
Abstract
Background
Trigeminal neuralgia (TN) is an electric-like recurrent pain of a sudden onset and is localized to the area supplied by the trigeminal nerve, and the patients are usually free in between the attacks. It’s one of the most common causes of facial pain and is commonly induced by mechanical irritation, and there’s strong evidence suggesting an insult at the trigeminal nerve root which is usually caused by a neurovascular compression. The aim of the study was to evaluate the role of diffusion tensor imaging (DTI) in the detection of microstructural changes of normal appearing trigeminal nerve in patients with trigeminal neuralgia and the correlation between DTI parameters and pain severity.
Results
Thirty one cases were included in the study (16 patients with TN and 15 healthy controls) underwent MRI with diffusion tensor imaging. The fractional anisotropy (FA) values of the trigeminal nerves were recorded and then comparison between the affected and unaffected sides in TN patients and healthy controls was done, also the degree of FA reduction was correlated with the pain severity in TN groups. The mean FA value of the affected trigeminal nerves was 0.43 ± 0.083, while that of the unaffected sides was 0.56 ± 0.058. The mean FA value of the trigeminal nerves in the healthy controls was 0.54 ± 0.057. A significant statistical differences was found between affected and unaffected sides (P < 0.00001) and between the affected sides and healthy controls (P < 0.0003), while no statistically significant difference was detected between the unaffected side and the healthy controls. A strong negative correlation was found between the pain score and the degree of FA reduction (P < 0.001).
Conclusions
Diffusion tensor imaging is a functional MRI technique which can detect the microstructural changes in the normal appearing trigeminal nerves in patients with trigeminal neuralgia with a strong negative correlation between the severity of pain and the degree of FA reduction of the affected trigeminal nerve.
Similar content being viewed by others


Background
Trigeminal neuralgia (TN) is characterized by recurrent very painful, electric-like pain of brief duration (between 2 s and 2 min), in the distribution of the trigeminal nerve that are abrupt in onset and termination and the patients are usually free in between the attacks [1]. It’s one of the most common causes of facial pain and is commonly induced by mechanical irritation and there’s a strong evidence suggesting an insult at the trigeminal nerve root which is usually caused by vascular loop from the superior cerebellar artery (neurovascular compression). Recognized risk factors for developing trigeminal neuralgia include hypertension, atherosclerosis, individual sensitivity and familial history [2, 3].
Different treatment options are available for trigeminal neuralgia including anticonvulsant medications as a first-line treatment option. In patients with persistent pain or unacceptable side effects from the medications may have other options including transcutaneous, percutaneous and open surgical options. Radiofrequency rhizotomy was first introduced to treat TN in 1974 [4], it can provide complete pain relief with lower side effects; however, a recurrence rate of 15–20% was noted within 12 months after therapy [5].
There’s a debate about the exact pathogenesis of trigeminal neuralgia. Several structural alterations in the trigeminal nerve resulting from vascular compression have been described, including demyelination at the root entry zone, atrophy or hypertrophy of peripheral axons and damage to Schwann cells and peripheral myelin. [6]. Also, some structural abnormalities were identified in large number of patients including deviation of the nerve and nerve atrophy [3].
MRI of patients with trigeminal neuralgia using high-resolution sequences such as 3D T2-weighted images and 3D T1-weighted gadolinium-enhanced images can depict the fine neurovascular anatomy of the trigeminal nerve and important in planning microvascular decompression [7]. However, the morphological and pathological changes of the TGN can be difficult to identify by conventional MRI sequences [3].
Diffusion tensor imaging (DTI) is a recently introduced functional MRI technique used for depiction of microstructural white matter changes of the brain. The most important DTI parameter is the FA (fractional anisotropy) which reflect the directionality of water molecules diffusion. Abnormalities of the white matter causing axonal damage and loss of organization produce lower FA values [8].
Recent studies demonstrated decreased fractional anisotropy (FA), increased radial diffusivity (RD) and apparent diffusion coefficient (ADC) in the affected side compared to the normal side; in spite of normal morphological appearance, thus depicting the microstructural abnormality by non-invasive means [2, 3].
In this study, our aim was to evaluate the role of DTI in the detection of microstructural changes of normal appearing trigeminal nerve in patients with trigeminal neuralgia and correlating the DTI findings with the pain severity.
Methods
Nineteen patients with TN (13 females and 6 males) were included in this cross-sectional analytic study which was performed in the period between March 2023 and June 2023. Three patients were excluded from the study, 2 patients who underwent neurovascular decompressive surgeries and one patient had trigeminal neuroma. The final cohort was 16 patients (11 females and 5 males) with repeated attacks of TN symptoms, diagnosed and classified according to visual analog pain scale (VAS). The age of the patients ranged from 27 to 57 years with the mean age was 41 ± 5.2. Fifteen age-matched healthy persons were also examined as a control group. They consisted of 10 females and 5 males, with their ages ranged from 19 to 48 years with a mean age of 38 ± 5.6.
All subjects participated in the study signed a written informed consent before the examination. Institutional review board (IRB) approval was also obtained.
Inclusion criteria: adult male or female patients complaining of trigeminal neuralgia without a history of previous interventions.
Exclusion criteria: Patients with history of herpes zoster infection, trigeminal neuroma (whether known history to have a tumour or incidentally discovered during the MRI examination) or any other diseases that can cause similar symptoms to TN, like maxillary sinusitis, toothache or internal derangement of temporomandibular joints were excluded from the study. Patients underwent neurovascular decompression surgery or having absolute contraindication to MRI were also excluded.
The patients included in the study were subjected to:
-
Clinical assessment by a neurologist with 15 years’ experience including the sex, age, duration of symptoms and pain laterality (right or left pain) were obtained.
-
Visual analogue pain scale (VAS): There are some difficulties in measurement of the degree of chronic pain in TN and related facial pain syndromes because of their subjective nature. Measurement of pain intensity or percent pain relief had been used for assessment and grading of TN [9, 10]. VAS is commonly used in assessment of pain in TN. The instrument consists of a 10 cm line at which 0 is representing “no pain” and 10 is representing “worst pain”. Each patient marks on this line the point at which he/she feels best represents their perception of pain (Fig. 1) [11].

The visual analog scale (VAS) [11]
MRI examination
MRI was performed for all patients and healthy controls using 1.5 T machine (Signa artist GE) with a standard head coil and without prior preparation or anaesthesia. The conventional sequences were obtained including axial T1, T2 and FLAIR covering the whole brain. 3D volumetric axial T1 GRE (BRAVO) and 3D axial T2 over the cerebellopontine angle were also obtained.
DTI was then acquired and consisted of a single shot, spin-echo echo planar sequence in 12 encoding directions using b value of 0 and 1000 s/mm2, a slice thickness of 2 mm, field of view was 210 mm and the matrix was 112 × 110. The time of repetition (TR) was 8000 ms, and the time of echo (TE) was 67 ms.
Post processing of the acquired images suing the available work station was then performed by 3 experienced radiologist with 14, 15 and 17 years’ experience in neuroradiology. Grey scale FA maps, directionality colour coded FA maps and 3D fibre tractography of the trigeminal nerves were obtained.
Thirty two trigeminal nerves were examined in the 16 patients (categorized as affected and unaffected sides). Regions of interest (ROIs) were assigned for trigeminal nerves over the area of the root entry zone (REZ). FA values were measured for the right and left trigeminal nerves. Drawing of the regions of interest (ROIs) were made at the FA map overlaid on axial T2 images. The voxels for each ROI were between 3 and 7. We used the manual multi-ROI technique for 3D fibre tracking and the software algorithm tracked the trigeminal nerves. We defined the pain side as “affected” and the other side as “unaffected”.
For the healthy controls, the FA of the right and left nerves was measured separately then the mean of both sides was calculated in each patient (Fig. 2).

Axial colour-coded FA map of a healthy 41-year old male control showing normal FA value of the trigeminal nerves (right 0.43 and left 0.45)
Comparison between FA of trigeminal nerves in the affected and unaffected sides was done in TN patients. Then, a comparison between the FA of trigeminal nerve in the healthy controls with those of trigeminal neuralgia patients (including the affected and unaffected sides) was done. Finally, the degree of FA reduction was correlated with degree of pain severity in TN patients.
Results
Thirty one subjects were included in the study (16 patients with TN and 15 healthy controls). The patients’ ages ranged between 27 and 57 years with a mean age of 41 ± 5.2, while the healthy controls ages ranged between 23 and 48 years with a mean age of 38 ± 5.6 (Table 1). Seven cases complained from left trigeminal neuralgia and nine cases complained from the right side.
All patients showed normal morphology of the trigeminal nerves in the conventional MRI sequences. Vascular loop compression from the superior cerebellar artery was found in 11 patients out of the 16 patients with TN (68.7%), while no obvious cause was detected in the other 5 patients (31.3%) (Figs. 3 and 4).

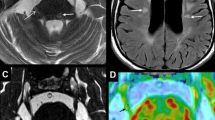
A 53-year-old female patient presented with right TN for 2 years. VAS was 6. A Axial T2 WI showing normal appearing right trigeminal nerve B Axial T2 WI showing the normal appearing left trigeminal nerve and C Axial T2 WI at a lower level showing a small vascular loop crossing the REZ of the right trigeminal nerve (arrow). D Axial colour-coded FA map overlaid on axial T2 images showing reduced FA value of the right trigeminal nerve (0.3) compared to the contralateral normal side (0.56) E 3D fibre tractography of both trigeminal nerves showing normal and comparable 3D tractography appearance of both nerves

A 39-year-old female patient presented with left TN for 4 months duration. Clinical assessment showed a pain score of 3. A Axial T2 WI showing normal appearing trigeminal nerves with a small vascular loop crossing the REZ of the left trigeminal nerve (arrow). B Axial colour-coded map showing normal colour intensity of both trigeminal nerves. C Axial FA map showing reduced FA value of the left trigeminal nerve (0.35) compared to the contralateral normal side (0.48) D 3D fibre tractography of both trigeminal nerves showing normal and comparable 3D tractography appearance of both nerves
It was found that the mean FA value of the affected trigeminal nerves was 0.43 ± 0.083, while that of the unaffected sides was 0.56 ± 0.058. The mean FA value of the trigeminal nerves in the healthy controls was 0.54 ± 0.057 (Table 2).
TN patients showed decreased FA values in the trigeminal nerve at the side of pain with significant statistical differences between the affected and the unaffected sides (P < 0.00001). This indicating microstructural changes in the nerve fibres in spite of normal morphological appearance in the conventional MR images.
Also, there was a statistically significant difference between the mean FA value of the affected nerves and the FA values of the trigeminal nerves in healthy controls (P < 0.0003). On the other hand, no significant differences were found between the mean FA values of the trigeminal nerves of the unaffected side and the healthy controls (P 0.2308).
According to the Visual analogue pain scale, the pain score of the TN patients ranges between 2 and 7 with a mean of 4.5 ± 1.54. The duration of symptoms ranged from one month to three years with a mean of 8 ± 1.3 months.
By using Pearson's correlation coefficient as a measure of correlation between pain score and FA values, the results show that the correlation coefficient = − 0.876 with P-value equals \(<0.001\) indicating a significant high negative relationship between pain scores and the FA values. Besides, a simple linear regression model is used to estimate the relationship between pain scores and the FA values. The model is presented in Eq. 1 and its corresponding results are provided in (Table 3).
From above results: it was observed that for every one-unit increase in pain score, there is a corresponding (0.047) unit decrease in FA value. Also, based on the t-test of the pain score variable and its corresponding P-value (\(<0.001\)), we conclude that pain score has statistically significant effect on FA value. Hence, the estimated model is:
Discussion
Trigeminal neuralgia is recognized as recurrent electric-like pain of a sudden onset and is localized to the area supplied by the trigeminal nerve (TGN), and the patients are usually free in between the attacks [1]. The purpose of this study was to assess the value of diffusion tensor MR imaging in patients with trigeminal neuralgia and to correlate the DTI findings with the pain severity.
A significant statistical difference was found between the FA values in the trigeminal nerve at the pain side and that of the unaffected side (P < 0.00001) and those of the normal healthy controls (P < 0.0003) indicating microstructural changes in the nerve fibres in spite of normal morphological appearance in the conventional MR images. Our results matched with previous studies including Chen et al. [2] who studied 37 patients with TN and found that the FA of the affected side were significantly lower than those of the unaffected side (P = 0.012). Also, our results agreed with another study done by DeSouza et al. [12] who performed DTI scans in 18 right-sided TN patients and 18 healthy control and it was found that the affected trigeminal nerves had lower FA compared to controls. Also, the study done by Lutz et al. [13] over 81 patients with TN underwent DTI and revealed significantly lower FA values within the vulnerable zone of the affected trigeminal nerve compared with the contralateral side. Similar findings were detected in several previous studies as well [14,15,16].
In the current study, a significant high negative relationship between pain scores and the FA values were detected with P < 0.001. Studies correlating the DTI findings with pain score are relatively sparse. However, our results agreed with the results of Wu et al. [17] who found the decline rate of FA was significantly correlated with VAS scores and symptom duration (the decline of FA was negatively correlated with VAS and symptom duration). Also, our results agreed with Wang et al. [18] who studied a total of 17 patients with TN and it was found that the FA value of the diseased side was negatively correlated with VAS (P = 0.018).
In the study done by Moon et al. [19] over 14 patients with TN underwent DTI using 7.0 Tesla MRI. They found that, in patients with TN, affected sides showed significantly decreased FA compared with unaffected trigeminal nerves which agreed with our results, however upon examining the associations between DTI parameters and clinical characteristics for patients with TN, no statistical correlation were detected. Another pain score was used “Barrow Neurological Institute (BNI)” in their study. Also in the study of Lutz et al. [13], no correlation was found with the duration of symptoms or severity of compression. Luo et al. [20] also found a significant statistical difference in the DTI and DSI parameters between the affected and unaffected sides and those of healthy controls; however, there was no significant statistical difference found between the MRI findings and the VAS pain score.
The study has some limitations that necessitate further investigations. One of the limitation is the relatively small sample size. Another limitation is that all the study group has short symptom duration (less than 3 years). Further studies with larger number of patients and more variations the disease duration and degree of pain is recommended.
Conclusions
Diffusion tensor imaging is a functional MRI technique which can detect the microstructural changes in the normal appearing trigeminal nerves in patients with trigeminal neuralgia with a strong negative correlation between the severity of pain and the degree of FA reduction of the affected trigeminal nerve.
Availability of data and materials
All the datasets used and analysed in this study are available with the corresponding author on reasonable request.
Abbreviations
- BNI:
-
Barrow Neurological Institute
- DSI:
-
Diffusion spectrum imaging
- DTI:
-
Diffusion tensor imaging
- FA:
-
Fractional anisotropy
- MRI:
-
Magnetic resonance imaging
- TN:
-
Trigeminal neuralgia
- REZ:
-
Root entry zone
- ROI:
-
Region of interest
- VAS:
-
Visual analog scale pain score
References
Lambru G, Zakrzewska J, Matharu M (2021) Trigeminal neuralgia: a practical guide. Pract Neurol 21(5):392–402
Chen ST, Yang JT, Weng HH et al (2019) Diffusion tensor imaging for assessment of microstructural changes associate with treatment outcome at one-year after radiofrequency Rhizotomy in trigeminal neuralgia. BMC Neurol 19(1):62
Leal PRL (2019) Fraction of anisotropy and apparent diffusion coefficient as diagnostic tools in trigeminal neuralgia. Acta Neurochir 161(7):1403–1405
Xu R, Xie ME, Jackson CM (2021) Trigeminal neuralgia: current approaches and emerging interventions. J Pain Res 14:3437–3463
Kanpolat Y, Savas A, Bekar A et al (2001) Percutaneous controlled radiofrequency trigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25-year experience with 1600 patients. Neurosurgery 48(3):524–534
Gambeta E, Chichorro JG, Zamponi GW (2020) Trigeminal neuralgia: an overview from pathophysiology to pharmacological treatments. Mol Pain 16:1744806920901890
Leal PRL, Hermier M, Souza MA et al (2011) Visualization of vascular compression of the trigeminal nerve with high-resolution 3T MRI: a prospective study comparing preoperative imaging analysis to surgical findings in 40 consecutive patients who underwent microvascular decompression for trigeminal neuralgia. Neurosurgery 69(1):15–26
Razek AAKA, El-Serougy L, Abdelsalam M et al (2018) Differentiation of residual/recurrent gliomas from postradiation necrosis with arterial spin labeling and diffusion tensor magnetic resonance imaging-derived metrics. Neuroradiology 60(2):169–177
Chen HI, Lee JY (2010) The measurement of pain in patients with trigeminal neuralgia. Clin Neurosurg 57:129–133
Rogers CL, Shetter AG, Fiedler JA et al (2000) Gamma knife radiosurgery for trigeminal neuralgia: the initial experience of The Barrow Neurological Institute. Int J Radiat Oncol Biol Phys 47(4):1013–1019
Kumar S, Rastogi S, Mahendra P et al (2013) Pain in trigeminal neuralgia: neurophysiology and measurement: a comprehensive review. J Med Life 6(4):383
DeSouza DD, Hodaie M, Davis KD (2014) Abnormal trigeminal nerve microstructure and brain white matter in idiopathic trigeminal neuralgia. PAIN® 155(1):37–44
Lutz J, Thon N, Stahl R et al (2016) Microstructural alterations in trigeminal neuralgia determined by diffusion tensor imaging are independent of symptom duration, severity, and type of neurovascular conflict. J Neurosurg 124(3):823–830
Chen DQ, DeSouza DD, Hayes DJ et al (2016) Diffusivity signatures characterize trigeminal neuralgia associated with multiple sclerosis. Mult Scler 22(1):51–63
Wilcox SL, Gustin SM, Eykman EN et al (2013) Trigeminal nerve anatomy in neuropathic and non-neuropathic orofacial pain patients. J Pain 14(8):865–872
Liu Y, Li J, Butzkueven H et al (2013) Microstructural abnormalities in the trigeminal nerves of patients with trigeminal neuralgia revealed by multiple diffusion metrics. Eur J Radiol 82:783–786
Wu M, Qiu J, Jiang X et al (2020) Diffusion tensor imaging reveals microstructural alteration of the trigeminal nerve root in classical trigeminal neuralgia without neurovascular compression and correlation with outcome after internal neurolysis. Magn Reson Imaging 71:37–44
Wang Y, Wang D, Wu Y et al (2023) A preliminary study of diffusion tensor imaging in root entry zone of primary trigeminal neuralgia. Front Neuroanat 17:1112662
Moon HC, You ST, Baek HM et al (2018) 7.0 Tesla MRI tractography in patients with trigeminal neuralgia. Magn Reson Imaging 54:265–270
Luo SP, Chen FF, Zhang HW et al (2022) trigeminal nerve white matter fiber abnormalities in primary trigeminal neuralgia: a diffusion spectrum imaging study. Front Neurol 12:798969
Acknowledgements
Not applicable.
Funding
Not applicable (no funding received for this study).
Author information
Authors and Affiliations
Contributions
SFE put the idea of the study, participation in the study design, FA measurements and DTI analysis. AAH helped in data collection, participation in MRI analysis and FA measurements. MEM helped in patients collection and clinical assessment. BEM editor of the manuscript, participated in DTI analysis and FA measurements and performed the statistical analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was signed by all patients before the examination. The study was approved by the research committee of faculty of medicine, Cairo University, 2023. Reference number N-125.
Consent for publication
All patients included in this research were fully conscious and older than 16-year old and gave written informed consent.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elkholy, S.F., Gadalla, A.A.E.H., Mohammad, M.E. et al. Diffusion tensor imaging in trigeminal neuralgia: beyond the normal morphology. Egypt J Radiol Nucl Med 54, 154 (2023). https://doi.org/10.1186/s43055-023-01102-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01102-0