
Abstract
Background
The Sickle cell disease (SCD) is a hemoglobinopathy that is recessively inherited commonly among people of Equatorial African, Saudi Arabian, and Mediterranean ancestry. It is characterized by chronic hemolytic anemia and intermittent vaso-occlusive events. The stroke is a common complication of SCD, which occurs in approximately 7% of children with SCD. The Transcranial Doppler ultrasonography is the only noninvasive examination that provides a reliable evaluation of intracranial blood flow patterns in real time with no need for sedation of the patient. The TCD can identify children with the highest risk of the first-ever stroke and those in need of prophylactic blood transfusion, as the blood transfusion is not in the protocol of management of SCD till now but just after complication occurrence. So, it is important to know if the chronicity and the regularity of the transfusion are useful or not.
Results
Sixty-nine patients diagnosed with sickle cell disease, recruited from the pediatric hematology outpatient clinic, over a period of 7 months, with age 2–13 years, examined by transcranial Doppler ultrasound. 44.9% of them were on regular blood transfusion, 39.1% occasionally transfused and 15.9% never transfused. Transcranial Doppler parameters of the cerebral arteries, namely TAMAX, PSV, were correlated with the frequency of transfusion and with (STOP) classification of the stroke risk. The Doppler parameters were also correlated with the different clinical parameters. The right MCA PSV and left DICA PSV were significantly higher among patients who were never transfused before. The Right DICA TAMAX was significantly higher among patients on regular transfusion, and the left DICA TAmax was significantly higher among patients who were never transfused before. Patients with high risk of stroke were diagnosed at a significantly older age. Regarding the laboratory parameters, platelets were significantly lower and total and direct bilirubin was significantly higher among the high stroke risk patients.
Conclusions
The regularity of the blood transfusion is extremely important in the stroke prevention. The most important velocities that may act as indicators for the risk are TAMAX of both DICAs and PSV of RT MCA & LT DICA.
Similar content being viewed by others


Background
Sickle cell disease (SCD) is one of the most common hematologic disorders associated with neurological disease in children [1].
Vasculopathy of the large intracranial arteries, such as the supraclinoid internal carotid artery (ICA), middle cerebral artery (MCA), and anterior cerebral artery (ACA), was first seen on conventional angiography in children with SCD and neurological sequelae in the 1970s [2]. The pathophysiology of vasculopathy consists of progressive damage to the basal intracranial arteries and cerebral microcirculation, while chronic anemia worsens exposure to cerebral hypoxia. It results in stroke and subclinical or poorly symptomatic ischemic lesions [3].Overt stroke occurs in up to 11% of children with SCD by age 18 and 24% by age 45 [4].
Silent cerebral infarctions (SCIs) can occur in newborns and preschoolers, despite the fact that the average age of occurrence of overt stroke is 7.7 years. Even in the absence of a history of clinical stroke, infarction and/or stenosis of the major cerebral arteries are common in very young children. Even when they are very young, children with SCI are at an increased risk of overt stroke and developing silent infarction. Intellectual ability and academic achievement are among the associated morbidities [5].
Transfusions can be used to treat specific episodes or to prevent life-threatening consequences in children with sickle cell disease. Ongoing transfusions can also assist children with sickle cell disease improve their height and weight [6].
Transcranial Doppler (TCD) has become an essential tool in the management of sickle cell anemia patients, recommended by the French Authority of Health and by the United States Department of Health and Human Services (type A, class I evidence). In children who have suffered a stroke, it detects arteriopathy with a sensitivity of 90% and specificity of 100% compared to cerebral angiography [7]. The most important application is in evaluation of stroke risk in neurologically asymptomatic sickle cell anemia patients. It was demonstrated that an abnormal TCD is linked to high risk of a first stroke, and that chronic transfusions reduce this risk [8].
Blood flow velocities in the major cerebral arteries measured by transcranial Doppler (TCD) are indicators of stroke risk in HbSS/HbSB0 children aged 2 to 16. Chronic red cell transfusions (CRT) with an intent of reducing hemoglobin S levels to less than 30% normalize TCD velocities in about 80% of patients and reduce the risk of primary stroke by 90%. Children who were withdrawn of CRT after 30 months had a higher rate of primary stroke [9]. TCD velocities can be reduced with hydroxyurea (HU), and a trial showed that young children at risk for stroke whose TCDs normalized on CRT could be gradually weaned off transfusion therapy and maintained on HU with stable TCD velocities [10].
Chronic red cell transfusions decreases the risk of stroke recurrence from 67 to 20% [11]. Hydroxyurea does not provide the same level of protection for secondary stroke prevention [12].
According to the French and United States guidelines, children with sickle cell anemia should be screened with TCD from the second year of life and then re-scanned annually until 16 years old if normal (i.e., highest TAMX of any artery < 170 cm/s), quarterly if conditional (TAMX of at least one artery 170–199 cm/s), and regular transfusions should be initiated in case of abnormal TCD (TAMX in at least one artery ≥ 200 cm/s) [13].
Methods
Study population
This study was conducted over a period of 7 months. It included sixty-nine sickle cell disease patients aged from 2 to 13 years old, attending at the pediatric hematology outpatient clinic. A verbal consent was obtained from the patients and their legal guardians before enrollment in the study.
We included patients diagnosed with sickle cell anemia established by hemoglobin electrophoresis whether transfusion or non-transfusion dependant. We excluded patients with CNS congenital anomalies, patients with history of previous stroke, and patients during the acute attack of sickling crisis or hemolytic attack.
The patients were allocated into three groups according to frequency of transfusion:
-
Group (A): 31 cases regularly blood transfused.
-
Group (B): 27 cases occasionally blood transfused.
-
Group (C): 11 cases never blood transfused before.
Clinical examination
Full history was taken with emphasis on age, sex, Age at diagnosis, frequency of transfusion in previously transfused patients, treatment with hydroxyurea among patients, and history of splenectomy or not.
Laboratory investigations
The laboratory data collected included hemoglobin (HB), hematocrit value (HCT), white blood cells count (WBCs), platelets, total serum bilirubin, and direct bilirubin levels.
Imaging
Transcranial Doppler was performed at the pediatric radiology department by one investigator using SAMSUNG HS 60 ultrasound machine, that is equipped by 2–3 MHz phased array probe.
The patient lies supine with lateral tilting of his head to either side during the examination. The two middle cerebral arteries (MCAs) were investigated using a trans temporal approach, where the probe was placed on the temporal aspect of the head, cephalad to the zygomatic arch and immediately anterior and slightly superior to the tragus of the ear in a transverse position. Then the probe is angulated anteriorly till we visualize the M1 segment of the middle cerebral artery.
When the circle of Willis becomes evident, the middle cerebral artery is directed laterally into the Sylvian fissure. Then, spectral wave analysis is done in M1 segment on both sides.
Then the anterior cerebral artery is investigated by directing the probe downward, forward, and medially, where the flow is away from the transducer. After angling the probe slightly inferior and posterior, the distal part of internal carotid artery is visualized, with color flow in direction to the transducer.
The transducer is slid posteriorly for the posterior cerebral artery, with color flow is detected in direction to the transducer in its initial part, then away from the transducer as it courses around the cerebral peduncle. After completing investigation on one side, we repeat the procedure on the other side after asking the child to turn the head to the opposite side.
The following parameters were measured on both sides (right and left sides):PSV (peak systolic velocity),EDV (end diastolic velocity),RI (resistive index) and TA.max (time average mean of maximum velocity).
According to the Stroke Prevention Trial in Sickle Cell Anemia (STOP) classification for the risk of stroke, the TAmax velocities of the patients were classified into 3 groups:
Group 1 TAmax < 170 cm/s normal (no risk).
Group 2 TAmax 170–200 cm/s conditional risk.
Group 3 TAmax > 200 cm/s high risk of stroke.
Statistical analysis
An Excel spreadsheet was established for the entry of data. The analysis was carried with SPSS software (Statistical Package for the Social Sciences, version 24, SSPS Inc, Chicago, IL, USA). Frequency tables with percentages were used for categorical variables and descriptive statistics (mean and standard deviation) were used for numerical variables. Either paired Student's t or Mann–Whitney tests were used to compare quantitative variables, while McNemar or McNemar–Bowker tests were used to analyze categorical variables. A p value < 0.05 is considered statistically significant.
Results
This prospective cross-sectional study was conducted on 69 patients with sickle cell anemia regularly attending the pediatric hematology outpatient clinic, and fulfilling the inclusion criteria.
Our patients consisted of 36 (52.2%) males and 33 (47.8%) females with male: female ratio being 1.09:1. Mean patients' age was 7.61 ± 3.98 years; with mean age at diagnosis was 12.24 ± 12.19 months 0.31 patients were on regular transfusion, 27 patients were occasionally transfused and 11 patients never transfused before.
Regarding the hematological workup, the mean WBCs was 10.73 ± 5.34 × 103/microliter, HB 8.23 ± 1.4 gm/dL, HCT 23.36 ± 4.22%, and for platelets 333.01 ± 124.82 × 103/microliter. The total serum bilirubin mean value was 2.13 ± 1.09 gm/dL, while the mean value for direct bilirubin was 0.42 ± 0.26 gm/dL. The detailed clinical data are explained in Table 1.
Table 2 demonstrates the PSV and TA max of different cerebral arteries among the studied patients. For the Middle cerebral artery (MCA), the mean PSV for the right one is 144.06 ± 28.9 cm/s and 149.45 ± 35.06 cm/s for left, while the mean TA.max 99.35 ± 22.39 cm/s for RT and 93.41 ± 31.64 cm/s for LT.
The Mean (RT& LT) PSV and TA.max for Distal internal carotid (DICA) were 135.20 ± 36.43 cm/s, 121.71 ± 37.83 cm/s, 94.90 ± 22.21 cm/s, and 85.74 ± 25.49 cm/s, respectively.
Moreover, the mean PSV of Anterior cerebral artery (ACA) was 135.48 ± 39.17 cm/s for right and 137.40 ± 56.96 cm/s for LT, while the mean TA.max 95.05 ± 31.33 cm/s for RT and 96.10 ± 42.09 cm/s for LT.
The Mean (RT& LT) PSV and TA.max for posterior cerebral artery (PCA) were 123.86 ± 45.15 cm/s, 120.21 ± 46.53 cm/s, 87.43 ± 30.45 cm/s, and 81.86 ± 30.08 cm/s, respectively.
Regarding the clinical parameters, we found no correlation between the regularity of the blood transfusion and the gender of the patients. Also, we found that 4 patients had splenectomy operation with no significant correlation between the splenectomy and the regularity of blood transfusion (P value is 0.344).
No significant correlation was found between the regularity of blood transfusion and the age of the patients, age at diagnosis or any of the hematological and serological parameters (namely total and direct bilirubin level).
Patients were divided according to frequency of blood transfusion to 3 groups
-
Never had transfusion
-
Occasional blood transfusion
-
Regular transfusion
The three groups were comparable regarding gender, age, age at diagnosis, hematological and biochemical parameters (Fig. 1). However, the right MCA PSV and left DICA PSV were significantly higher among patients who were never transfused before (p-0.023 and p = 0.021, respectively). On the other hand, the Right DICA TAmax was significantly higher among patients on regular transfusion (p = 0.015) and the left DICA TAmax was significantly higher among patients who were never transfused before (p = 0.014) as further demonstrated in Table 3.
-
Furthermore the patients were divided into three groups according to (STOP) classification for the risk of stroke (Table 4):
-
Conditional: 170–200 cm/s (Fig. 4)

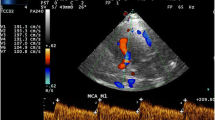
Transcranial Doppler for 7 years old female patient who never transfused showing the PSV within the distal ICA on the left side to be 307 cm/s and the TAMAX to be 224 cm/s (more than 200 cm/s) indicating the presence of high stroke risk

4 years old male patient on regular blood transfusion, Transcranial Doppler measurements showing no risk of stroke

6 years old female patient on occasional blood transfusion, Transcranial Doppler measurements showing right MCA TAmax of 147 cm/sec, left MCA TAmax of 145 cm/sec and Lt ACA TAmax of 209 cm/sec, parameters indicating high risk of stroke
There was no significant difference between the three groups regarding the age, however, patients with high risk of stroke were diagnosed at a significantly older age (p = 0.008). Regarding the laboratory parameters, platelets were significantly lower, while total and direct bilirubin were significantly higher among the patients with high risk stroke (p = 0.022, p = 0.025, p = 0.000, respectively) (Figs. 4, 5, and 6).

8 years old female patient on occasional blood transfusion, Transcranial Doppler measurements showing right MCA TAmax of 128 cm/sec, left MCA TAmax of 150 cm/sec, right ACA TAmax of 185 cm/sec and Rt DICA TAmax of 165 cm/sec, parameters indicating conditional risk of stroke

ROC curve for specificity and sensitivity between TCA Doppler and need for transfusion

Transcranial Doppler for a 10 years old male on occasional blood transfusion showing the TAMAX within the right MCA to be 108 cm/s (i.e., less than 170 cm/s),indicating no risk of stroke
Regarding the radiological parameters, the PSV of the right MCA, left MCA, left DICA, right ACA, Left ACA, and right PCA were significantly higher among the high risk stroke group (p = 0.004, p = 0.002, p = 0.003, p = 0.000, p = 0.004, respectively). Likewise, the TA max of the right MCA, Left MCA, Left DICA, right ACA, Left ACA, and right PCA were significantly higher among the high risk group (p = 0.005, p = 0.001, p = 0.000,p = 0.000, p = 0.000,and p = 0.001, respectively) as further shown in Table 4.
-
ROC curve for specificity and sensitivity is shown in Fig. 5
-
As shown in Table 5, there was a significant (p value < 0.05 specificity and sensitivity for RT MCA PSV, LT DICA PSV, RT DICA, TA.max, and LT DICA TA.max for detection the need for transfusion. The detailed area under curve is explained in Table 5.
Discussion
Sickle cell anemia is a qualitative genetic hemoglobinopathy caused by a single amino acid substitution in the beta globin chain of hemoglobin leading to expression of HbS [14]. It is one of the most common genetic diseases worldwide, with the East Mediterranean areas and the Middle East considered to be among the most heavily affected region with sickle cell disease burden [15]. In Egypt, it is highly common in the Oasis where the carrier rate ranges from 9 to 22% [16].
Stroke is one of the most severe complications of sickle cell disease (SCD), affecting children as well as adults, as reported by the Collaborative Study of Sickle Cell Disease (CSSCD) [17]. Silent cerebral infarcts are common among patients with sickle cell anemia. Around one quarter of the patients are expected to experience their first infarct before the age of six and 39% before the age [18].
This prospective cross-sectional study was conducted on 69 patients with sickle cell anemia regularly attending the at the pediatric hematology clinic and fulfilling the inclusion criteria aiming to assess the TCD velocities (TAmax and PSV) among patients with sickle cell disease who were classified into three variable blood transfusion groups (regular, occasional and never) and were taking hydroxyurea therapy with correlation to different clinical parameters.
The highest mean (TAmax) velocity recorded among our patients was 99.35 ± 22.39 cm/s and was noted in the right MCA. This is in accordance with the literature where the highest velocities are recorded in the right MCA [19.20,21] This velocity is comparable with that of healthy Egyptian children with recorded velocities of 92.15 ± 9.62 cm/s [22]. On the other hand, the least mean velocity was 81.86 ± 30.08 cm/s and was noted in the left PCA in comparison with DICA in two studies [19, 21].It is worth noting that the highest maximum (TAmax) velocity was 224 ± 42.09 cm/s and was recorded in the left ACA, this is in accordance with the study of [23], where the authors report stroke in two children with sickle cell disease and high blood flow velocity limited to the anterior cerebral artery and suggested that elevated velocity in this vessel may be associated with an increased risk of stroke.
According to (stop) classification for detection of stroke risk, TAmax measured in the arteries of the circle of Willis has been proven to detect SCD patients at high risk of developing ischemic stroke. Its significance in the prevention of stroke has also been widely acknowledged [24, 25]. Based on the STOP trial criteria the TAmax is used to classify patients into three risk groups: (1) no risk, when the TAmax is below 170 cm/s. (2) Conditional risk, when the velocity is between 170 and 199 cm/s carrying 7% risk of stroke. (3) High risk is seen when the TAmax is 200 m/s or over, conferring 40% risk of stroke to sufferers. The importance of this observation is that first stroke can be avoided in children at high risk by chronic transfusion, or hydroxyurea therapy. The prior studies reported up to 90% of first stroke might be prevented by prophylactic blood transfusion, and their study provided evidence for the efficacy of this approach in primary stroke prevention in children at risk [24,25,26,27].
Only 3 (4.3%) of our patients had abnormal velocities denoting high risk for stroke and 3 patients (4%) had a conditional risk for stroke, This finding is similar to that conducted by an Iranian study which detected that 3% of studied patients showed conditional and high risk stroke, respectively [28]. It is also similar to that reported by another study conducted on African population showing 3% with abnormal velocities > 200 cm/s [21]. However this contradicts several studies conducted on the American population that revealed 9.4% with high risk and 17.3% with conditional risk [29] and another French study that concluded 20.7% with high risk and 26.7% with conditional risk [30]. This could suggest regional or ethnic variations in the cerebral velocities. The reason for this low prevalence of high TCD velocities in African children with SCA is not clear and is interesting especially since we have a higher prevalence of stroke in Africa than in America [31], also contradicts the study of Lagunju et al. [32], in which no regular transfusion, The study had stated a prevalence of 8.4% for abnormal velocities (≥ 200 cm/s) and 21.9% for conditional velocities, this could suggest the important role of the transfusion regularity or combined with hydroxyurea treatment [1, 33, 34].
Patients with sickle cell anemia and conditional risk velocities must be closely monitored with frequent TCD scans to enable for early diagnosis of aberrant velocities and the implementation of primary stroke prevention strategies [35].
According to the frequency of blood transfusion, the right MCA (PSV), left DICA (PSV) & both DICA (TAmax) had a significant correlation with the frequency of blood transfusion, and this finding is in accordance with prior research. Abd-Allah et al. [36] which showed that the annual frequency of blood transfusion and HU dose was associated with a decreased frequency of abnormal TCD findings, but is opposite to Bowman et al.[37]; Gujjar et al. [38] that had reported that The differences in Doppler velocities noted were not significantly different between patients who had been transfused within 3 months of examination, and those who had not received transfusions.
According to frequency of blood transfusion the sensitivity and the specificity of the arterial velocities showed, The right MCA (PSV), the left DICA (PSV), and both DICA (TAmax) are the highest sensitive and specific velocities according to frequency of transfusion and this in accordance with Proust et al. [39] & Lagunju et al. [17] that had reported that sensitivity and specificity were higher than those for TCD for MCA (100% and 93%, respectively) and ICA (100% and 96.6%, respectively) in addition to Jones [40]; Naffaa [41] that showed PSV is at least as good as TAmax and can be used to select children with SCD for treatment or increased surveillance to prevent first stroke and the most frequent location of highest velocity measurement was noted to be in the middle cerebral artery regardless of whether it was measured by PSV or TAmax.
Among our patients, 65 patients had normal (not excised) spleen, while 4 patients underwent splenectomy (who were in low risk of stroke group). And there was insignificant difference between splenectomy status and Doppler velocities according to the risk of stroke, which is similar with the study done by Gutiérrez et al. [42]; Kanavaki et al. [43] had reported that there was no statistically significant difference in the TAmax values for all examined cerebral arteries between the non-splenectomized and splenectomized patient groups.
Regarding the hematological workup, the mean hemoglobin at our study was 8.23 ± 1.4 gm/dL and platelets was 333 ± 124.82 × 103. This is similar to that reported by Adekile et al. [20], where mean total hemoglobin was 8.5 ± 3.5 gm/dl among studied patients in Arabian Peninsula and platelets were on the upper limit with a value of 315.9 ± 140.6. Another study carried out in Nigeria deduced that the patients were anemic with platelets on the upper normal border. Chronic hemolysis, autosplenectomy, and chronic inflammation provide the unifying pathophysiological bases for the aforementioned hematological findings in SCD [44,45,46]. Several clinical studies have also linked severe anemia and thrombocytosis to adverse clinical events in SCD including acute chest syndrome, vaso-occlusive crisis, hospitalizations, silent cerebral infarcts, overt stroke, and death [47, 48].
In the current study, total bilirubin positively correlated with TCD velocities of all vessels apart from left PCA. This is similar finding to one study that correlated hemolytic markers with TCD velocities [19]. On the other hand, the same study concluded hemoglobin and hematocrit showed a negative correlation with TCD velocities, which is in line with our study. This can be explained by the compensatory mechanism of the cerebral perfusion under chronic anemia status [21]. Low baseline Hb were suggested to be associated with an increased risk of developing a conditional TCD or abnormal TCD later in childhood [49]. It is worth noting that direct bilirubin positively correlated with velocities in all vessels.
Our study revealed a positive correlation between age and TCD velocities. This is in line with a Sudanese study which detected the same correlation. Ismail et al. [21], but is opposite to that concluded by one Nigerian study Lagunju et al. [32] and another French study conducted by Bernaudi et al.[30], which showed a progressive decline in velocities after the age of 5 years. There is no clear explanation for this discrepancy.
Conclusions
The routine trans cranial duplex is indispensable in prediction of stroke in children with sickle cell disease who are at an increased risk of stroke, and the regularity of the blood transfusion is extremely important in the stroke prevention, in addition that the hydroxyurea combined with regular transfusion therapy might even be more beneficial. The most important velocities may act as indicators for the risk are TA max of both DICAs and PSV of RT MCA & LT DICA.
Availability of data and materials
The data supporting the conclusions of this article are available upon reasonable request from the authors.
Abbreviations
- CRT:
-
Chronic red cell transfusions
- EDV:
-
End diastolic velocity
- Hb:
-
Hemoglobin.
- HU:
-
Hydroxyurea
- PSV:
-
Peak systolic velocity.
- RI:
-
Resistive index
- SCD:
-
Sickle cell disease.
- SCIs:
-
Silent cerebral infarctions
- TA.max:
-
Time average mean of maximum velocity
- TCD:
-
Transcranial Doppler
- WBCs:
-
White blood cells count
References
Hirtz D, Kirkham FJ (2019) Sickle cell disease and stroke. Pediatr Neurol 95:34–41
Houwing ME, Grohssteiner RL, Dremmen MH et al (2020) Silent cerebral infarcts in patients with sickle cell disease: a systematic review and meta-analysis. BMC Med 18:1–7
Corvest V, Blais S, Dahmani B et al (2018) Cerebral vasculopathy in children with sickle cell disease: key issues and the latest data. Arch Pediatr 25:63–71
Mrad C, Pathak P, Abougergi MS et al. (2017) Cerebrovascular accidents among African American adults with sickle cell disease: a nationwide outcomes and trend analysis over two decades, pp 4644
Choudhury NA, DeBaun MR, Rodeghier M et al (2018) Silent cerebral infarct definitions and full-scale IQ loss in children with sickle cell anemia. Neurology 90:239–246
Obeagu EI (2018) An update on micro RNA in sickle cell disease. Int J Adv Res Biol Sci 5:157–158
O’Brien NF, Reuter-Rice K, Wainwright MS et al (2021) Practice recommendations for transcranial doppler ultrasonography in critically Ill children in the pediatric intensive care unit: a multidisciplinary expert consensus statement. J Pediatr Intensive Care 10:133–142. https://doi.org/10.1055/s-0040-1715128
Adams RJ, Nichols FT, Figueroa R et al (1992) Transcranial Doppler correlation with cerebral angiography in sickle cell disease. Stroke 23:1073–1077
Hoppe C, Neumayr L (2019) Sickle cell disease: monitoring, current treatment, and therapeutics under development. Hematol Oncol Clin 33:355–371
Ware RE, Davis BR, Schultz WH et al (2016) Hydroxycarbamide versus chronic trans-fusion for maintenance of transcranial doppler flow velocities in children with sickle cell anaemia-TCD With Transfusions Changing to Hydroxyurea (TWiTCH): a multicentre, open-label, phase 3, non-inferiority trial. Lancet 387:661–670
Fortin PM, Hopewell S, Estcourt LJ (2018) Red blood cell transfusion to treat or prevent complications in sickle cell disease: an overview of Cochrane reviews. Cochrane Database Syst Rev 2018(8):CD012082
Estcourt LJ, Fortin PM, Hopewell S et al (2017) Interventions for preventing silent cerebral infarcts in people with sickle cell disease. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD012389.pub2
Mazzucco S, Diomedi M, Qureshi A et al (2017) Transcranial Doppler screening for stroke risk in children with sickle cell disease: a systematic review. Int J Stroke 12:580–588
Cherry MG, Greenhalgh J, Osipenko L et al (2012) The clinical effectiveness and cost-effectiveness of primary stroke prevention in children with sickle cell disease: a systematic review and economic evaluation. Health Technol Assess Program. https://doi.org/10.3310/hta16430
Adewoyin AS (2015) Management of sickle cell disease: a review for physician education in Nigeria (Sub-Saharan Africa). Anemia 2015:791498
El-Beshlawy A, Youssry I (2009) Prevention of hemoglobinopathies in Egypt. Hemoglobin 33:S14-20
Lagunju I, Sodeinde O, Brown B et al. (2013) Transcranial Doppler ultrasonography in children with sickle cell anemia: clinical and laboratory correlates for elevated blood flow velocities. J Clin Ultrasound 1–7
Bernaudin F, Verlhac S, Arnaud C, Kamdem A et al (2015) Chronic and acute anemia and extracranial internal carotid stenosis are risk factors for silent cerebral infarcts in sickle cell anemia. Blood 125:1653–1661
Salama K, Rady R, Hashem RH et al (2020) Transcranial Doppler velocities among sickle cell disease patients in steady state. Hemoglobin 44:418–422
Adekile A, Hassan M, Asbeutah A et al (2019) Transcranial Doppler ultrasound in peninsular Arab patients with sickle cell disease. J Ultrasound Med 38:165–172
Ismail WIM, Elnour M, Mustafa AEM (2019) Evaluation of transcranial Doppler abnormalities in children with sickle cell disease in El-Obeid Specialized Children’s Hospital. J Family Med Prim Care 8:1176–1181
El-Shanshory M, Hablas N, Nagy H et al (2019) Asymmetric dimethylarginine levels and its correlation to cerebral blood flow in children with sickle cell Anemia. Indian J Hematol Blood Transfus 35:742–749. https://doi.org/10.1007/s12288-019-01109-6
Kwiatkowski JL, Zimmerman R, Greenbaum B et al (2004) Stroke and elevated blood flow velocity in the anterior cerebral artery in sickle cell disease. J Pediatr Hematol Oncol 26:323–326
Adams RJ, McKie VC, Brambilla D et al (1998) Stroke prevention trial in sickle cell anemia. Control Clin Trials 19:110–129
Greenwood S, Deane C, Rees OL, Freedman B, Kumar S et al (2017) The significance of inadequate transcranial Doppler studies in children with sickle cell disease. PLoS ONE 12:e0181681
Crosby LE, Joffe NE, Davis B et al (2016) Implementation of a process for initial transcranial Doppler ultrasonography in children with sickle cell anemia. Am J Prev Med 51:S10–S16
Jordan LC, Casella JF, DeBaun MR (2012) Prospects for primary stroke prevention in children with sickle cell anaemia. Br J Haematol 157:14–25
Bavarsad Shahripour R, Mortazavi MM, Barlinn K et al (2014) Can STOP trial velocity criteria be applied to Iranian children with sickle cell disease? J Stroke 16:97–101
Adams RJ (2005) TCD in sickle cell disease: an important and useful test. Pediatr Radiol 35:229–234
Bernaudin F, Verlhac S, Arnaud C et al (2011) Impact of early transcranial Doppler screening and intensive therapy on cerebral vasculopathy outcome in a newborn sickle cell anemia cohort. Blood 117:1130–1140
Makani J, Kirkham F, Komba A (2009) Risk factors for high cerebral blood flow velocity and death in Kenyan children with Sickle Cell Anaemia: the role of haemoglobin oxygen saturation and febrile illness. Br J Haematol 145:529–532
Lagunju I, Sodeinde O, Telfer P (2012) Prevalence of transcranial Doppler abnormalities in Nigerian children with sickle cell disease. Am J Hematol 87:544–547
Brousse V, Gandhi S, Montalembert M et al (2013) Combined blood transfusion and hydroxycarbamide in children with sickle cell anaemia. Br J Haematol 160:259–261
Kirkham FJ, Lagunju IA (2021) Epidemiology of stroke in sickle cell disease. J Clin Med 10:4232
Hokazono M, Silva GS, Silva EM et al (2011) Results form transcranial doppler examination on children and adolescents with sickle cell disease and correlation between time averaged maximal mean velocities and hematological characteristics: a cross-sectional study. Sao Paulo Med J 1129:34
Abd-Allah F, Eltagui M, Aboulfotooh AM et al (2020) Factors associated with abnormal cerebral blood flow in Egyptian children with sickle cell disease. Clin Transl Neurosci. https://doi.org/10.1177/2514183X20911351
Bowman LS, Ramsingh D, Vicari P et al (2006) Transcranial Doppler ultrasonography in adults with sickle cell disease. Neurology 67:572–574
Gujjar AR, Zacharia M, Al-Kindi S et al (2013) Transcranial Doppler ultrasonography in sickle cell disease: a study in Omani patients. J Pediatr Hematol Oncol 35:18–23
Proust F, Callonec F, Clavier E et al (1999) Usefulness of transcranial color-coded sonography in the diagnosis of cerebral vasospasm. Stroke 30:1091–1098
Jones A, Granger S, Brambilla D et al (2005) Can peak systolic velocities be used for prediction of stroke in sickle cell anemia? Pediatr Radiol 35:66–72
Naffaa LN, Tandon YK, Irani N (2015) Transcranial Doppler screening in sickle cell disease: the implications of using peak systolic criteria. World J Radiol 7:52–56
Gutiérrez DA, Svarch E, Arencibia NA, et al. (2014) Partial splenectomy in sickle cell disease. An Pediatr (Barc)
Kanavaki A, Kattamis A, Delaporta P et al (2015) Evaluation of intracranial cerebral blood flow velocities in splenectomised and non-splenectomised patients with β-thalassemia intermedia using transcranial doppler sonography. In Vivo 29:501–504
Rother R, Bell L, Hillmen P et al (2005) The clinical sequelae of intravascular haemolysis and extracellular plasma haemoglobin: a novel mechanism of human disease. JAMA 293:1653–1662
Okpala I (2006) Leukocyte adhesion and the pathophysiology of sickle cell disease. Curr Opin Hematol 13:40–44
Okpala I (2004) The intriguing contribution of white blood cells to sickle cell disease—a red cell disorder. Blood Rev 18:65–73
Omoti C (2005) Haematological values in sickle cell anaemia in steady-state and during vaso-occlusive crisis in Benin City Nigeria. Ann Afr Med 4:62–67
Meier E, Wright E, Miller J (2014) Reticulocytosis and anaemia are associated with an increased risk of death and stroke in the newborn cohort of the Cooperative Study of Sickle Cell Disease. Am J Hematol 89:904–906
Meier ER, Fasano RM, Estrada M et al (2016) Early reticulocytosis and anemia are associated with abnormal and conditional transcranial Doppler in children with sickle cell anemia. J Pediatr 169:227–231
Acknowledgements
We acknowledge this work to all the patients who were involved in the study.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
SM and MS have designed this study together. MS and MA contributed to the data collection. SM and MA contributed to data analysis. MS contributed to data processing. SM and SF shared together in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethical Research Committee of Faculty of Medicine Cairo University in Egypt. The ethics committee reference number is not available. A verbal consent was taken from the legal guardians of all patients accepting to participate in our research work.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within this study.
Competing interests
The authors declared that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kamel, S.M., Nassim, M.S., Mohamed, M.A. et al. Updating the role of transcranial Doppler in prediction and prevention of stroke in correlation to the regularity of blood transfusion in Egyptian children with sickle cell anemia. Egypt J Radiol Nucl Med 53, 256 (2022). https://doi.org/10.1186/s43055-022-00936-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00936-4