
Abstract
Background
Imaging of idiopathic inflammatory myopathies (IIMs) is challenging, and no pathognomonic signs exist. Different tracers have been tested for this purpose, mainly inflammation markers including technetium-99m-pyrophosphate (PYP). We aimed to examine the utility of fluorine-18-fluorodeoxyglucose (FDG) relative to PYP in idiopathic inflammatory myopathy (IIM).
Methods
Using visual grading and CT-guided muscular segmentation and standardized uptake values (SUVs), we assessed muscular tracer uptake qualitatively and quantitatively, comparing FDG uptake in eight patients with recent-onset IIM and 24 healthy control persons and FDG and PYP uptake in seven patients.
Results
Muscular FDG and PYP uptake was increased in all patients. However, uptake distribution and signal intensity differed considerably. FDG scans revealed clear involvement of certain muscle groups including core and swallowing muscles and, in addition, abnormality in diseased extra-muscular organs. PYP was mainly visible in bones, whereas muscular PYP uptake was generally discrete and primarily located in the extremities. Quantitatively, FDG uptake was significantly higher in patients than in controls; the volume-weighted SUVmean for all right-side muscles was 0.84 versus 0.60 g/ml (95% confidence interval (CI) for mean difference 0.14–0.34, p = 0.0001). FDG SUVmean values were up to four times higher than PYP mean values in upper limb muscles (95% CI for the mean ratio 2.37–3.77, p = 0.0004) and two–three times higher in lower limb muscles (95% CI for the mean ratio 2.28–2.71, p < 0.0001).
Conclusions
Muscular FDG uptake was higher in treatment-naïve IIM patients than in healthy controls and more distinct than PYP uptake in patients with a potential to reveal extra-muscular IIM involvement and malignancy. Thus, FDG appears to be superior to PYP in the diagnostic evaluation of IIM.
Similar content being viewed by others


Key points
-
First head-to-head comparison of FDG and PYP uptake in IIM patients,
-
Quantification of tracer uptake done in standardized volumes of interest,
-
FDG uptake was significantly higher in patients than in controls; in patients, FDG uptake was two–three times as high as PYP uptake and revealed an extra-muscular disease in half,
-
Dissimilarities in tracer uptake add new aspects to our understanding of functional imaging in IIM.
Background
Idiopathic inflammatory myopathies (IIMs) constitute a group of rare conditions characterized by inflammation in skeletal muscles and various extra-muscular organs [1]. The muscular inflammation causes progressive, symmetrical muscle weakness that typically develops in weeks to months. IIMs affect the proximal muscles of the extremities, neck, and swallowing muscles; cover different subsets, including immune-mediated necrotizing myopathy (IMNM), polymyositis (PM), and dermatomyositis (DM); and are associated with increased mortality [2]. In DM patients, the frequency of underlying cancer is 20–25% [3]. When malignancy develops within 1–2 years of the myositis diagnosis, the term cancer-associated myositis (CAM) is used.
The diagnosis of IIM is based on criteria that developed over the years [4,5,6], but up to the present, the criteria did not include image formation. As the diagnosis of these rare diseases is still challenging, it calls for the development of new tools. The diagnostic value of different imaging modalities has been richly investigated with a focus on magnetic resonance imaging (MRI) and less so on ultrasound and nuclear imaging [7]. Various radionuclides have been applied, primarily inflammation markers and anti-myosin tracers [8]. Technetium-99m-pyrophosphate (PYP), which is a bone-seeking agent showing muscular uptake in the case of myopathy, was formerly the predominant surrogate marker of inflammation [9]. In recent years, concurrently with the general widespread use of positron emission tomography (PET)—also for detection of malignancy in IIM patients—fluorine-18-fluorodeoxyglucose (FDG) has become more popular for imaging of myopathy [10,11,12,13]. We previously found muscular PYP uptake in IIM patients at different stages to be higher than that of healthy controls [14]. In the present paper, we performed a head-to-head comparison of FDG and PYP uptake in recent-onset, treatment-naïve IIM patients to elucidate these tracers' similarities and dissimilarities and, thereby, their potential diagnostic value in this field.
Methods
Population
This is an explorative case series. As part of a controlled, cross-sectional population-based study described in detail elsewhere [15, 16], 90 consecutive patients with IIM (according to the classification criteria by Peter and Bohan [4, 5]) referred to rheumatology departments at two different hospitals over 18 months underwent PYP scintigraphy in terms of single-photon emission computed tomography combined with computed tomography (PYP SPECT/CT) at our center to characterize muscular uptake of this tracer. Patients with overlap syndromes (having another autoimmune rheumatic disease aside from IIM) or sporadic inclusion body myositis were excluded. Fourteen patients were newly diagnosed and untreated. Eight of these also underwent an FDG PET/CT scan as part of their clinical work-up, and in seven of them, a direct comparison of FDG and PYP uptake was feasible. Healthy FDG controls were picked from a population participating in an investigation on the normal FDG uptake [17]. In the present study, each PET/CT patient was gender- and age-matched with three control subjects; hence, there were 24 FDG controls.
Myositis baseline measures
Patients underwent various clinical, biochemical, and histological analyses as part of the diagnostics. These included manual muscle tests of eight muscle groups (MMT8) with each muscle scoring 1–10, yielding a possible maximum score of 80, serum levels of the muscle-associated enzyme creatine kinase (CK) [18], muscle biopsy analyses, and myositis-specific/myositis-associated autoantibody testing by immunoblot (EUROLINE Myositis Antigens Profile 3 (IgG) (anti-Mi-2, SRP, PL-7, PL-12, OJ, EJ, Jo1, PM-Scl75/100, Ro52, KU), not including anti-NXP2, TIF1γ, SAE1, and MDA5) [19]. Muscle weakness was defined as MMT8 < 80, and an increased CK level was defined as CK above the upper reference level at our laboratory (200 IU/l) [20, 21].
FDG PET/CT
FDG was administered intravenously in a dose of 4.0 megabecquerel (MBq) per kg body weight after a fast of at least 6 h. Afterward, the participants were resting in a quiet and warm room for 60 min. Four patients were scanned with arms above their heads, whereas four patients were unable to lie in this position. Scans were performed on integrated PET/CT scanners (GE Discovery 690, VCT, RX, or STE) with comparable spatial resolution. CT was low-dose non-contrast-enhanced (140 kV, smart mA, noise index 25, 30–110 mA). PET images were acquired in 3D mode from the base of the skull to the thighs (6–7 bed positions, acquisition time 2.5 min per bed position) and reconstructed into trans-axial slices with a matrix of 128 × 128 iterative reconstruction (two iterations, 21–28 subsets). They were corrected for attenuation, scatter, random coincidences, and scanner dead time.
PYP SPECT/CT
A dose of 550 MBq of PYP was administered intravenously. Three hours after injection, the patients had a SPECT/CT of the thorax (arms along the body except in one patient whose CT radiation dose was kept at a minimum because of her young age) and a SPECT/CT of the pelvis and thighs (apart for the above-mentioned patient) on a Siemens Symbia T16 SPECT/CT scanner. Collimators were low energy high resolution with a 15% window centered on the 140 keV photopeak of technetium-99m. SPECT parameters were 128 × 128 matrix, 64 projections, 40 s per frame at the upper body, and 20 s per frame at the lower body. The lower body scan was accomplished as a two-bed acquisition. CT was performed as a low-dose non-contrast-enhanced scan (130 kV, 20 mAS). SPECT data were reconstructed iteratively (four iterations, four subsets) with scatter and attenuation correction as well as resolution recovery. An 8-mm Gaussian filter was applied afterward.
Comparison of tracer uptake
Scans were evaluated qualitatively as well as quantitatively. By qualitative evaluation of reconstructed 3D models (maximum intensity projections, MIPs) and trans-axial slices, performed by a specialist in nuclear medicine with 20 years of experience (JAS) and with inspiration from the literature [22], “+,” “++,” and “+++” indicated mildly, moderately, and severely increased tracer uptake, respectively, compared with the normal picture. With the purpose of a quantitative comparison of the skeletal muscle uptake of patients and controls and different tracers, the activity within the muscles was measured in standardized volumes of interest (VOIs) delineated by the use of Siemens Syngo medical imaging software (Siemens Healthcare, Ballerup, Denmark). Muscles were defined manually on the CT images, and successive trans-axial regions of interest were added up to create VOIs for the different muscles. For the comparison of FDG and PYP uptake, muscles visible on both scan types were chosen; these were the deltoid muscle, gluteal muscle, and proximal parts of the arm and thigh muscles on the right side. The size of the different VOIs was registered, and volume-weighted uptake values were calculated to compare average FDG and PYP uptake in several muscles.
From PET/CT scans, mean and maximum standardized uptake values (SUVs in g/ml) were read directly. From SPECT/CT scans, the mean and maximum number of counts per voxel (counts per second per ml) were registered and the mean and maximum voxel activities (Bq/ml) were calculated from knowledge of the camera sensitivity (counts per second per MBq). The latter was measured using a known amount of 99mTc [23]. The activity was decay corrected according to the time of injection and normalized to injected activity (MBq) per kg body weight. The result was an SUV measured in g/ml.
Statistics
Continuous variables are presented as mean ± standard deviation or mean (range). Inter-group comparisons were made using Student’s t-tests. As to muscle tracer uptake, 95% confidence intervals (CI) for the mean difference or ratio are given. Categorical variables are presented as frequencies (percentages) and were compared by the Chi-squared test. Correlations were assessed by Spearman’s rho. p values < 0.05 were considered significant. Statistical analyses were performed with STATA/IC 11.2 (©StataCorp LP, College Station, Texas, USA).
Results
Patients had a mean age of 63.0 ± 20.9 years, and 75% were women. Sex, age, height, weight, and body mass index did not differ significantly between patients and controls (Additional file 1: Table).
Patient characteristics are shown in Table 1. The patients were re-classified according to the new ACR/EULAR classification criteria from 2017 [6]; three patients had PM/IMNM, one had possible IIM, and four had DM. The patient with possible IIM was clinically diagnosed with statin-induced IMNM, based on former statin exposure, the muscle biopsy dominated by necrosis, and response to immunosuppressive. Two of the patients with DM turned out to have cancer: one esophageal and one pulmonary.
Mean MMT8 was 68 (56–74). The average CK value was 2765 (144–9527) IU/l (data not shown elsewhere). Hence, all patients had muscle weakness, and all patients but one had increased CK levels. No correlation was found between CK level and MMT8; rho = − 0.32, p = 0.43. Five patients had histological signs of muscular inflammation, whereas two patients with DM had negative biopsies and one patient with PM only revealed necrosis in the muscle biopsy (Table 1).
Qualitative comparison of FDG and PYP uptake
By qualitative evaluation of the scans, all patients had increased muscular FDG uptake. Additionally, all SPECT/CT scans showed increased PYP uptake. PYP and FDG uptakes were not increased to the same degree in individual patients; PYP could be only mildly increased, while FDG was moderately or severely increased, and vice versa (Table 1). A qualitative comparison of the two tracers is illustrated in Figs. 1,2, and 3. In Fig. 1, MIPs of FDG PET/CT and PYP SPECT/CT are compared one-to-one for all seven patients who underwent both scan types. It is apparent that PYP is a bone tracer with variable uptake in skeletal muscles in these patients, whereas the FDG scans consistently showed a higher than normal muscular uptake. In both cases, muscular uptake was predominantly symmetrical, yet somewhat patchy. FDG added extra information about some of the patients. Patient number 4 had an avid FDG activity in her throat corresponding to severe dysphagia. Patient number 7 was considerably weakened and had dysphagia; her FDG scan, too, showed an activity in the throat as well as in a lung infiltrate due to aspiration. Patient number 2 had a high FDG uptake in the esophagus and cervical and mediastinal lymph nodes, representing cancer and metastases. Patient number 6 had an avid FDG uptake in lung nodules and mediastinal lymph nodes representing malignant lesions. Examples of the FDG uptake in healthy control persons for comparison are given in Additional file 2: Figure.

Maximum intensity projections of seven patients undergoing both PYP SPECT/CT of the thorax (upper row) and lower body (middle row) and FDG PET/CT whole-body scans (lower row). SPECT/CT was routinely performed with the patient’s arms along the body. For PET/CT, patients normally have their arms up. In the present material, patients 2, 5, 6, and 7 were not able to lie in that position

Corresponding trans-axial slices from PYP and FDG scans in a patient number 4 and b patient number 5. PYP scans are shown in a warm color scale in upper rows, and FDG scans are shown in a thermal scale in lower rows. Muscular FDG hot spots are indicated by red arrows. Minor misalignments are due to a slightly varying positioning of the patients on the two scan occasions

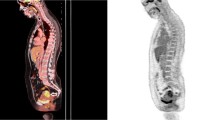
Corresponding trans-axial, coronal, and sagittal slices from PYP (upper row) and FDG (lower row) scans in one of the patients. With FDG, focally increased tracer uptake is seen in the caudal part of the esophagus (red arrow). A similar focus was not identified by PYP scintigraphy
In Fig. 2, trans-axial slices are shown for two of the patients with distinct muscular hot spots by FDG. These hot spots were not visualized to the same degree by PYP. Figure 3 shows the above-mentioned esophagus cancer demonstrated by FDG, but not by PYP.
Quantitative comparison of FDG uptake in patients and controls
Muscular FDG uptake values are shown in Table 2. Patients had significantly higher uptake values than controls, the difference being most marked for the upper limbs.
The volume-weighted average FDG SUVs were correlated with CK (rho = − 0.88, p = 0.004 for SUVmean; rho = − 0.76, p = 0.03 for SUVmax), whereas no correlation was found with MMT8 (data not shown). The FDG uptake in the right deltoid, biceps, gluteus, and quadriceps muscles did not correlate with MMT for the respective muscles (data not shown).
Quantitative comparison of FDG and PYP uptake in patients
A quantitative comparison of FDG- with PYP uptake in the same muscles of seven patients is presented in Table 3 as regards SUVmean and SUVmax. The FDG uptake values were three–four times higher than the PYP uptake values in the upper limb and two–three times higher in lower limb muscles.
Discussion
To our knowledge, this is the first direct comparison of muscular tracer uptake in treatment-naïve IIM patients assessed qualitatively and quantitatively by traditional PYP SPECT/CT and more recently applied FDG PET/CT imaging. The eight IIM patients differed considerably clinically, biochemically, and histologically. Scans exhibited different patterns and degrees of muscular tracer uptake in a way that no clear relationship between clinical parameters and imaging findings emerged. These results are in line with MRI findings, which correlate only to a limited extent with other parameters of disease activity in myositis [24]. In addition, we found no correlation between CK level and MMT8. FDG uptake was negatively correlated with CK and uncorrelated with muscle strength tests. Previously reported results were similarly ambiguous. Some authors found a correlation between SUV of FDG and myositis severity, muscle strength, and the extent of inflammatory infiltrate in biopsy [25,26,27,28], while others found no correlation of FDG findings with paraclinical or clinical parameters [13, 29, 30]. The reason may be a heterogeneous disease manifestation as described by Sun et al., who noted that an average SUV is not necessarily representative of the activity and severity of muscles specifically affected in IIM patients [31]. Similarly, one may argue that isolated SUVmax values can hardly be true representatives of non-uniform disease. Moreover, edema and muscle atrophy with potential fat replacement may occur to varying extents and lower average tracer uptake [24]. However, with cases of extra-muscular uptake and visualization of swallowing muscles as well, FDG findings were more in line with patient characteristics than PYP results.
The generally two–three times higher FDG uptake was not correlated with the lower PYP uptake, suggesting that the two tracers mirror different characteristics of the same muscle-degrading disease. Skeletal muscle uptake of PYP in case of muscular injury is well described [32] and thought to be an uptake in calcium deposits arising in areas of inflammation or ischemia, without discrimination between inflammatory and non-inflammatory causes of myopathy [33,34,35]. In our previous quantitative study with 90 IIM patients (chronic as well as acute), there was a significant difference between PYP uptake in patients and healthy controls with no overlap in 95% CI but wide and overlapping ranges underlining the vast heterogeneity of the disease [14]. Muscular uptake is easily seen by qualitative evaluation, but no scintigraphical signs pathognomonic for IIM exist, and a more specific tracer is direly warranted. Besides, the spatial resolution and sensitivity of the SPECT/CT modality are inferior to those of the PET/CT modality [36].
FDG is a glucose analog whose cellular uptake is proportional to the metabolic activity of the cells. The value of FDG in the diagnosis of inflammation as well as malignancy is well established, and FDG PET/CT is used in rheumatologic diseases such as rheumatoid arthritis, vasculitis, and polymyalgia rheumatica [37,38,39,40]. Recently, its use in IIMs has also been described, and researchers have demonstrated higher SUVs in patients than controls [25, 29] or persons with non-inflammatory muscle disease [41], but also an overlap of FDG uptake in patients with IIM and without [31]. On the whole, there seems to be a wide distribution range of FDG uptake in IIM patients [25, 26, 30, 31]. FDG PET/CT is sensitive but unspecific; the increased FDG uptake in skeletal muscles may be indicative of inflammation/injury, but also of physical activity right before or during the time from tracer injection to imaging, high insulin levels, and other reasons [42, 43].
FDG was not previously compared directly with PYP in IMM patients, but it has been studied along with the PET bone tracer, fluorine-18-sodium fluoride (NaF), with characteristics similar to those of PYP for the detection and quantification of early-stage atherosclerosis [44,45,46]. NaF has no noticeable uptake in healthy muscles but is seen in injured muscle [47], where it is taken up by microcalcification (< 50 µm) [48] by a mechanism similar to that of PYP uptake into striated muscle and myocardium. In atherosclerosis, arterial wall FDG uptake is a waxing and waning process, and there is a remarkable little overlap between arterial wall uptake of FDG and NaF. NaF uptake signifies ongoing arterial wall calcification, which may vary over time in cardiovascular low-risk subjects, but appear to increase slowly in patients with angina pectoris [49]. Extrapolation from these observations suggests that there should not be a high degree of agreement between PYP and FDG uptake in skeletal muscles of IIM patients although there may well be some sort of connection, the most probable one being that a state of muscular inflammation in IIM may at times give rise to more severe tissue damage resulting in local necrosis, which is what is visualized by PYP imaging.
Even with the few patients examined head to head, the consistency of our data raises the question of the extent to which the two tracers demonstrate the same or different disease processes, and whether one is preferable or if they should rather be used supplementary. The FDG uptake may vary by the activity of the disease, and muscular PYP uptake may be larger (and thus detectable) than in healthy controls but only give rise to visible foci in case of significant focal muscular necrosis. This suggests that the two tracers show two sides and two stages, one more advanced than the other, of the same muscle-degrading disease.
It was a single-center study of a small number of patients with muscle segmentation performed manually but similarly in patients and healthy controls. We did not test the reproducibility of this procedure, since the estimation of proportions of agreement in small samples like ours would imply very wide 95% confidence intervals. We have previously tested semi-automated segmentation of thigh muscles and found acceptable but not optimal reproducibility [14], and we recognize that segmentation may be more challenging in the upper extremities with minor muscle groups, where SUVs in the present material differed more between patients and controls.
The myositis-specific autoantibodies anti-NXP2, TIF1γ, SAE1, MDA5, and HMGCR were not measured, as an older version of the immunoblot (EUROLINE Myositis Antigens Profile 3) was used. Even though the potential presence of these autoantibodies adds additional information to the patient group, none of these autoantibodies are included in the ACR/EULAR classification criteria from 2017.
Conclusions
IIM is a complex disease entity with various findings calling for a multi-faceted diagnostic approach. Nuclear imaging may support the diagnosis of IIM and carries several potentials including whole-body scanning. Both PYP and FDG accumulate in inflammatory muscle lesions but are not specific for inflammation. Compared with PYP, skeletal muscle uptake is more pronounced with FDG, which also allows for the evaluation of other organ involvement and cancer screening. The present data suggest that FDG PET/CT may be of diagnostic value in IIM and add to the body of knowledge necessary for further development of functional imaging in IIM, which we strongly encourage.
Availability of data and materials
The datasets used and/or analyzed during the current study are not publicly available due to legal regulation on anonymization but are available from the corresponding author upon reasonable request.
Abbreviations
- IIM:
-
Idiopathic inflammatory myopathy
- PYP:
-
Technetium-99m-pyrophosphate
- FDG:
-
Fluorine-18-fluorodeoxyglucose
- SUV:
-
Standardized uptake value
- IMNM:
-
Immune-mediated necrotizing myopathy
- PM:
-
Polymyositis
- DM:
-
Dermatomyositis
- CAM:
-
Cancer-associated myositis
- MRI:
-
Magnetic resonance imaging
- PET:
-
Positron emission tomography
- SPECT:
-
Single-photon emission computed tomography
- CT:
-
Computed tomography
- MMT8:
-
Manual muscle test of eight muscle groups
- CK:
-
Creatine kinase
- CI:
-
Confidence interval
- MIP:
-
Maximum intensity projection
- VOI:
-
Volume of interest
- NaF:
-
Fluorine-18-sodium fluoride
References
Sasaki H, Kohsaka H (2018) Current diagnosis and treatment of polymyositis and dermatomyositis. Mod Rheumatol 28:913–921. https://doi.org/10.1080/14397595.2018.1467257
Limaye V, Hakendorf P, Woodman RJ, Blumbergs P, Roberts-Thomson P (2012) Mortality and its predominant causes in a large cohort of patients with biopsy-determined inflammatory myositis. Intern Med J 42:191–198. https://doi.org/10.1111/j.1445-5994.2010.02406.x
Tripoli A, Marasco E, Cometi L, De Stefano L, Marcucci E, Furini F et al (2020) One year in review 2019: idiopathic inflammatory myopathies. Clin Exp Rheumatol 38:1–10
Bohan A, Peter JB (1975) Polymyositis and dermatomyositis (first of two parts). N Engl J Med 292:344–347. https://doi.org/10.1056/nejm197502132920706
Bohan A, Peter JB (1975) Polymyositis and dermatomyositis (second of two parts). N Engl J Med 292:403–407. https://doi.org/10.1056/nejm197502202920807
Lundberg IE, Tjarnlund A, Bottai M, Werth VP, Pilkington C, Visser M et al (2017) 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann Rheum Dis 76:1955–1964. https://doi.org/10.1136/annrheumdis-2017-211468
Kubínová K, Dejthevaporn R, Mann H, Machado PM, Vencovský J (2018) The role of imaging in evaluating patients with idiopathic inflammatory myopathies. Clin Exp Rheumatol 36(Suppl 114):74–81
Walker UA (2008) Imaging tools for the clinical assessment of idiopathic inflammatory myositis. Curr Opin Rheumatol 20:656–661. https://doi.org/10.1097/BOR.0b013e3283118711
von Kempis J, Kalden P, Gutfleisch J, Grimbacher B, Krause T, Uhl M et al (1998) Diagnosis of idiopathic myositis: value of 99mtechnetium pyrophosphate muscle scintigraphy and magnetic resonance imaging in targeted muscle biopsy. Rheumatol Int 17:207–213
Rivas-de Noriega JP, Galnares-Olalde JA, Zuniga-Varga J, Herrera-Felix JP, Alegria-Loyola MA, Turrent-Carriles A (2018) Utility of [(18)F] fluorodeoxyglucose positron emission tomography/computed tomography scan in inflammatory myopathies: case report and literature review. Case Rep Rheumatol 2018:8398453. https://doi.org/10.1155/2018/8398453
Zanframundo G, Tripoli A, Cometi L, Marcucci E, Furini F, Cavagna L et al (2021) One year in review 2020: idiopathic inflammatory myopathies. Clin Exp Rheumatol 39:1–12
Kim K, Kim SJ (2021) (18)F-FDG PET/CT for assessing of disease activity of idiopathic inflammatory myopathies. A systematic review and meta-analysis. Hell J Nucl Med 24:132–139. https://doi.org/10.1967/s002449912353
Yildiz H, D’Abadie P, Gheysens O (2022) The role of quantitative and semi-quantitative [(18)F]FDG-PET/CT indices for evaluating disease activity and management of patients with dermatomyositis and polymyositis. Front Med (Lausanne) 9:883727. https://doi.org/10.3389/fmed.2022.883727
Thogersen KF, Simonsen JA, Hvidsten S, Gerke O, Jacobsen S, Hoilund-Carlsen PF et al (2017) Quantitative 3D scintigraphy shows increased muscular uptake of pyrophosphate in idiopathic inflammatory myopathy. EJNMMI Res 7:97. https://doi.org/10.1186/s13550-017-0348-2
Diederichsen LP, Simonsen JA, Diederichsen AC, Kim WY, Hvidsten S, Hougaard M et al (2015) Cardiac abnormalities assessed by non-invasive techniques in patients with newly diagnosed idiopathic inflammatory myopathies. Clin Exp Rheumatol 33:706–714
Diederichsen LP, Simonsen JA, Diederichsen AC, Hvidsten S, Hougaard M, Junker P et al (2016) Cardiac abnormalities in adult patients with polymyositis or dermatomyositis as assessed by noninvasive modalities. Arthritis Care Res (Hoboken) 68:1012–1020. https://doi.org/10.1002/acr.22772
Blomberg BA, Thomassen A, Takx RA, Hildebrandt MG, Simonsen JA, Buch-Olsen KM et al (2014) Delayed (1)(8)F-fluorodeoxyglucose PET/CT imaging improves quantitation of atherosclerotic plaque inflammation: results from the CAMONA study. J Nucl Cardiol 21:588–597. https://doi.org/10.1007/s12350-014-9884-6
Rider LG, Giannini EH, Harris-Love M, Joe G, Isenberg D, Pilkington C et al (2003) Defining clinical improvement in adult and juvenile myositis. J Rheumatol 30:603–617
McHugh NJ, Tansley SL (2018) Autoantibodies in myositis. Nat Rev Rheumatol 14:290–302. https://doi.org/10.1038/nrrheum.2018.56
Rider LG, Werth VP, Huber AM, Alexanderson H, Rao AP, Ruperto N et al (2011) Measures of adult and juvenile dermatomyositis, polymyositis, and inclusion body myositis: Physician and Patient/Parent Global Activity, Manual Muscle Testing (MMT), Health Assessment Questionnaire (HAQ)/Childhood Health Assessment Questionnaire (C-HAQ), Childhood Myositis Assessment Scale (CMAS), Myositis Disease Activity Assessment Tool (MDAAT), Disease Activity Score (DAS), Short Form 36 (SF-36), Child Health Questionnaire (CHQ), physician global damage, Myositis Damage Index (MDI), Quantitative Muscle Testing (QMT), Myositis Functional Index-2 (FI-2), Myositis Activities Profile (MAP), Inclusion Body Myositis Functional Rating Scale (IBMFRS), Cutaneous Dermatomyositis Disease Area and Severity Index (CDASI), Cutaneous Assessment Tool (CAT), Dermatomyositis Skin Severity Index (DSSI), Skindex, and Dermatology Life Quality Index (DLQI). Arthritis Care Res (Hoboken) 63(Suppl 11):S118-157. https://doi.org/10.1002/acr.20532
Rider LG, Aggarwal R, Machado PM, Hogrel JY, Reed AM, Christopher-Stine L et al (2018) Update on outcome assessment in myositis. Nat Rev Rheumatol 14:303–318. https://doi.org/10.1038/nrrheum.2018.33
Buchpiguel CA, Roizemblatt S, Pastor EH, Hironaka FH, Cossermelli W (1996) Cardiac and skeletal muscle scintigraphy in dermato- and polymyositis: clinical implications. Eur J Nucl Med 23:199–203. https://doi.org/10.1007/BF01731845
Dewaraja YK, Frey EC, Sgouros G, Brill AB, Roberson P, Zanzonico PB et al (2012) MIRD pamphlet No. 23: quantitative SPECT for patient-specific 3-dimensional dosimetry in internal radionuclide therapy. J Nucl Med 53:1310–1325. https://doi.org/10.2967/jnumed.111.100123
Pipitone N (2016) Value of MRI in diagnostics and evaluation of myositis. Curr Opin Rheumatol 28:625–630. https://doi.org/10.1097/bor.0000000000000326
Tanaka S, Ikeda K, Uchiyama K, Iwamoto T, Sanayama Y, Okubo A et al (2013) [18F]FDG uptake in proximal muscles assessed by PET/CT reflects both global and local muscular inflammation and provides useful information in the management of patients with polymyositis/dermatomyositis. Rheumatology (Oxford) 52:1271–1278. https://doi.org/10.1093/rheumatology/ket112
Li Y, Zhou Y, Wang Q (2017) Multiple values of (18)F-FDG PET/CT in idiopathic inflammatory myopathy. Clin Rheumatol 36:2297–2305. https://doi.org/10.1007/s10067-017-3794-3
Motegi SI, Fujiwara C, Sekiguchi A, Hara K, Yamaguchi K, Maeno T et al (2019) Clinical value of (18) F-fluorodeoxyglucose positron emission tomography/computed tomography for interstitial lung disease and myositis in patients with dermatomyositis. J Dermatol 46:213–218. https://doi.org/10.1111/1346-8138.14758
Matuszak J, Blondet C, Hubele F, Gottenberg JE, Sibilia J, Bund C et al (2019) Muscle fluorodeoxyglucose uptake assessed by positron emission tomography-computed tomography as a biomarker of inflammatory myopathies disease activity. Rheumatology (Oxford) 58:2345–2346. https://doi.org/10.1093/rheumatology/kez040
Pipitone N, Versari A, Zuccoli G, Levrini G, Macchioni P, Bajocchi G et al (2012) 18F-Fluorodeoxyglucose positron emission tomography for the assessment of myositis: a case series. Clin Exp Rheumatol 30:570–573
Owada T, Maezawa R, Kurasawa K, Okada H, Arai S, Fukuda T (2012) Detection of inflammatory lesions by f-18 fluorodeoxyglucose positron emission tomography in patients with polymyositis and dermatomyositis. J Rheumatol 39:1659–1665. https://doi.org/10.3899/jrheum.111597
Sun L, Dong Y, Zhang N, Lv X, Chen Q, Wei W (2018) [(18)F]Fluorodeoxyglucose positron emission tomography/computed tomography for diagnosing polymyositis/dermatomyositis. Exp Ther Med 15:5023–5028. https://doi.org/10.3892/etm.2018.6066
Poulose KP, Reba RC, Eckelman WC, Goodyear M (1975) Extra-osseous localization of 99Tcm-Sn pyrophosphate. Br J Radiol 48:724–726. https://doi.org/10.1259/0007-1285-48-573-724
Bonte FJ, Parkey RW, Graham KD, Moore J, Stokely EM (1974) A new method for radionuclide imaging of myocardial infarcts. Radiology 110:473–474. https://doi.org/10.1148/110.2.473
Dewanjee MK, Kahn PC (1976) Mechanism of localization of 99mTc-labeled pyrophosphate and tetracycline in infarcted myocardium. J Nucl Med 17:639–646
Buja LM, Tofe AJ, Kulkarni PV, Mukherjee A, Parkey RW, Francis MD et al (1977) Sites and mechanisms of localization of technetium-99m phosphorus radiopharmaceuticals in acute myocardial infarcts and other tissues. J Clin Investig 60:724–740. https://doi.org/10.1172/jci108825
Bailey DL, Willowson KP (2013) An evidence-based review of quantitative SPECT imaging and potential clinical applications. J Nucl Med 54:83–89. https://doi.org/10.2967/jnumed.112.111476
Hess S, Blomberg BA, Zhu HJ, Hoilund-Carlsen PF, Alavi A (2014) The pivotal role of FDG-PET/CT in modern medicine. Acad Radiol 21:232–249. https://doi.org/10.1016/j.acra.2013.11.002
Yamashita H, Kubota K, Mimori A (2014) Clinical value of whole-body PET/CT in patients with active rheumatic diseases. Arthritis Res Ther 16:423
Alavi A, Hess S, Werner TJ, Hoilund-Carlsen PF (2020) An update on the unparalleled impact of FDG-PET imaging on the day-to-day practice of medicine with emphasis on management of infectious/inflammatory disorders. Eur J Nucl Med Mol Imaging 47:18–27. https://doi.org/10.1007/s00259-019-04490-6
Raynor WY, Jonnakuti VS, Zirakchian Zadeh M, Werner TJ, Cheng G, Zhuang H et al (2019) Comparison of methods of quantifying global synovial metabolic activity with FDG-PET/CT in rheumatoid arthritis. Int J Rheum Dis 22:2191–2198. https://doi.org/10.1111/1756-185x.13730
Tateyama M, Fujihara K, Misu T, Arai A, Kaneta T, Aoki M (2015) Clinical values of FDG PET in polymyositis and dermatomyositis syndromes: imaging of skeletal muscle inflammation. BMJ Open 5:e006763. https://doi.org/10.1136/bmjopen-2014-006763
Bai X, Tie N, Wang X, Zhao J (2017) Intense muscle activity due to polymyositis incidentally detected in a patient evaluated for possible malignancy by FDG PET/CT imaging. Clin Nucl Med 42:647–648. https://doi.org/10.1097/rlu.0000000000001727
Al-Nahhas A, Jawad AS (2011) PET/CT imaging in inflammatory myopathies. Ann N Y Acad Sci 1228:39–45. https://doi.org/10.1111/j.1749-6632.2011.06016.x
McKenney-Drake ML, Moghbel MC, Paydary K, Alloosh M, Houshmand S, Moe S et al (2018) (18)F-NaF and (18)F-FDG as molecular probes in the evaluation of atherosclerosis. Eur J Nucl Med Mol Imaging 45:2190–2200. https://doi.org/10.1007/s00259-018-4078-0
Mayer M, Borja AJ, Hancin EC, Auslander T, Revheim ME, Moghbel MC et al (2020) Imaging atherosclerosis by PET, with emphasis on the role of FDG and NaF as potential biomarkers for this disorder. Front Physiol 11:511391. https://doi.org/10.3389/fphys.2020.511391
Høilund-Carlsen PF, Moghbel MC, Gerke O, Alavi A (2019) Evolving role of PET in detecting and characterizing atherosclerosis. PET Clin 14:197–209. https://doi.org/10.1016/j.cpet.2018.12.001
Han JH, Lim SY, Lee MS, Lee WW (2015) Sodium [(1)(8)F]fluoride PET/CT in myocardial infarction. Mol Imaging Biol 17:214–221. https://doi.org/10.1007/s11307-014-0796-2
Høilund-Carlsen PF, Sturek M, Alavi A, Gerke O (2020) Atherosclerosis imaging with (18)F-sodium fluoride PET: state-of-the-art review. Eur J Nucl Med Mol Imaging 47:1538–1551. https://doi.org/10.1007/s00259-019-04603-1
Piri R, Lici G, Riyahimanesh P, Gerke O, Alavi A, Høilund-Carlsen PF (2021) Two-year change in 18F-sodium fluoride uptake in major arteries of healthy subjects and angina pectoris patients. Int J Cardiovasc Imaging 37:3115–3126. https://doi.org/10.1007/s10554-021-02263-7
Acknowledgements
The skilled technical assistance of medical laboratory technician Lene Bøtker is highly appreciated. We also wish to thank the Danish Myositis Patient Group.
Funding
This work was supported by the Danish Rheumatism Association Grant Number R87-A1497.
Author information
Authors and Affiliations
Contributions
LPD, SH, and JAS designed the study. KFT, SH, LPD, and JAS were involved in collecting data. SH, OG, and JAS performed data analysis. All authors were actively involved in the conception of the study, in interpreting data, and in drafting or revising the manuscript, and all read and approved the final manuscript submitted. All authors agree to be accountable for all aspects of the work. KFT was the driving force in defining volumes of interest as JAS was in data handling. Therefore, we propose that these two share the first authorship.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants gave written informed consent. All procedures performed were following the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments, and the study was carried out with the approval of the Scientific Ethics Committee of The Region of Southern Denmark (no. S-20100022).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table.
Clinical characteristics of patients with idiopathic inflammatory myopathy and control persons.
Additional file 2: Figure.
Examples of FDG uptake in healthy control persons.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Simonsen, J.A., Thøgersen, K.F., Hvidsten, S. et al. Treatment-naïve idiopathic inflammatory myopathy: disease evaluation by fluorodeoxyglucose versus pyrophosphate. Egypt J Radiol Nucl Med 53, 150 (2022). https://doi.org/10.1186/s43055-022-00822-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00822-z