrometastases are accounted for a very small proportion of bone metastases. Lung cancer is the most common acrometastasis origin, and it often has a poor prognosis. The aim of the present cases is to describe the probability of an acrometastasis in the differential diagnosis of finger lesions and to emphasize the importance of taking local views of extremity of complaint for proper interpretation in such patients.
Case presentation
Here we reported two patients with metastases to the fingers with occult primary lung carcinoma and a history of prior lung malignancy, respectively. First case was a 58-year-old man with history of pain and swelling in the fourth finger of his left hand. He underwent an amputation from the metacarpophalangeal level and the pathological diagnosis was metastatic NSCLC. The second case was a 65-year-old ex-smoker man with a history of prior lung cancer (adenocarcinoma) suffered from a swollen, erythematous, painful tip of the right third finger. Phalangectomy was performed and the histological examination of the amputated part revealed the presence of a metastatic differentiated carcinoma of pulmonary origin.
Conclusions
When assessing the masses located at fingers, possibility of a solitary metastatic lung lesion should be considered.
Similar content being viewed by others

Background
The malignant lesions detected in bone tissue often originate from the prostate, lung, breast, kidney and gastrointestinal tract tissue [1]. Any location in the skeletal system can be involved, but only 0.007–0.3% of these metastases are located in the hand or foot [2]. Acrometastasis, as the first manifestation of a malignancy, is extremely rare, with a poor prognosis. The mean survival is about 5–6 months [3]. Forty-four per cent of all acrometastases originate from primary lung tumours, and metastases to the digits are seen in 0.2% of lung cancer patients [4, 5]. After clinical staging, radiotherapy and amputation are the most common therapeutic options for pain palliation. The aim of the present cases is to describe the probability of an acrometastasis in the differential diagnosis of finger lesions and to emphasizing the importance of taking local views of extremity of complaint for proper interpretation in such patients.
Case presentation
Case 1
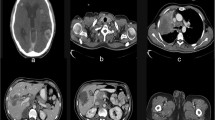
A 58-year-old man was admitted to the rheumatology department with a three months history of pain and swelling in the fourth finger of his left hand. He was smoker (40 pack-years), and he did not have any chronic diseases requiring regular medication. Upon physical examination, the fourth digit of his left hand was swollen and painful (Fig. 1A). The magnetic resonance imaging (MRI) of the left upper extremity showed soft tissue destruction measuring approximately 30 × 17 mm on the distal part of the fourth proximal phalanx of his left hand (Fig. 1B, C). The blood flow phase and blood pool images of the three-phase 99m methylene diphosphonate (99m Tc MDP) bone scan revealed increased radiotracer uptake in the fourth finger, and a focal retention of the radiotracer in the middle region of the fourth finger of the left hand, respectively (Fig. 1D–F). In the delayed images, a photopenic area could be seen in the proximal phalanx of the fourth finger of the left hand that resembled a “lytic” metastasis (Fig. 1G). The tracer uptakes in other bones (in wrist and tibias) were not typical of metastases (Fig. 1D, G).

A Enlargement on his fourth digit of left hand. B, C MRI findings of 30 × 17 mm destruction on the distal part of fourth proximal phalanx of left hand. DHypertrophic osteoartropathy in both tibiae. E, F Blood flow phase and blood pool images of three phase bone scan following right arm injection of the radiotracer Technetium-99m methylene diphosphonate (MDP) revealed increased radiotracer uptake in the fourth finger and a focal retention of the radiotracer in the middle region of the fourth finger. G Diffuse increased uptake at the left wrist and a photopenic area in proximal phalanx of the ourth finger is seen H 25 × 21 mm lobulated contour lesion in the posterior segment of right lower lobe on CTT. I The axial fused PET/CT image with a maximum ıntensity prejection (MIP) image showing intensely FDG avid right lower lobe mass and the ipsilateral nodal FDG uptakes in the right tracheobronchial and right hilar lymphadenopathies
The chest x-ray revealed a consolidated area in the right lower zone. The contrast-enhanced computed tomography (CT) of the thorax revealed a 25 × 21 mm lobulated contour lesion in the posterior segment of the right lower lobe (Fig. 1H). A CT-guided biopsy was performed, and the pathological examination showed non-small cell lung carcinoma (NSCLC)-not otherwise specified (NOS). A positron emission tomography (PET) CT was taken during the staging process, and a 24 × 27 × 24 mm mass with a maximum standardized uptake value (SUVmax) of 9.85 in the right lower lobe and right tracheobronchial and right hilar lymphadenopathies of 13 mm in diameter were detected (SUVmax: 7.51) (Fig. 1I). The cranial MRI was negative for metastasis. This patient was staged as T1bN2M1b according to the 7th lung cancer Tumour, Node and Metastasis (TNM) classification and staging system. The patient was diagnosed with oligometastatic disease due to the absence of distant metastases, with the exception of the fourth finger of his left hand.
This patient was referred to the orthopaedics department, and he underwent an amputation from the metacarpophalangeal level. The pathological diagnosis was metastatic NSCLC-NOS harbouring anEGFR 21L858R mutation. After undergoing curative treatment for the acrometastasis, concurrent chemoradiotherapy was planned to treat the primary lung cancer as a therapeutic approach.
Case 2
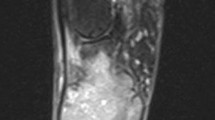
A 65-year-old ex-smoker man with a history of prior lung cancer (adenocarcinoma) suffered from a swollen, erythematous, painful tip of the right third finger was presented. Clinical examination revealed a palpable mass at the proximal part of the third finger of the right hand. Finger was tender and swollen without any trauma. Flexion and extension movements of the finger were painful. There was no neurovascular deficit. He was referred to the Nuclear Medicine Department for a 99m Tc-MDP bone scintigram to exclude metastasis. The blood flow phase and blood pool images of the three-phase bone scan with Tc 99m-MDP demonstrated increased radiotracer uptake at the distal part of the third finger of the right hand. The delayed images, prominently in the local views of the hands, demonstrated hyper-accumulation at the middle phalanx of the third finger of the right hand (Fig. 2A). Increased focal uptake at 5th rib was primarily assessed as secondary to a recent trauma described by the patient. The slightly increased tracer activity in lateral parts of the distal extremities was considered as hypertrophic osteoarthropathy (Fig. 2B). The findings were consistent with abnormal osteoblastic process suggesting probable osteoblastic acrometastasis.

A Blood Flow phase and Blood pool images of three phase bone scan in anterior local projection of the hands. Hypervascular lesion is seen in the proximal part of the third finger of the right hand (arrow). Delayed image after 3 h anterior view of hands demonstrating increased localization of tracer in middle phalanx of the third finger of the right hand (arrow). B In routine whole body bone scans, no additional focus that could be considered consistent with metastasis was detected. C Right hand radiography showing lytic destruction of the third middle phalanx with surrounding soft tissue enlargement (arrow)
The plain radiographic views of the right hand revealed a lytic destruction of his third middle phalanx with enlargement of surrounding soft tissue (Fig. 2C). MRI was not performed in that patient. With the consent of the patient, phalangectomy was performed. The histological examination of the amputated part revealed the presence of a metastatic differentiated carcinoma of pulmonary origin. The lytic appearance of the phalanx on x-ray image aided us in the differential diagnosis. Postoperative pathology supported bone scintigraphy findings in terms of metastasis, as well. After surgery he recovered well and did not receive any other treatment but he did not survive.
Discussion
The skeletal system is involved in more than 50% of all cancers. After the lung and liver, the bones are the third most common site for metastatic spreading [6]. The spine, pelvis, ribs, skull and proximal parts of the long bones are the most affected localizations [7]; however, acrometastases of the hands are rare which account for 0.1% of all metastatic bone lesions [8] Forty-seven percent of all cancers with hand metastases originate in the lungs. Kidney (13%) and breast (12%) carcinomas are the other most common primary origins reported in the literature [8].
Acrometastases may be caused from primary tumour progression or may be seen as the first sign of an unknown malignancy [9]. It is commonly associated with advanced lung cancer, and rarely, it can be the first symptom of any carcinoma [8, 10]. So, it is important to consider a finger lesion that can be a manifestation of an occult primary tumour.
When a local lesion that is suspected to be a malignancy is detected, a systemic physical investigation is essential to reach an accurate diagnosis. Our first case was initially admitted to the rheumatology clinic with complaints of finger pain; however, as a result.
of the multisystem clinical evaluation, a lung malignancy was diagnosed as the origin of the disease.
Usually, the symptoms and signs are nonspecific, like oedema, hyperaemia, ulcerated lesions and pain, which are the most common clinical signs [11]. Since they can mimic other infective-inflammatory processes such as paronychia, osteomyelitis, septic arthritis, gout, rheumatoid arthritis or tenosynovitis reflex symphatic dystrophy [9] and are seen rarely, possibility of acrometastases cannot be firstly considered by the physicians that encountered such lesions. Our cases presented with similar symptoms: pain and swelling.
Tc-99m MDP bone scan is widely used in evaluation of detecting skeletal metastases in variety of primary neoplasms. Radionuclide bone scanning provides the imaging of the whole skeleton that let the clinicians to identify oligoacrometastasis [12,13,14]. Similar case reports of metastatic lesions from different malignancies to hand or foot have been reported in the literature, but bone scintigrams of oligoacrometastases rarely reported [15, 16]. Since peripheral tracer uptakes can be unremarkable or can be dismissed on routine whole body bone scans, local views of extremity of complaint should be taken for proper interpretation in such patients. Luke et al. illustrated a solitary phalangeal metastasis of renal carcinoma by emphasizing the need for including the extremities in a standard whole-body study [16].
There is a male predominance in acrometastasis, and finger involvement is expected more often than toe involvement [8]. The leading primary neoplasm of hand and foot acrometastases are bronchogenic carcinomas and gastrointestinal or genito-urinary tract neoplasms, respectively [17]. It is usually unilateral, bilateral involvement has rarely been reported, and it usually effects the dominant hand [8, 18]. The distal phalanx and the third finger are the regions most affected by bone metastases [19]. When compared to the literature, the current patients were both male smokers and the finger metastasis was unilateral in both. However, non-dominant hand was involved in the first case unexpectedly. Acrometastases frequently accompany other organ metastases in lung cancer cases, and they have poor prognoses, with a median survival of 6 months [5]. Some cases may have distant metastases together with acrometastasis. For example, in the literature, a 56-year-old female patient presented with pain in the right hand middle finger and other distant metastasis was reported [20]. Unlike the literature, distant metastases were not detected in our first patient, with exception of the acrometastasis. Hovever, in the second case liver metastases on abdominal ultrasonagraphy (USG) was detected at follow-up.
Amputation is applied for pain palliation in the available terminal lesions of the hand, and it is often recommended for patients who have distal phalanx involvement [9]. Other than amputation, radiotherapy, excision and systemic therapy are the other treatment modalities used for acrometastases. The remaining treatment methods are frequently recommended for proximal lesions in the hand [5, 9]. Radiotherapy is an effective and noninvasive treatment for pain palliation, and it permits the patient to regain complete use of their hand, which improves the patient’s quality of life. The symptoms resolved in our patients after amputation, and they did not require further treatment. For the first case, after treating the oligometastasis, curative treatment was performed for the primary lesion. The second case did not receive any additional therapy after hand surgery and unfortunately, he did not survive.
Conclusions
In these cases, we want to remind the clinicians that when assessing the masses located at fingers, possibility of a solitary metastatic lung lesion should be considered. In the light of multisystemic approach and imaging findings, early diagnosis and adequate treatment are important for improving both the patient’s quality of life and life expectancy.
Availability of data and materials
Not applicable.
Abbreviations
- CT:
-
Computed Tomography
- MI:
-
Magnetic Resonance Imaging
- SUVmax:
-
Maximum standardized uptake value
- TNM:
-
Tumour, Node and Metastasis
- 99m Tc MDP:
-
99m technetium-methylene diphosphonate
- NSCLC:
-
Non small cell lung carcinoma
- NOS:
-
Not otherwise specified
- PET:
-
Positron Emission Tomography
- USG:
-
Ultrasonagraphy
References
Soylemez S, Demiroglu M, Yayla MA, Ozkan K, Alpan B, Ozger H (2015) Lung metastasis mimicking fingertip ınfection. Case Rep Oncol Med 2015, Article ID 708789
Veenendaal LM, Klerk G, Velde D (2014) A painful finger as first sign of a malignancy. Geriatr Orthop Surg Rehab 5(1):18–20
Mollet TW, Garcia CA, Koester G (2009) Skin metastases from lung cancer. Dermatol Online J 15(5):1
Kumar PP (1975) Metastases to the bones of the hand. J Natl Med Assoc 67(4):275–276
Flynn CJ, Danjoux C, Wongetal J (2008) Two cases of acrometastasis to the hands and review of the literature. Curr Oncol 15(5):51–58
Hage WD, Aboulafia AJ, Aboulafia DM (2000) Incidence, location, and diagnostic evaluation of metastatic bone disease. Orthop Clin North Am 31(4):515–528
Silverberg E (1986) Cancer statistics. CA Cancer J Clin 36:9–25
Libson E, Bloom RA, Husband JE (1987) Metastatic tumours of bones of the hand and foot. A comparative review and report of 43 additional cases. Skelet Radiol 16(5):387–392
Abrahams TG (1995) Occult malignancy presenting as metastatic disease to the hand and wrist. Skelet Radiol 24(2):135–137
Apollonatou V, Loukides S, Papaioannou AI, Papiris S (2018) Acrometastasis due to lung adenocarcinoma. Adv Respir Med 86(2):97–100
Healey JH, Turnbull AD, Miedema B, Lane JM (1986) Acrometastases. A study of twenty-nine patients with osseous involvement of the hands and feet. J Bone Jt Surg Am 68(5):743–746
Van den Wyngaert T, Strobel K, Kampen WU, Kuwert T, van der Bruggen W, Mohan HK, Gnanasegaran G, Delgado-Bolton R, Weber WA, Beheshti M, Langsteger W, Giammarile F, Mottaghy FM, Paycha F (2016) The EANM practice guidelines for bone scintigraphy. Eur J Nucl Med Mol Imaging 43:1723–1738
Krüger S, Buck AK, Mottaghy FM et al (2009) Detection of bone metastases in patients with lung cancer: 99mTc-MDP planar bone scintigraphy, 18F-fluoride PET or 18F-FDG PET/CT. Eur J Nucl Med Mol Imaging 36:1807–1812
Davila D, Antoniou A, Chaudhry MA (2015) Evaluation of osseous metastasis in bone scintigraphy. Semin Nucl Med 45:3–15
Li W, Li W, Zhang R (2016) Metastasis to the medial cuneiform bone from squamous cell carcinoma of the lung revealed by bone scintigraphy. Clin Nucl Med 41:946–947
Sonoda LI, Halim MY, Balan KK (2011) Solitary phalangeal metastasis of renal cell carcinoma on bone scintigram. Clin Nucl Med 36(3):237–239
Baran R, Tosti A (1994) Metastatic carcinoma to the terminal phalanx of the big toe: report of two cases and review of the literature. J Am Acad Dermatol 31:259–263
Ioia JV, Sumner JM, Gallagher T (1984) Presentation of malignancy by metastasis to the carpal navicular bone. Clin Orthop Relat Res 188:230–233
Flynn CJ, Danjoux C, Wong J et al (2008) Two cases of acrometastasis to the hands and review of the literature. Curr Oncol 15:51–58
Asirvatham Gjorup C, Ottesen SS, Gjerloff C (2017) Acrometastasis as the first sign of an occult non-small cell carcinoma of lung. J Plast Surg Hand Surg 51(2):156–157
Acknowledgements
Not applicable.
Metehan Karaca: Formerly he was Working at Ankara Atatürk Chest Disease and Thoracic Surgery Training and Research Hospital, Ankara, Turkey.
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by IUB, UY, PAK. ET, OO, and YA. Literature search was performed by FC, TIC, DK. and MK. The first draft of the manuscript was written by IUB and PAK. All authors reviewed and commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Informed constent was taken from the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uslu Biner, I., Akin Kabalak, P., Inal Cengiz, T. et al. A rare clinical presentation of lung cancer: two cases of solitary digital metastasis on Tc-99m MDP bone scan. Egypt J Radiol Nucl Med 54, 177 (2023). https://doi.org/10.1186/s43055-023-01109-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01109-7