
Abstract
Background
SPECT/CT imaging can provide information on axillary nodal morphology, number, and status of axillary levels, along with information on primary tumor morphology, mediastinum, and lungs that assesses nodal status beyond localization. The current study aims to evaluate the feasibility of SLNB with SPECT/CT for reporting nodal information in terms of morphology, number, and axillary levels that assess nodal staging. Ninety consecutive patients with early breast cancer were included. Thirty-seven MBq (1 mCi) of Tc99m nanocolloid was used. SPECT/CT followed PS. Nodal morphology, number, and axillary levels of sentinel and non-SLNs were reported along with their localization through a gamma probe.
Results
The mean population age was 54.5 ± 3 years. PS visualized 152 SLNs in 79 patients (success rate of 88%), and SPECT/CT showed 178 SLNs in 84 patients (93% success rate). SPECT/CT showed 90% of SLNs localized at axillary levels I & II, with 10% at the rest of the nodal areas. Out of total surgically excised, 103/706 nodes were tumor positive, and 603/706 nodes were histopathologically tumor-free. Out of 178 hot nodules, 40 showed morphologically abnormal nodes, including a few with more than one abnormal feature. The average scores in the characterization of nodal morphology for the two observers were 2.4 ± 0.71 and 2.53 ± 0.52, respectively, with a substantial agreement (k = 0.76).
Conclusions
Hybrid imaging with SPECT/CT defines axillary lymph nodes' level and morphological features. This additional information directs the surgeon to nodes not seen by planar imaging during SLNB and can help redefine the clinical axillary lymph node staging.
Similar content being viewed by others


Significance of the study
-
The significance of this study was to evaluate the clinical usefulness, suitability, and comparison of planar imaging and SPECT/CT in SLNB in breast cancer patients. In addition, evaluating the values of SPECT/CT in providing additional information for the clinical TNM staging.
Background
The two major prognostic indicators for breast cancer are the presence of axillary lymph node metastases and the clinical size of the primary tumor. The status of axillary nodal metastases shall then, in turn, decide for axillary lymph node dissection (ALND), which is the definitive method of determining axillary nodal metastases. However, ALND, which has high morbidity, has been supplanted by sentinel lymph node biopsy (SLNB), which has meager false-negative rates [1,2,3,4].
Ultrasonography (US) is the primary imaging modality in the preoperative setting for evaluating axillary nodes that can show morphologic details, such as cortical thickening, hilar effacement, and nonhilar cortical blood flow that is crucial information to be added to the size criteria in the identification of metastases and aids in tissue sampling. However, precise localization of higher-level axillary, intramammary, or in transit, and internal mammary nodes pose a limitation in sonographic evaluation, not to mention its high operator dependency.
Magnetic resonance imaging is also helpful, with the added benefit of providing a global view of both axillae; however, due to the phase-encoding direction being set in the left to right direction in most breast magnetic resonance imaging (MRI) protocols, the axillae are occasionally obscured by pulsation artifact from the heart. This problem is worse at axillary levels II and III.
For two decades, despite introducing hybrid single-photon emission tomography/computed tomography (SPECT/CT) gamma cameras and sentinel lymph node biopsy (SLNB), sentinel lymph node (SLN) imaging is potentially underutilized and has not been explored beyond the localization of SLN followed by biopsy [2, 5, 6].
The results consistently show that the SLN can be identified in 80% to 100% of patients undergoing SLNB for breast cancer [7, 8]. Furthermore, the false-negative rate in SLNB is low, with rates varying from 1 to 10% [9,10,11,12,13].
Radionuclide lymphoscintigraphy (RNL) in SLNB using hybrid SPECT/CT offers enhanced 3-D imaging and gives a global view of the axillae, breasts, mediastinum, and lungs. Beyond the philosophy of just localization of SLN for preoperative assessment, RNL SPECT/CT with high high-resolution CT component offer characterization of nodal morphology like size, shape, loss of fatty hila, cortical bulge, cortical effacement, gross nodal replacement with tumor, extranodal spread, speculation, pleomorphic microcalcifications, extracapsular extension, matted nodes, extranodal involvement, along with insights into the sonographically non-accessible technically challenging areas for precise localization of higher-level axillary, intramammary or in transit, and internal mammary nodes [14,15,16]. Along with US, RNL in SLNB imaging is routinely used for localization of SLN. However, with the widespread availability of RNL with hybrid SPECT/CT integration, clinical axillary staging using additional CT information has become an interesting aspect for staging the axilla beyond just localization of the SLN through planar scintigraphy (PS). The pathologic features of nodal metastases highlight these nodes' appearances are depicted on the CT part in RNL SPECT/CT, which gives a global view of both axillae during SLNB when the arms are in the abducted and externally rotated ("ABER") position.
The present study primarily aims to evaluate the clinical usefulness, suitability, and comparison of PS and SPECT/CT in SLNB, along with the evaluation of potential values of SPECT/CT in providing additional information for the clinical TNM staging (cTNM) by identification of number and levels of SLNs and characterization of nodal morphology.
Methods
Patients
The study included all patients (n=90) from January 2017 to March 2022 referred for SLNB. All patients included had early-stage breast cancer T1 (Tumor <2 cm), T2 (Tumor < 2-5cm), ductal carcinoma in situ, Paget's disease, and those cases who did not receive chemoradiation, and patients without any surgery. Patients with clinical evidence of axillary metastases, previous axillary lymphadenectomy, breast augmentation, palpable axillary nodes, treatment with chemotherapy or radiotherapy before breast surgery, and pregnant or lactating women were excluded. The hospital ethical committee formally approved the study, and routine informed consent was obtained for all patients after the procedure was explained to them.
Radionuclide lymphoscintigraphy (RNL)
SLN mapping was coordinated with the surgical department and was performed before surgery (within 2–4 h). Thirty-seven MBq (1 mCi) of Tc99m nanocolloid was divided into four aliquots of 0.3–0.5 mL tuberculin syringes and intradermally injected within the periareolar region in all four quadrants. Initial localization was done using a gamma probe, followed by imaging using a dual-head gamma camera with a low-energy, high-resolution, parallel-hole collimator. Static anterior, anterior oblique, and lateral images of 3 min were acquired after 15–30 min post-injection. The patient's ipsilateral arm was raised above the head. If no nodes were seen on the planar images, further delayed planer images were obtained 45–60-min post radiotracer injection. Transmission images using a Cobalt-57 (Co-57) flood source were used to outline the body contour on the planer imaging.
SPECT/CT acquisition
SPECT/CT images were acquired immediately after the planar study. SPECT/CT was performed using the SIEMENS Symbia T16 gamma camera with a system comprising of a dual-head gamma camera with a low-dose X-ray tube, low-energy high-resolution (LEHR) collimators, 16-slice CT scanner optimized for rapid rotation. SPECT acquisition (matrix 128 × 128, 60 frames at 25 s. per view) was performed using steps of 6 degrees. For CT (120 kV, 20 mA, and Beta 60 s kernel), 1-mm slices were created. SPECT and CT axial 1-mm slices were reconstructed using the ordered subset expectation maximization (OSEM) algorithm. The SPECT data were corrected for attenuation and scatter and then fused with the CT data to generate 3-D volumetric rendered imaging for better localization.
Interpretation of the studies
Two experienced nuclear medicine physicians performed the interpretation of RNL data independent of each other. Planar images with the Co57 flood source and SPECT/CT images were interpreted separately and in a masked fashion. The data for planar assessment included the number of hot nodes detected and whether they were axillary or internal mammary nodes. The locations of the hot nodes on the fused SPECT/CT images were categorized using the surgical levels of axillary lymph nodes. All visualized lymph nodes seen on the scintigraphy were called SLN. Disagreement was resolved by consensus.
The characterization of nodal morphology for possible metastases was based on radiological parameters (Table 1). The normal axillary lymph node is oval and has a smooth, well-defined margin. The cortex should be slightly hypodense and uniformly thin, measuring 3 mm or less. Nodes that meet this description have a high negative predictive value for excluding metastases.
Lymph node biopsy and histopathology
In the operation theater, the patient was prepared. General anesthesia starts with endotracheal intubation. The surgical site is prepared and draped in a standard surgical way. A gamma-ray detecting probe (GDP) GAMMA FINDER®, from World of Medicine, Germany, with a screen count display and an audible guidance system, was used to confirm the location of the SLN. The skin was incised close to the anterior axillary skin line for about 2 cm. Dissection is carried out in layers posteriorly toward the axillary depth of tissue; while using the GDP to guide dissection, the node emitting the highest activity was excised. Sometimes more than one node was picked up by the probe, in which case, the hottest node and the nodes with more than 10% of the ex vivo counts per minute of the hottest node were removed. Comparison is made of the counts with the GDP in situ before excision and directly in vitro after excision. The nodes with the highest radioactivity were labeled as the SLN and serially numbered. Permanent sections of all removed nodes were prepared for pathological examination. Then, the wound is closed in a simple fashion.
All nodes removed from the axilla (separately tagged SLN or non-SLN) were examined using a standard technique. Briefly, the nodes were freed from fat tissue, and those that were > 0.5 cm in diameter were bisected longitudinally, whereas nodes < 0.5 cm in greatest diameter were embedded whole. Three different sections were obtained (0.3–1.0 mm apart) and stained with hematoxylin and eosin. In addition, all SLNs underwent frozen sectioning, hematoxylin and eosin staining for gross metastases, and immunobiological (cytokeratin) staining to detect micrometastases. Positive cases eventually underwent axillary clearance as per guidelines.
Statistical analysis
Chi-square test was applied to evaluate the significance of difference between the two modalities, and the P value was accepted to be less than 0.05 as significant. The observers' scores were analyzed, the p value was calculated with the continuity Chi-square test, and the agreement was tested using Cohen's Kappa coefficient. The possible range of weighted kappa values is from − 1 (complete disagreement) to + 1 (perfect agreement) and is corrected to eliminate the agreement expected by chance alone. Kappa was classified as follows: 0, chance agreement; < 0.20, poor agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; 0.81–1.00, very good agreement.
Ninety patients with breast cancer (mean age, 54.5 years; median age 52 years; age range, 28–85 years) were included, as shown in Table 2, along with the measurement of the primary tumor size and the histology of axillary nodes reported in Table 3. Out of 178 hot SLNs on SPECT/CT, 90% were localized at axillary levels I & II, with 10% seen in the rest of the nodal areas (Table 4).
Results
Imaging findings on PS and SPECT/CT
PS visualized 152 SLNs in 79 patients (1.92 SLNs) with a success rate of 88% (median 2, range 1–6). SPECT/CT showed 178 SLNs (2.12 SLNs) in 84 of the 90 patients (93% success rate), as shown in Table 5. Of the total 90 patients, 11 patients did not show any hot nodes on the planer images alone, of which six patients (4 invasive ductal carcinomas (IDC), one ductal carcinoma in situ (DCIS), and one invasive lobular carcinoma (ILC)) did not show any hot nodes on SPECT/CT images as well. Of the remaining patients (5/11), two (one IDC and one ILC) showed metastatic nodes on surgery and were neither seen on the SPECT/CT nor planer images. These lymph nodes were enlarged, showing hilar effacement and cortical thickening on the CT component. The time range between the initial image acquisition and the start of the axillary dissection in most cases is between 90 to 120 min.
Two patients (one with DCIS and one with IDC) showed questionable hot foci on PS and were not detected on SPECT/CT. All these foci were highly suggestive of focal activity within tortuous lymphatic channels rather than lymph node uptake, which emptied by the time the SPECT/CT images were acquired. Therefore, these nodes were not labeled as SLN on the nuclear medicine report.
The locations of hot nodes seen on the fused SPECT/CT images were categorized into 122 (69%) at level I, 38 (21%) at level II, and 9 (5%) at level III. SPECT/CT additionally localized 3 (2%) at the intramammary level and 6 (3%) hot nodes at the supraclavicular region (where one patient presented with two hot supraclavicular nodes on SPECT/CT).
In our study, SPECT/CT detected 26 more hot nodes missed by planar images alone. Four of these nodes were located in supraclavicular and two in the internal mammary drainage sites ipsilateral to the tumor side.
In 33% (30/90) of the cases, only one focus was visualized on SPECT/CT, while in 30% (27/90), two foci of hot nodules were seen, leading to 57 cases with a radiological low nodal burden. Whereas in 19 (21%) patients, three foci were seen on SPECT/CT imaging, and four or more lymph nodes were identified in 8 (9%) patients (radiological high nodal burden). In 6 (7%) cases, no hot foci were identified.
Operative and pathological findings
Out of the total surgically excised (n = 706), 103/706 nodes were tumor positive, and 603/706 nodes were histopathologically free of tumor. The 706 nodes were excised based on surgical suspicion or detection by the gamma finder probe during the operative procedure. Not all hot nodes were positive; however, two involved SLNs visualized only on SPECT/CT and were the only tumor-positive nodes excised, which led to a change in management and the TNM stage of breast cancer. In addition, morphological characterization of the abnormal lymph nodes on the CT part (Table 1) helped the surgeon identify the abnormal nodes in almost every case.
Discussion
The presence of axillary lymph node metastases is an established indicator of poor prognosis of the 5-year survival, declining by approximately 8% to 40%. Therefore, SLNB is now the practice of choice for managing many patients with breast cancer to improve the loco-regional control of the disease and improve patient survival by reducing morbidity related to intraoperative and postoperative complications such as bleeding pain and chronic lymphedema [5, 17].
The concept of SLNB has largely replaced ALND for patients with clinically and histologically tumor-free lymph nodes. Evidence suggests that if the SLNB is negative, there is no need for ALND, and there are negligible chances of recurrence compared to the cases that undergo ALND [18,19,20]. Therefore, the identification of SLN has become imperative in the management of axillary dissection.
Hybrid SPECT/CT in SLNB has a time-proven advantage over PS in localization and characterization of the axillary lymph nodes [21]. In our study, SPECT/CT successfully localized SLNs in 93% of the patients compared to PS alone (P value < 0.005), comparable with the data published by Stanzel S. et al. [13] and showed 26 additional SLNs compared to PS, along with precise localization of axillary levels (Figs. 1 and 2).

48-year-old female with invasive ductal carcinoma of the left breast. A, B PS demonstrating activity within multiple lymphatic channels. Two hot left axillary nodes are noted. C–F The fused SPECT/CT images pinpoints the level-I left axillary node. The medial focus (arrow) turned to be a left Interpectoral lymph node (Rotter's nodes)

36-year-old female with invasive ductal carcinoma of the left breast. A, B PS demonstrates multiple foci of activity in the left axilla, two of which along the midclavicular line. C, D Hybrid cross-sectional SPECT/CT images demonstrate the foci of activity lateral to the pectoralis minor station at Level-I. The lateral focus shows three small matted axillary nodes (arrow)
As inferred by Siddique M et al. [21], our SPECT/CT imaging detected 26 additional hot nodes missed by PS alone, including nodes (n = 18) located in the drainage sites, which are not routinely explored during surgery such as internal mammary (Fig. 3) and supraclavicular regions 3(2%) and 6 (3%), respectively.

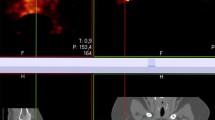
A 43-year-old female with invasive ductal carcinoma of the left breast. A, B PS demonstrates multiple lymphatic channels with tracer accumulation near the parasternal area, as shown with the arrow. C, D Hybrid SPECT/CT demonstrates the focus of activity at the inferior border of the left first rib medially(arrow), i.e., Intra-thoracic (internal mammary) nodal uptake
Husarik DB. et al. [22] showed that hybrid SPECT/CT provides more accurate information of the anatomical axillary levels as high as up to 100% of patients due to 3-D image processing. Similarly, in our study, more than 90% of the nodes were found at the axillary level I & II, followed by 5%, 3%, and 2% of the SLNs seen at the axillary level III, supraclavicular, and internal mammary levels, respectively (Table 4). All identified hot axillary SLNs were resected along with 528 non-SLNs, except six supraclavicular and three internal mammary nodes. Of the 706 dissected LNs, only 103 (15%) were tumor-positive (Fig. 4), whereas 603 (85%) were free of tumors (Table 3).

showing histopathology and immunochemical stains of an internal mammary lymph node showing metastatic intraductal carcinoma A Hematoxylin and eosin 12 × B Progesterone receptor C Her-2-neu receptor D Estrogen receptor
In addition to anatomical localization, the CT part of SPECT/CT was used to characterize the LN morphology for possible tumor involvement based on the radiological feature (Table 1). 138/178 LNs were identified as normal morphology according to the CT criteria [23]. 40/178 LNs showed abnormal morphology mainly in size, shape, hilar effacement, or cortical involvement, as shown in Fig. 5. In a non-contrast CT study, hilar effacement is suggested by displacement of the fatty hilum that appears non-central in the lymph node and is confirmed on more than one plane on CT scan. In these cases, the hilum is not entirely replaced with tumor tissue. In our study, 2/90 patients showed metastatic nodes on surgery that were not seen on the SPECT images. These lymph nodes demonstrated morphological features of metastasis, such as enlargement with hilar effacement and cortical thickening on the CT component of the study.

Characterization of CT features of sentinel lymph nodes detected on SPECT/CT showing A Pleomorphic calcification, B Round, C Enlargement with hilar effacement and loss of hilar fat, D Enlarged with nodal replaced with tumor
The average score for observers one and two was 2.4 ± 0.71 and 2.53 ± 0.52, respectively, with a substantial agreement (k = 0.76). Many lymph nodes had more than one abnormal radiological feature on CT. The SPECT/CT findings of nodal morphology described in Table 1 were conveyed to the surgeons and were found valuable by the operating surgeons and specified the surgical approach in almost all the above cases.
Two false-positive cases were seen in the PS. They were negative on SPECT/CT, likely due to the focal activity within tortuous lymphatic channels that cleared before the SPECT/CT images were acquired. Serrano-Vicente et al. elaborate on the value of hybrid imaging in such cases, especially if unexpected lymphatic drainage is suspected [24]. Two false-negative patients on SPECT/CT showed metastatic lymph nodes on surgery and histopathology out of six cases in which SPECT/CT could not localize the SLN. However, all six patients showed activity in the surgical bed after removing the SLN, which indicates that there are still lymph nodes receiving the injected activity even after the imaging process. In all our cases, the average time between the imaging and the start of the axillary dissection was 180 min (± 30). The slower flow of radiotracer to these lymph nodes could be due to multiple reasons such as old age (~ 85 years), high BMI of > 45 kg/m2, large or dense breasts, injection techniques, and particle size, primary tumor size which is in correlation to already published data [25,26,27,28]. One more hypothesis is that delay in activity reaching axillary lymph nodes is probable due to metastatic cell deposits in the lymphatic channels draining in these nodes, which slows the lymph flow and, hence, the activity reaching the nodes.
Hybrid SPECT/CT systems have improved over the past decade to a level to provide cross-sectional details of axilla along with fine morphological details of the lymph nodes during SLNB [29]. No additional intervention is required except for an additional 10–15 min for the scan. Low-dose CT with improved modern algorithms provides a global view of breast drainage areas at a negligible absorbed dose. According to the measured DLP from the low-dose CT performed in our study, none of the cases exceeded 3.0 mSv in our one-day protocol study. Our research is unique in evaluating the feasibility of RNL SPECT/CT during SLNB as a potential tool for providing anatomical axillary levels and morphological features of potentially involved lymph nodes. These data can be carefully translated into low and high axillary nodal burden, which can help surgeons decide whether to go for ALND or otherwise. In our study, surgeons decided on ALND on two patients, entirely relying on the CT characterization and GPD when the SPECT images were negative. Therefore, CT findings of abnormal lymph node morphology were used as a reason for the surgeon to remove these nodes even when they were not seen on the PS or SPECT images. Besides, six patients demonstrated uptake in axillary lymph nodes using the gamma detector probe initially not seen on the delayed planer and SPECT images. These explain why the number of excised lymph nodes (n = 706) exceeds the number of hot LNs (n = 178). Hot nodes labeled as SLN are not necessarily metastatic; negative LNs on scintigraphy are not always clear of disease. Although the EANM guidelines (2013) state that removing more than five nodes from the axilla does not result in marked improvement in sensitivity of axillary biopsy, the average number of excised nodes in our study was around eight nodes per axilla. The higher number relates to the threshold of the surgeons operating in such cases in our center.
Additionally, SPECT/CT showed (26 LNs) 17% more nodes (178 vs. 152), indicating significant statistical significance (P = 0.05) compared to PS alone, of which 4/26 nodes (15%) turned to be metastatic on histopathology. The current study explored the potential of SLNB with SPECT/CT imaging protocol as a potential tool for clinical staging of the axilla; however, more detailed prospective studies are required to evaluate the possibility of inclusion of SLNB with SPECT/CT as an adjunct imaging modality during the pre-surgical clinical axillary nodal staging of breast cancer.
Limitations of the study
The study's limitations include a small cohort; however, further studies are continued to explore the utility of the current initial experience of applying SLNB SPECT/CT in TNM staging of breast cancer. In addition, although the CT component also details the primary tumor, tumor multifocality, and the status of the contralateral axilla, mediastinum, and lungs, those findings are beyond this manuscript's scope.
Conclusions
Cross-sectional SPECT/CT imaging detects a higher number of nodes when compared to PS. Additionally, the CT part provides anatomical information on the bilateral axillary levels, bilateral breast, lungs, mediastinum, and morphology of lymph nodes, which can restage the disease and significantly impact pre- and post-surgical management of the patients in terms of pre-surgical cTNM and selective ALND. However, further protocol optimization is needed on a larger cohort to justify adding this protocol in initial axillary nodal staging.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author upon request.
Abbreviations
- 3-D:
-
Three dimensional
- ABER:
-
Abducted and externally rotated
- ALND:
-
Axillary lymph node dissection
- BMI:
-
Body mass index
- cm:
-
Centimeter
- CT:
-
Computed tomography
- cTNM:
-
Clinical tumor, node, metastasis (classification of malignant tumors)
- DCIS:
-
Ductal carcinoma in situ
- DLP:
-
Dose length product
- EANM:
-
European Association of Nuclear Medicine
- GDP:
-
Gamma-ray detector probe
- IDC:
-
Invasive ductal carcinoma
- ILC:
-
Invasive lobular carcinoma
- LEHR:
-
Low-energy high-resolution
- LN:
-
Lymph node
- mCi:
-
Millicurie
- MRI:
-
Magnetic resonance imaging
- OSEM:
-
Ordered subset expectation maximization
- PS:
-
Planar scintigraphy
- RNL:
-
Radionuclide lymphoscintigraphy
- SLN:
-
Sentinel lymph node
- SLNB:
-
Sentinel lymph node biopsy
- SPECT:
-
Single photon emission computer tomography
- T1:
-
Tumor is 2 cm (3/4 of an inch) or less across
- T2:
-
Tumor is more than 2 cm but not more than 5 cm (2 inches) across
- TNM:
-
Tumor, node, metastasis (classification of malignant tumors)
- US:
-
Ultrasonography
References
Schwartz GF, Veronesi U, Clough KB, Dixon JM, Fentiman IS, Heywang-Köbrunner SH, Holland R, Hughes KS, Mansel RE, Margolese R, Mendelson EB, Olivotto IA, Palazzo JP, Solin LJ (2006) Consensus Conference Committee. Consensus conference on breast conservation, Milan, Italy, April 28-May 1 2005. Breast J 12(4):398–407
Lyman G, Somerfield M, Bosserman L, Perkins C, Weaver D, Giuliano A (2017) Sentinel lymph node biopsy for patients with early-stage breast cancer: american society of clinical oncology clinical practice guideline update. J Clin Oncol 35(5):561–564
Pilewskie M, Morrow M (2017) Axillary nodal management following neoadjuvant chemotherapy. JAMA Oncol 3(4):549
Li CZ, Zhang P, Li RW, Wu CT, Zhang XP, Zhu HC (2015) Axillary lymph node dissection versus sentinel lymph node biopsy alone for early breast cancer with sentinel node metastasis: A meta-analysis. Eur J Surg Oncol 41(8):958–966
Mariani G, Erba P, Villa G, Gipponi M, Manca G, Boni G, Buffoni F, Castagnola F, Paganelli G, Strauss HW (2004) Lymphoscintigraphic and intraoperative detection of the sentinel lymph node in breast cancer patients: the nuclear medicine perspective. J Surg Oncol 85(3):112–122
Ahadiat O, Higgins S, Kwon S, Wysong A (2018) Underuse of the sentinel lymph node biopsy for high-risk squamous cell carcinoma of the skin. JAMA Dermatol 154(1):101
Gangi A, Essner R, Giuliano AE (2014) Long-term clinical impact of sentinel lymph node biopsy in breast cancer and cutaneous melanoma. Q J Nucl Med Mol Imaging 58(2):95–104
Zavagno G, De Salvo GL, Scalco G, Bozza F, Barutta L, Del Bianco P, Renier M, Racano C, Carraro P, Nitti D (2008) GIVOM Trialists. A randomized clinical trial on sentinel lymph node biopsy versus axillary lymph node dissection in breast cancer: results of the Sentinella/GIVOM trial. Ann Surg. 247(2):207–13
Wang Y, Dong H, Wu H, Zhang L, Yuan K, Chen H, Jiao M, Fu R (2015) Improved false negative rate of axillary status using sentinel lymph node biopsy and ultrasound-suspicious lymph node sampling in patients with early breast cancer. BMC Cancer. 2015(15):382
Straver ME, Meijnen P, van Tienhoven G, van de Velde CJ, Mansel RE, Bogaerts J, Duez N, Cataliotti L, Klinkenbijl JH, Westenberg HA, van der Mijle H, Snoj M, Hurkmans C, Rutgers EJ (2010) Sentinel node identification rate and nodal involvement in the EORTC 10981–22023 AMAROS trial. Ann Surg Oncol 17(7):1854–1861
Bergkvist L, Frisell J, Liljegren G, Celebioglu F, Damm S, Thörn M (2001) Multicentre study of detection and false-negative rates in sentinel node biopsy for breast cancer. Br J Surg 88(12):1644–1648
Goyal A, Newcombe RG, Chhabra A, Mansel RE (2006) ALMANAC Trialists group. Factors affecting failed localisation and false-negative rates of sentinel node biopsy in breast cancer–results of the ALMANAC validation phase. Breast Cancer Res Treat. 99(2):203–8
Stanzel S, Pernthaler B, Schwarz T, Bjelic-Radisic V, Kerschbaumer S, Aigner RM (2018) Diagnostic and prognostic value of additional SPECT/CT in sentinel lymph node mapping in breast cancer patients. Nuklearmedizin 57(3):92–99
Even-Sapir E, Lerman H, Lievshitz G, Khafif A, Fliss DM, Schwartz A, Gur E, Skornick Y, Schneebaum S (2003) Lymphoscintigraphy for sentinel node mapping using a hybrid SPECT/CT system. J Nucl Med 44(9):1413–1420
Lerman H, Metser U, Lievshitz G, Sperber F, Shneebaum S, Even-Sapir E (2006) Lymphoscintigraphic sentinel node identification in patients with breast cancer: the role of SPECT-CT. Eur J Nucl Med Mol Imaging 33(3):329–337
Valdés Olmos RA, Rietbergen DD, Vidal-Sicart S, Manca G, Giammarile F, Mariani G (2014) Contribution of SPECT/CT imaging to radioguided sentinel lymph node biopsy in breast cancer, melanoma, and other solid cancers: from “open and see” to “see and open.” Q J Nucl Med Mol Imaging 58(2):127–139
Whitman G, AlHalawani R, Karbasian N, Krishnamurthy R (2019) Sentinel lymph node evaluation: what the radiologist needs to know. Diagnostics 9(1):12
Kiluk JV, Ly QP, Meade T, Ramos D, Reintgen DS, Dessureault S, Davis M, Shamehdi C, Cox CE (2011) Axillary recurrence rate following negative sentinel node biopsy for invasive breast cancer: long-term follow-up. Ann Surg Oncol 18(Suppl 3):S339–S342
Edge SB, Niland JC, Bookman MA, Theriault RL, Ottesen R, Lepisto E, Weeks JC (2003) Emergence of sentinel node biopsy in breast cancer as standard-of-care in academic comprehensive cancer centers. J Natl Cancer Inst 95(20):1514–1521
Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW, Blumencranz PW, Leitch AM, Saha S, McCall LM, Morrow M (2011) Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA 305(6):569–575
Siddique M, Nawaz MK, Bashir H (2018) The usefulness of SPECT/CT in sentinel node mapping of early stage breast cancer patients showing negative or equivocal findings on planar scintigraphy. Asia Ocean J Nucl Med Biol 6(2):80–89
Husarik DB, Steinert HC (2007s) Single-photon emission computed tomography/computed tomography for sentinel node mapping in breast cancer. Semin Nucl Med 37(1):29–33
Ecanow J, Abe H, Newstead G, Ecanow D, Jeske J (2013) Axillary staging of breast cancer: what the radiologist should know. Radiographics 33(6):1589–1612
Serrano-Vicente J, Rayo-Madrid J, Domínguez-Grande M, Infante-Torre J, García-Bernardo L, Moreno-Caballero M et al (2015) Role of SPECT-CT in breast cancer sentinel node biopsy when internal mammary chain drainage is observed. Clin Transl Oncol 18(4):418–425
Nowikiewicz T, Głowacka-Mrotek I, Tarkowska M, Nowikiewicz M, Zegarski W (2020) Failure of sentinel lymph node mapping in breast cancer patients qualified for treatment sparing axillary lymph nodes-Clinical importance and management strategy-One-center analysis. Breast J 26(5):873–881
Aliakbarian M, Memar B, Jangjoo A, Zakavi SR, Reza Dabbagh Kakhki V, Aryana K, Forghani MN, Sadeghi R (2011) Factors influencing the time of sentinel node visualization in breast cancer patients using intradermal injection of the radiotracer. Am J Surg. 202(2):199–202
Wosnitzer B, Mirtcheva R, Ghesani M (2010) Nonvisualization of sentinel node by lymphoscintigraphy in advanced breast cancer. Radiol Case Rep 5(3):444
Yang J, Xu L, Liu P, Du Z, Chen J, Liang F, Long Q, Zhang D, Zeng H, Lv Q (2020) Accuracy of sentinel lymph node biopsy in breast cancer: pitfalls in the application of single tracers. Cancer Manag Res. 12:3045–3051
Israel O, Pellet O, Biassoni L, De Palma D, Estrada-Lobato E, Gnanasegaran G, Kuwert T, la Fougère C, Mariani G, Massalha S, Paez D, Giammarile F (2019) Two decades of SPECT/CT - the coming of age of a technology: An updated review of literature evidence. Eur J Nucl Med Mol Imaging 46(10):1990–2012
Acknowledgements
Not applicable.
Funding
No funds, sponsorship, or financial support are to be disclosed.
Author information
Authors and Affiliations
Contributions
MG suggested and developed the research idea, shared in data collection and analysis, shared in statistical analysis, shared in manuscript writing, revision, and editing, and prepared figures and tables. RR, SO, AA, and RA shared in data collection and analysis, shared in reviewing the literature, shared in collecting data, and performing statistical analysis. MG, AA, and RR reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethical approval was obtained from the Ethical Committee at the Faculty of Medicine, Kuwait University. However, the informed consent for the case review was waived as the images were used completely anonymously.
Consent for publication
Not applicable as it is a retrospective study, and it was waived by the ethical committee. The proof of consent to publish from study participants can be requested at any time.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ghanem, M., Rasheed, R., Almousawi, A. et al. Redefining the clinical axillary lymph node staging using SPECT/CT in early breast cancer during SLNB. Egypt J Radiol Nucl Med 53, 234 (2022). https://doi.org/10.1186/s43055-022-00913-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00913-x