
Abstract
Background
Breast cancer is the leading cause of cancer-related mortality in women. Human epidermal growth factor receptor 2 (HER2) overexpression is seen in 20 out of 100 invasive breast cancers. Among HER2+ patients, two distinct hormone receptor (HR) subtypes can be defined: HR-positive (HR+) and HR-negative (HR−) each of which with unique therapeutic response and survival pattern. Contrast-enhanced spectral mammography (CESM) is an emerging novel imaging modality that offers diagnostic performance comparable to contrast-enhanced MRI. The purpose of this retrospective study was to describe the CESM features of HER2+ breast cancers according to hormone receptor status and to assess whether specific mammographic and CESM imaging features can differentiate between HER2+/HR+ and HER2+/HR− breast cancers potentially aiding treatment planning in HER2+ breast cancer patients.
Results
A total of 61 patients were included. Twenty-nine cases (47.5%) were HER2+/HR+ and 32 cases (52.5%) were HER2+/HR−. No statistically significant difference was found between mammographic imaging presentations and hormonal status. HR- were more likely to be multifocal (P 0.018), rounded or oval (P 0.008), circumscribed (P 0.004), and with associated non-mass enhancement (NME) (P < 0.001). HR+ cancers showed a tendency for irregular shape (P 0.008), spiculated outline (P 0.004), and heterogeneous (P 0.021) or ring (P 0.046) enhancement.
Conclusions
HER2+ tumors have different demographic, pathologic and imaging features according to the hormone receptor status. Because the two subtypes of HER2 breast cancer have different clinical outcomes, CESM imaging features can potentially enhance patient outcome by accelerating the diagnosis and treatment.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Breast cancer is the most common cancer and the leading cause of cancer-related death in women [1]. The prognosis of breast cancer is impacted by several factors including tumor grade, axillary lymph node status and molecular subtypes all of which are vital in treatment planning with molecular subtypes being the most crucial [2,3,4]. Human epidermal growth factor receptor 2 (HER2) overexpression is seen in one out of five invasive breast cancer cases, which is linked to a lower survival rate [5, 6]. Published clinical trial studies reported that HER2-positive (HER2+) are a diverse group of cancers [7, 8]. Among HER2+ patients, two distinct hormone receptor (HR) subtypes can be defined: HR-positive (HR+) and HR-negative (HR-) each of which with unique therapeutic response, recurrence rates, and survival pattern with HR-/HER2+ tumors more likely to cause death within the first five years of diagnosis, a higher tendency to metastasize to brain compared to bone, and a more favorable response to neoadjuvant chemotherapy [9,10,11].
Identification of the imaging features of different molecular types of breast cancer is crucial as it can potentially reflect its biological features [4]. Several studies have described the MRI and mammographic characteristics of HER2+ breast tumors. Fine pleomorphic and linear branching microcalcifications on mammograms while irregular tumor margins, tendency to multifocality and wash-out kinetics on MRI were characteristic of HER2+ tumors [12,13,14,15]. Contrast-enhanced spectral mammography (CESM) is a novel diagnostic imaging tool that utilizes iodinated contrast media using digital mammography to provide low-energy and subtraction images reflecting tumor vascularity, and displaying morphological and anatomical features of neoplastic breast lesions [16, 17]. According to previous reports, CESM offers diagnostic accuracy that is comparable to contrast-enhanced MRI (CE-MRI) [18, 19]. Wide availability, shorter examination time and lower cost are among other CESM advantages [20, 21].
While several studies reported the CE-MRI imaging features of molecular subtypes of breast cancer [22,23,24], studies on CESM focused mainly on differentiating benign from malignant breast cancers, or monitoring treatment response in patients receiving neoadjuvant chemotherapy [25,26,27,28,29]. We believe that CESM can provide morphological and anatomical information that are comparable to CE-MRI, which reflects breast cancer molecular subtypes. Therefore, the purpose of this retrospective study was to describe the CESM features of HER2+ breast cancers according to hormone receptor status and to assess whether specific imaging features can distinguish between HER2+/HR+ and HER2+/HR− breast cancers that can potentially be useful for treatment planning in patients with HER2+ breast cancer.
Methods
Our retrospective single-institution study included all consecutive female patients who had pathologic diagnosis of HER2+ invasive breast cancers. Data were collected from January 2017 to December 2021. The study was approved by our institution Ethics Committee before data collection. A waiver of informed consent was granted due to retrospective study design. The data were collected using our hospital electronic medical records. Images were retrieved from our Radiology Department Picture Archiving and Communication System (PACS). Inclusion criteria included female patient with age more than 18 years, HER2+ breast cancer diagnosis based on core needle biopsy and immunohistochemistry and completion of standard mammogram with CESM examination. Exclusion criteria include contrast media reaction, renal impairment, pregnancy as well as neoadjuvant chemotherapy administration, biopsy, or surgery prior to CESM examination.
CESM examination
All mammographic examinations were performed at the institution’s Radiology Department using GE Healthcare machine (Chalfont St. Giles, UK) allowing dual-energy CESM acquisitions with some specific hardware and software enhancements for image processing and acquisition.
Unlike conventional mammography, the X-ray spectrum was tailored to produce energies just above the K-edge of iodine (33.2 keV) to increase the sensitivity to low concentration of iodine to optimize the visualization of iodine. Typically, for a 50% glandular and 5-cm-thick breast, exposure times were around 1 s and 3 s for low -and high-energy images, respectively.
Standard mammography was done followed by an intravenous administration of 1.5 ml/kg body weighted of a non-ionic contrast material (Omnipaque) manually at one shot. Two sets of low- and high-energy exposures were taken: one 2 min after the contrast medium administration with the breast compressed in a mediolateral oblique (MLO) view and the second 4 min after the contrast medium administration with the breast compressed in the craniocaudal (CC) view. Specific image processing for both exposures was then done with the final subtraction images (one in the MLO and one in the CC view) highlighting the mass and removing the noise created by the fibroglandular tissue. The compression applied after the injection minimized the motion blur keeping the image details seen with the standard mammography. The average examination time was 10 min. After the examination, the patients were monitored for around 30 min for any potential contrast medium adverse reactions.
Image interpretation
One of the participating radiologists interpreted standard mammography and CESM studies in accordance with the Breast Imaging Reporting and Data System (BI-RADS) lexicon designed by the American College of Radiology [30]. In case of disagreement, the case was discussed, and a joint consensus was reached. In patients with multiple masses, the largest lesion was considered for assessment. All radiologists were blinded to the hormonal status of the lesions. On mammograms, imaging presentation was described as mass, architectural changes, or asymmetry and the presence or absence of calcifications was recorded. A mass lesion was defined when a lesion larger than 5 mm in three dimensions was visible in both mammographic views. On CESM examination, the disease was recorded as unifocal or multifocal. The size, shape and margin of the lesion were recorded, and the pattern of enhancement was documented as homogeneous, heterogeneous, ring or non-mass enhancement (NME), which is defined as an area of enhancement not confined to a mass or a three-dimensional volume effect. Table 1 summarizes mammographic and CESM imaging criteria assessed in our study.
Histopathological assessment
Following surgery or image-guided core biopsy, all specimens were sent to our institution laboratory for histopathological confirmation. Specimens underwent immunohistochemistry to detect the levels of ER, PR and HER2 overexpression. Imaging findings were available during histopathologic assessment. HER2 expression on IHC was categorized according to the cell membrane staining pattern with grades 2+ and 3+ regarded as positive, whereas grades 1+ and 0 considered negative. Fluorescence in situ hybridization (FISH) was used to further analyze all the equivocal samples. In all cases, a FISH ratio larger than 2.2 or a HER2 gene copy greater than 6.0 was considered positive. Stained slides were examined by pathologists for nuclear ER or PR expression using the College of American Pathologists guidelines (≥ 1% cutoff value for positive) [31].
Statistical methods
Data were statistically described in terms of mean ± standard deviation (±SD), median and range, or frequencies (number of cases) and percentages when appropriate. Comparison of numerical variables between the study groups was done using Student t test for independent samples. For comparing categorical data, Chi-square (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5. Accuracy of different findings in differentiating HR+ from HR− cases was represented using the terms sensitivity, specificity, +ve predictive value, −ve predictive value and overall accuracy. Two-sided p values less than 0.05 were considered statistically significant. IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 22 for Microsoft Windows was used for all statistical analyses. For accuracy calculations, the following formulas were used:
-
Sensitivity = T(+)ve ÷ [T(+)ve + F(−)ve].
-
Specificity = T(−)ve ÷ [T(−)ve + F(+)ve].
-
Positive predictive value = T(+)ve ÷ [T(+)ve + F(+)ve].
-
Negative predictive value = T(−)ve ÷ [T(−)ve + F(−)ve].
-
Overall accuracy = [T(+)ve + T(−)ve] ÷ all sample.
Results
Following exclusion criteria, 61 patients were included in our study. Twenty-nine cases (47.5%) were HER2+/HR+, and 32 cases (52.5%) were HER2+/HR−. Their ages ranged from 29 to 84 years with a mean of 52.34 ± 11.5 years. Twenty-six patients (42.6%) were < 50 years, while 35 patients (57.4%) were ≥ 50 years. HER2+/HR−. Cases were significantly associated with older age compared to HER2+/HR+ (P value 0.003) with 24 out of 35 (68.6%) patients ≥ 50 years seen in HR- group. Invasive duct carcinoma (IDC) was the most common histopathological type in our series seen in 58 cases (91.1%). Invasive lobular carcinoma (ILC) was seen in two cases (3.3%) and clear cell carcinoma in one case (1.6%). Twenty-eight out of 61 cases (45.9%) were histological grade III, 26 cases (42.6%) were grade II and seven cases (11.5%) were grade I. Compared to HER2+/HR+, HER2+/HR− tumors were strongly associated with higher histologic grade (P value < 0.001) with 22 out of 28 (78.6%) of high histological grade III tumors seen in HR− group in contrast to 23 out of 33 lesions (69.7%) of histological grade I and II in the HR+ group. Table 2 summarizes the demographic, pathologic and imaging features of HER+ tumors according to hormone receptor status.
On mammography, 40 out of 61 (65.6%) cases in our series were categorized as mass evenly distributed between the HR− and HR+ groups, 10 cases (16.4%) as architectural changes and 11 cases (18.0%) as asymmetry. We did not find statistically significant difference between mammographic imaging presentations and the HER2+/HR+ and HER2+/HR− groups with P values of 0.788, 0.170 and 0.307 for mass, architectural changes and asymmetry, respectively. Twenty-one out of our 61 HER2+ cases (34.4%) exhibited calcifications on mammography: 11 cases (52.4%) in the HR+ and 10 cases (47.6%) in the HR− group. There was no statistically significant difference between the HR+ and HR− groups regarding the presence or distribution of calcifications with a P value of 0.602.
On CESM, the mean tumor size was 5.4 ± 2.3 cm and 5.9 ± 2.7 cm for HR− and HR+ groups, respectively. We did not find statistically significant difference in tumor size between the two groups with a P value of 0.541. Multifocal tumors were reported in 25 out 61 cases (41.0%). We found that HR− tumors were more likely to be multifocal compared to HR+ group with 18 out of 25 cases (72.0%) of multifocal tumors in our series seen in HR− group (P value 0.018) (Fig. 1). HR-tumors were more likely to be rounded or oval (P value 0.008) compared to HR+ lesions with 18 out of 24 (75%) rounded or oval tumors seen in the HR− group. Additionally, HR-lesions were more likely to have circumscribed margins (P value 0.004) and with associated NME (P value < 0.001) on CESM compared to HR+ group (Fig. 2). Lesions in the HR+ group, on the other hand, had a higher tendency for irregular shape (P value 0.008), spiculated outline (P value v0.004) and heterogeneous (P value 0.021) or ring enhancement (P value 0.046) (Figs. 3 and 4). Table 3 demonstrates CESM imaging features associated with HR negativity within HER2+ tumors.

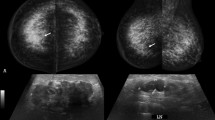
75-year-old female patient with a pathologically proven left breast IDC (HER2+/HR−) a and b Full-field digital mammography in CC and MLO views. c and d CESM in CC and MLO views showing a partially defined roughly oval-shaped mass lesion with spiculated outline at the retro-aerolar region of the left breast eliciting intense heterogeneous enhancement with smaller mass lesions at the deep retro-aerolar region indicating a multifocal neoplasm

64-year-old female patient with a pathologically proven right breast IDC (HER2+/HR−) a and b full-field digital mammography in CC and MLO views showing a large partially circumscribed dense lesion with an adjacent smaller nodule and overlying suspicious amorphous clustered microcalcifications. c and d CESM in CC and MLO views showing an intense heterogeneous enhancement of the large mass lesion at the upper outer quadrant of the right breast associated with non-mass enhancement with segmental distribution

68-year-old female patient with a pathologically proven left breast IDC (HER2+/HR+) a full-field digital mammography in CC view and b CESM in CC view showing left breast outer quadrant irregular shaped hyperdense mass lesion with spiculated outline eliciting intense heterogeneous enhancement

52-year-old female patient with a pathologically proven right breast IDC (HER2+/HR+: a full-field digital mammography in CC view and b CESM in CC view showing an irregular shaped hyperdense mass lesion with spiculated outline at the retro-areolar region eliciting intense heterogeneous ring enhancement
Assessment of the sensitivity and accuracy of mammographic and CESM imaging features revealed that the accuracy and sensitivity of NME in differentiating between HR- and HR+HER2+ neoplasms was high at 70.5% and 96.6% respectively. The imaging features with the highest sensitivity for HR+ tumors were irregular mass shape and spiculated margins, with a value of 79.3%. The accuracy of the mammographic imaging features was low at 52.5%, 59.0%, 45.9% and 54.1% for mass, architectural changes, asymmetry, and calcifications respectively.
Discussion
HER2 overexpression accounts for 20 out of 100 breast cancer cases, and it is associated with lower survival rates [5, 6]. In the last two decades, since the molecular subtyping has become the standard of care in breast cancer management, the role of imaging has been to attempt to find specific imaging features that correlate to certain molecular subtypes with the intention to improve patient survival through prompt diagnosis and treatment [4]. CESM is well tolerated by patients, and its use in clinical practice has increased in the last few years [32]. Published studies have concluded that MRI and CESM have similar accuracy for breast cancer detection [33]. In this study, we demonstrated that HER2+ tumors have different demographic, pathologic and imaging features according to hormonal status, and these features were more evident on CESM compared to mammography.
In the current study, HER2+/HR− tumors were significantly associated with older age and higher histological grade compared to HR+ group with P values of 0.003 and < 0.001, respectively, similar to previous investigators [34, 35]. We also reported no statistically significant difference in tumor size between the HR− and HR+ groups as found in our study similar to the study by Song et al. [34].
In this study, the mammographic imaging features were not statistically significant in differentiating between HER2+/HR− and HER2+/HR+ groups similar to previous investigators who did not find significant difference in mammographic imaging presentations as well as the distribution and morphology of calcifications between the HR- and HR group in their series [34].
In the current study, we categorized the pattern of enhancement elicited by CESM into homogeneous, heterogenous, ring and NME based on MRI-BIRADS lexicon morphological characteristics [36]. Heterogeneous pattern of enhancement was the most common enhancement pattern encountered in our series seen in 49.2% of cases. Our findings were consistent with previous investigators who reported that masses eliciting heterogeneous enhancement showed a significantly higher tendency of malignancy compared to masses with homogeneous enhancement [26, 37, 38]. NME was the second most common pattern observed in our series in line with the Kamal et al. [26] and Wilhelm et al. [39], who reported strong correlation between NME and malignant pathology with P values of ≤ 0.001. On CESM, we found that round or oval shape, circumscribed margins and associated NME were strongly associated with HER2+/HR− tumors similarly reported by previous investigators who based their conclusions on mammography and MRI findings [14, 34, 35].
We found that tumors with irregular shape, spiculated outline and heterogeneous or ring enhancement were more consistent with HER2+/HR+ tumors in line with previous investigators who also concluded that HER2+/HR+ tumors were more likely to resemble luminal A (LA) tumors [40, 41]. Our study was contrasted by previous investigators who did not find significant correlation between ring enhancement on CESM and malignant pathology in their series of 109 malignant lesions and came to a conclusion that reviewing T2 MRI images is very reliable in ruling out infected cysts and abscess cavities—an advantage that CESM lacks [26].
The current study had some limitations. Selection bias may have been present due to retrospective study design. The study was carried out at a single institution with a small sample size for HR− and HR+ groups. More multi-institution studies with larger sample sizes are needed in the future to further document and confirm our findings. Additionally, we excluded patients who had neoadjuvant chemotherapy before the CESM examination; therefore, our findings might not be applicable to locally advanced breast cancer. The study did not investigate the interobserver variability in image interpretation. We observed that despite the participation of expert radiologists who were blinded to the IHC status, the evaluation of mass shapes and margins was subjective. The use of automated computer-aided detection (CAD) techniques may be helpful in the future in obtaining reproducible results potentially aiding breast cancer molecular subtype characterization.
Conclusions
CESM is a well-tolerated widely available novel diagnostic tool that offers accuracy comparable to CE-MRI. HER2+ tumors have different demographic, pathologic and imaging features according to the hormone receptor status. On CESM, HER2+/HR− tumors were more likely to be multifocal, rounded or oval with circumscribed margins and associated with NME, while HER2+/HR+ cancers were more likely to be irregular in shape, and spiculated in margin, and elicit heterogeneous or ring enhancement. Mammographic imaging features were not helpful in differentiating HR− and HR+ cancers. Because the two subtypes of HER2 breast cancer have different clinical outcomes, CESM imaging features can potentially enhance patient outcome by accelerating the diagnosis and treatment. More prospective multicenter studies with larger sample sizes and interobserver variability are needed in the future to further validate and document our findings.
Availability of data and materials
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BIRADS:
-
Breast imaging reporting and data system
- CC:
-
Craniocaudal
- CE-MRI:
-
Contrast-enhanced MRI
- CESM:
-
Contrast-enhanced spectral mammography
- FISH:
-
Fluorescence in situ hybridization
- IDC:
-
Invasive duct carcinoma
- ILC:
-
Invasive lobular carcinoma
- HER2:
-
Human epidermal growth factor receptor 2
- HER2+:
-
Human epidermal growth factor receptor 2 positive
- HR:
-
Hormone receptor
- HR+:
-
Hormone receptor positive
- HR−:
-
Hormone receptor negative
- LA:
-
Luminal A
- MLO:
-
Mediolateral oblique
- NME:
-
Non-mass enhancement
- PACS:
-
Picture Archiving and Communication System
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394–424
Li H, Zhu Y, Burnside ES, Huang E, Drukker K, Hoadley KA, Fan C et al (2016) Quantitative MRI radiomics in the prediction of molecular classifications of breast cancer subtypes in the TCGA/TCIA data set. NPJ Breast Cancer 2:16012. https://doi.org/10.1038/npjbcancer.2016.12
Bedard PL, Hansen AR, Ratain MJ, Siu LL (2013) Tumour heterogeneity in the clinic. Nature 501:355–364
Wang S, Wang Z, Li R, You C, Mao N, Jiang T et al (2022) Association between quantitative and qualitative image features of contrast-enhanced mammography and molecular subtypes of breast cancer. Quant Imaging Med Surg 12:1270–1280
Chia S, Norris B, Speers C, Cheang M, Gilks B, Gown AM et al (2008) Human epidermal growth factor receptor 2 overexpression as a prognostic factor in a large tissue microarray series of node-negative breast cancers. J Clin Oncol 26:5697–5704
Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL (1987) Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 235:177–182
Prat A, Carey LA, Adamo B, Vidal M, Tabernero J, Cortés J et al (2014) Molecular features and survival outcomes of the intrinsic subtypes within HER2-positive breast cancer. J Natl Cancer Inst 106:dju152. https://doi.org/10.1093/jnci/dju152
Arteaga CL, Sliwkowski MX, Osborne CK, Perez EA, Puglisi F, Gianni L (2011) Treatment of HER2-positive breast cancer: current status and future perspectives. Nat Rev Clin Oncol 9:16–32
Lee HJ, Park IA, Park SY, Seo AN, Lim B, Chai Y et al (2014) Two histopathologically different diseases: hormone receptor-positive and hormone receptor-negative tumors in HER2-positive breast cancer. Breast Cancer Res Treat 145:615–623
Vaz-Luis I, Winer EP, Lin NU (2013) Human epidermal growth factor receptor-2-positive breast cancer: does estrogen receptor status define two distinct subtypes? Ann Oncol 24:283–291
Vaz-Luis I, Ottesen RA, Hughes ME, Marcom PK, Moy B, Rugo HS et al (2012) Impact of hormone receptor status on patterns of recurrence and clinical outcomes among patients with human epidermal growth factor-2-positive breast cancer in the national comprehensive cancer network: a prospective cohort study. Breast Cancer Res 14:R129. https://doi.org/10.1186/bcr3324
Elias SG, Adams A, Wisner DJ, Esserman LJ, van’t Veer LJ, Mali WP et al (2014) Imaging features of HER2 overexpression in breast cancer: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev 23:1464–1483
Agrawal G, Chen JH, Baek HM, Hsiang D, Mehta RS, Nalcioglu O et al (2007) MRI features of breast cancer: a correlation study with HER-2 receptor. Ann Oncol 18:1903–1904
Seo BK, Pisano ED, Kuzimak CM, Koomen M, Pavic D, Lee Y et al (2006) Correlation of HER-2/neu overexpression with mammography and age distribution in primary breast carcinomas. Acad Radiol 13:1211–1218
Wang Y, Ikeda DM, Narasimhan B, Longacre TA, Bleicher RJ, Pal S et al (2008) Estrogen Receptor-Negative invasive breast cancer: imaging features of tumors with and without human epidermal growth factor receptor type 2 overexpression. Radiology 246:367–375
Jochelson MS, Lobbes MBI (2021) Contrast-enhanced mammography: state of the art. Radiology 299:36–48
Lalji UC, Jeukens CR, Houben I, Nelemans PJ, van Engen RE, van Wylick E et al (2015) Evaluation of low-energy contrast-enhanced spectral mammography images by comparing them to full-field digital mammography using EUREF image quality criteria. Eur Radiol 25:2813–2820
Lewin J (2018) Comparison of contrast-enhanced mammography and contrast-enhanced breast MR imaging. Magn Reason Imaging Clin N Am 26:259–263
Li L, Roth R, Germaine P, Ren S, Lee M, Hunter K et al (2017) Contrast-enhanced spectral mammography (CESM) versus breast magnetic resonance imaging (MRI): a retrospective comparison in 66 breast lesions. Diagn Interv Imaging 98:113–123
Fallenberg EM, Schmitzberger FF, Amer H, Ingold-Heppner B, Balleyguier C, Diekmann F et al (2017) Contrast-enhanced spectral mammography vs. mammography and MRI—clinical performance in a multi-reader evaluation. Eur Radiol 27:2752–2764
Xing D, Lv Y, Sun B, Xie H, Dong J, Hao C et al (2019) Diagnostic value of contrast-enhanced spectral mammography in comparison to magnetic resonance imaging in breast lesions. J Comput Assist Tomogr 43:245–251
Kim JY, Kim SH, Kim YJ, Kang BJ, An YY, Lee AW et al (2014) Enhancement parameters on dynamic contrast enhanced breast MRI: do they correlate with prognostic factors and subtypes of breast cancers? Magn Reson Imaging 33:72–80
Yamaguchi K, Abe H, Newstead GM, Egashira R, Nakazono T, Imaizumi T et al (2014) Intratumoral heterogeneity of the distribution of kinetic parameters in breast cancer: comparison based on the molecular subtypes of invasive breast cancer. Breast Cancer 22:496–502
Blaschke E, Abe H (2015) MRI phenotype of breast cancer: kinetic assessment for molecular subtypes. J Magn Reson imaging 42:920–924
Barra FR, Sobrinho AB, Barra RR, Magalhães MT, Aguiar LR, de Albuquerque GFL et al (2018) Contrast-enhanced mammography (CEM) for detecting residual disease after neoadjuvant chemotherapy: a comparison with breast magnetic resonance imaging (MRI). Biomed Res Int 2018:1–9
Mohamed Kamal R, Hussien Helal M, Wessam R, Mahmoud Mansour S, Godda I, Alieldin N (2015) Contrast-enhanced spectral mammography: impact of the qualitative morphology descriptors on the diagnosis of breast lesions. Eur J Radiol 84:1049–1055
Lv Y, Chi X, Sun B, Lin S, Xing D (2020) Diagnostic value of quantitative gray-scale analysis of contrast-enhanced spectral mammography for benign and malignant breast lesions. J Comput Assist Tomogr 44:405–412
Rudnicki W, Heinze S, Popiela T, Kojs Z, Luczynska E (2020) Quantitative assessment of contrast enhancement on contrast enhancement spectral mammography (CESM) and comparison with qualitative assessment. Anticancer Res 40:2925–2932
Rudnicki W, Heinze S, Niemiec J, Kojs Z, Sas-Korczynska B, Hendrick E et al (2019) Correlation between quantitative assessment of contrast enhancement in contrast-enhanced spectral mammography (CESM) and histopathology-preliminary results. Eur Radiol 29:6220–6226
Sickles EA, D’Orsi CJ, Bassett LW (2013) ACR BI-RADS mammography. In: ACR BI-RADS Atlas, breast imaging reporting and data system, 5th Edition, American College of Radiology, Reston
Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thürlimann B, Senn HJ, Panel members (2011) Strategies for subtypes-dealing with the diversity of breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol 22:1736–1747
Savaridas SL, Tennant SL (2022) Quantifying lesion enhancement on contrast-enhanced mammography: a review of published data. Clin Radiol 77:e313–e320
Łuczyńska E, Heinze-Paluchowska S, Hendrick E, Dyczek S, Ryś J, Herman K et al (2015) Comparison between breast MRI and contrast-enhanced spectral mammography. Med Sci Monit 21:1358–1367
Song SE, Bae MS, Chang JM, Cho N, Ryu HS, Moon WK (2017) MR and mammographic imaging features of HER2-positive breast cancers according to hormone receptor status: a retrospective comparative study. Acta Radiol 58:792–799
Putti TC, El-Rehim DM, Rakha EA, Paish CE, Lee AH, Pinder SE et al (2005) Estrogen receptor-negative breast carcinomas: a review of morphology and immunophenotypical analysis. Mod Pathol 18:26–35
Spak DA, Plaxco JS, Santiago L, Dryden MJ, Dogan BE (2017) BI-RADS® fifth edition: a summary of changes. Diagn Interv Imaging 98:179–190
Chi X, Zhang L, Xing D, Gong P, Chen Q, Lv Y (2020) Diagnostic value of the enhancement intensity and enhancement pattern of CESM to benign and malignant breast lesions. Medicine (Baltim) 99:e22097. https://doi.org/10.1097/MD.0000000000022097
Travieso-Aja MM, Maldonado-Saluzzi D, Naranjo-Santana P, Fernández-Ruiz C, Severino-Rondón W, Rodríguez Rodríguez M et al (2019) Evaluation of the applicability of BI-RADS® MRI for the interpretation of contrast-enhanced digital mammography. Radiologia 61:477–488
Wilhelm A, McDonough MD, DePeri ER (2012) Malignancy rates of non-masslike enhancement on breast magnetic resonance imaging using American College of Radiology Breast Imaging Reporting and Data System descriptors. Breast J 18:523–526
Kawashima H, Inokuchi M, Furukawa H, Ikeda H, Kitamura S (2014) Magnetic resonance imaging features of breast cancer according to intrinsic subtypes: correlations with neoadjuvant chemotherapy effects. Springerplus 3:240. https://doi.org/10.1186/2193-1801-3-240
Costantini M, Belli P, Distefano D, Bufi E, Matteo MD, Rinaldi P et al (2012) Magnetic resonance imaging features in triple-negative breast cancer: comparison with luminal and HER2-overexpressing tumors. Clin Breast Cancer 12:331–339
Acknowledgements
The authors would like to acknowledge Dr. Magdy Ibrahim for providing the statistical advice for this manuscript and mammography radiographers at National Cancer Institute.
Funding
The authors declare that they have did not receive funding for this research.
Author information
Authors and Affiliations
Contributions
HE, SME, MHH, HSWM, AF and RK did data collection and analysis, and reporting CESM examinations, reviewing, and editing the manuscript. SME, MHH, HE and RK done review of literature, data collection and analysis, writing the original draft, reviewing, and editing the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
National Cancer Institute Ethics Committee approval was obtained. Reference number is not applicable. A waiver of informed consent was granted due to retrospective study design.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elkassas, H., Helal, M.H., Mikhael, H.S.W. et al. Mammographic and contrast-enhanced spectral mammography imaging findings of HER2-positive cancers according to hormone receptor status. Egypt J Radiol Nucl Med 53, 250 (2022). https://doi.org/10.1186/s43055-022-00933-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00933-7