
Abstract
Background
Aortic arch and vertebral artery anomalies are vascular variations that occur as a result of embryological developmental defects. Bicarotid trunk anomaly is a rare aortic arch anomaly and refers to a common single trunk origin of common carotid arteries. VA origin anomalies are mostly unilateral and the most common is the LVA originating from the aortic arch. Abnormal origin of the RVA from the RCCA is a rare vascular anomaly. In this case, we presented ARSA and bicarotid trunk anomaly with abnormal origin of the vertebral arteries.
Case presentation
A 64-year-old male was admitted to our center with complaints of chronic headache and dizziness. In addition to ARSA and bicarotid trunk anomaly, RVA originating from RCCA and LVA originating from aortic arch were observed in CT angiography. The origin of LVA was between the bicarotid trunk and LSCA. Both VA were entering the transverse foramen at the level of the C6 vertebra. These anomalies were also revealed in detail by MR angiography of head/neck.
Conclusion
Aortic arch anomalies are a group with different subtypes. Awareness of VA origin anomalies is important for planning surgical and endovascular interventional procedures.
Similar content being viewed by others


Background
The aortic arch normally contains three main branches. These are the brachiocephalic trunk (BCT), the left common carotid artery (LCCA) and the left subclavian artery (LSCA), respectively. The right subclavian artery (RSCA) and the right common carotid artery (RCCA) branch from the BCT. Bicarotid trunk anomaly is a rare aortic arch anomaly and refers to a common single trunk origin of common carotid arteries. Normally the vertebral artery (VA) originates from the proximal of the subclavian artery and is its first branch and is important in the vascular supply of the brainstem and cerebellum. VA origin anomalies are mostly unilateral and the most common is the left vertebral artery (LVA) originating from the aortic arch. Although bilateral cases have been reported, they are extremely rare [1, 2]. Abnormal origin of the right vertebral artery (RVA) from the RCCA is a rare vascular anomaly. Although there are various data in the literature, its incidence is not clearly known. Abnormal VA origin variations are detected incidentally in most of the cases. Identifying these anomalies is important for preoperative preparation of vascular surgery and guiding endovascular approaches [3, 4]. Abnormal origin of the right VA from the RCCA is generally seen with aberrant right subclavian artery (ARSA) variation [5]. In this case, we presented ARSA and bicarotid trunk anomaly with abnormal origin of the vertebral arteries.
Case presentation
A 64-year-old male was admitted to our center with complaints of chronic headache and dizziness. There was no known medical history other than hypertension. No abnormalities were detected in routine examinations and computed tomography (CT) angiography of head/neck was performed to exclude cerebrovascular pathology. In addition to ARSA and bicarotid trunk anomaly, RVA originating from RCCA and LVA originating from aortic arch were observed in CT angiography. The origin of LVA was between the bicarotid trunk and LSCA. Both VA were entering the transverse foramen at the level of the C6 vertebra (Fig. 1). These anomalies were also revealed in detail by magnetic resonance (MR) angiography of head/neck (Fig. 2). Intracranial vascular or parenchymal pathology was not observed. The patient whose complaints regressed with symptomatic treatment was discharged.

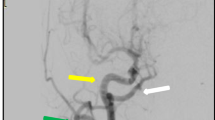
a Computed tomography angiography image shows the aberrant right subclavian artery originating as the last branch of the aortic arch and showing retroesophageal course (arrow). b Bicarotid trunk (arrow), ARSA (blank arrow), RCCA originated RVA (arrowhead) and aortic arch origin LVA (blank arrowhead) are seen in 3D reconstruction images. LSCA exits from the proximal of the ARSA (curved arrow). c Maximum intensity projection of computed tomography angiography image shows that both vertebral arteries enter the transverse foramen at the C6 vertebral level (arrows). C7 vertebra is shown with blank arrows

a Magnetic resonance angiography image shows the aberrant right subclavian artery originating as the last branch of the aortic arch (arrow). b Bicarotid trunk (arrow), ARSA (blank arrow), RCCA originated RVA (white arrowhead), aortic arch origin LVA (black arrowhead) and LSCA (curved arrow) are seen in 3D reconstruction images
Discussion
During embryogenesis, the aortic arch and its branches begin to develop in the first weeks of fetal life and take its final shape in the eighth week. Aortic arch anomalies occur in embryological defects. The majority of aortic arch anomalies are detected incidentally. In about 80% of people, three branches arise from the aortic arch. These are BCT, LCCA and LSCA, respectively. The most common aortic arch anomaly is the bovine-type arch in which RSCA, RCCA and LCCA originate from a single trunk. This is followed by LVA originating independently from the aortic arch [6]. ARSA is an anomaly in which the RSCA originates as the last branch of the aortic arch and usually shows an aberrant course from the posterior of the trachea and esophagus, and its incidence is less than 1%. This aortic arch anomaly is due to interruption of the fourth right aortic arch between the notches for the common carotid artery (CCA) and RSCA. Although ARSA is mostly asymptomatic, dysphagia secondary to esophageal compression can be seen in patients with retroesophageal course, and this is called dysphagia lusoria. Respiratory symptoms may accompany in ARSA anomaly passing between trachea and esophagus. The bicarotid trunk is a very rare aortic arch anomaly with an incidence less than 0.1% and occurs when the third aortic arches persist as common bicarotid trunk during embryogenesis. In this anomaly, carotid arteries originate from a common trunk [7].
Vertebral arteries normally originate from the posterosuperior of the proximal segment of the subclavian artery and enter the transverse foramen at the C6 level and run towards the foramen magnum. Embryologically, the vertebral and subclavian arteries arise from the seven intersegmental arteries that arise from the dorsal aorta. While the first six intersegmental arteries degenerate, vertebral and subclavian arteries develop from the 7th intersegmental artery. If the first six intersegmnetal arteries do not regress, anatomical variants may occur. If the first two intersegmental arteries continue, an abnormal supply of VA occurs from the internal or external carotid artery. If a 3rd to 6th intersegmental artery becomes permanent, the VA originates from the CCA or aorta [8, 9]. VA origin anomalies are usually unilateral and are more common on the left side. The most common anomaly is LVA in the aortic arch, which exits between LCCA and LSCA [1, 2, 10]. RVA origin anomaly is less common. Although the incidence of RVA anomaly originating from RCCA has been defined in some angiography studies, it is not clearly known [4, 11].
In the study of Lazaridis et al. the most common RVA origin anomaly was reported as RVA originating from RCCA, and its incidence among all anomalies is less than 0.5%. Again, in this review, the incidence of bilateral VA origin anomaly was reported very rarely with 0.048% and two LVA anomalies have been reported with the bicarotid trunk, and their ratio among all anomalies is approximately 0.015%. In this study, although the schematic figure similar to our case was named RV.LA3.ARSCA, the number of cases was not mentioned [1].
Vertebral arteries normally enter the transverse foramen at the level of the C6 vertebra. According to the literature, when the LVA originates from the aortic arch, it enters the foramen at the C3, C4 or C5 level instead of the C6 vertebra level. In RVA origin anomalies, a difference can be seen at the entrance level of the transverse foramen [2, 12]. In our case, although both VA had an anomaly of origin, both VA entered the transverse foramina at the C6 vertebra level.
We presented a case in which bicarotid trunk, ARSA, LVA originating from the aortic arch and RVA anomaly originating from RCCA were seen together. VA origin anomalies are usually asymptomatic and detected incidentally, as in our case. However, knowing these vascular anomalies is very important for planning endovascular or surgical procedures. Particularly in cases undergoing carotid artery stenting, it is vital to know the carotid artery originated VA anomalies.
Conclusions
Aortic arch anomalies are a group with different subtypes. ARSA can be seen with different aortic arch anomalies. Although VA anomalies are more frequently seen unilaterally, they can rarely be seen bilaterally. Awareness of VA origin anomalies is important for planning surgical and endovascular interventional procedures.
Availability of data and materials
For this type of study formal consent is not required.
Code availability
For this type of study formal consent is not required.
Abbreviations
- BCT:
-
Brachiocephalic trunk
- CCA:
-
Common carotid artery
- RCCA:
-
Right common carotid artery
- LCCA:
-
Left common carotid artery
- LSCA:
-
Left subclavian artery
- RSCA:
-
Right subclavian artery
- VA:
-
Vertebral artery
- RVA:
-
Right vertebral artery
- LVA:
-
Left vertebral artery
- ARSA:
-
Aberrant right subclavian artery
- CT:
-
Computed tomography
- MR:
-
Magnetic resonance
References
Lazaridis N, Piagkou M, Loukas M, Piperaki E-T, Totlis T, Noussios G et al (2018) A systematic classification of the vertebral artery variable origin: clinical and surgical implications. Surg Radiol Anat 40(7):779–797
Yuan S-M (2016) Aberrant origin of vertebral artery and its clinical implications. Braz J Cardiovasc Surg 31(1):52–59
Ali A, Roman NIS, Cox M, Kung D, Choudhri O, Hurst RW et al (2018) Anomalous origin of the right vertebral artery from the right common carotid artery. Cureus. 10(11):e3602
Ishikawa K, Yamanouchi T, Mamiya T, Shimato S, Nishizawa T, Kato K (2018) Independent anomalous origin of the right vertebral artery from the right common carotid artery. J Vasc Interv Neurol 10(2):25
Chen C-J, Wang L-J, Wong Y-C (1998) Abnormal origin of the vertebral artery from the common carotid artery. Am J Neuroradiol 19(8):1414–1416
Celikyay ZRY, Koner AE, Celikyay F, Denız C, Acu B, Firat MM (2013) Frequency and imaging findings of variations in human aortic arch anatomy based on multidetector computed tomography data. Clin Imaging 37(6):1011–1019
Hanžič N, Čizmarević U, Lesjak V, Caf P (2019) Aberrant right subclavian artery with a Bicarotid trunk: the importance of diagnosing this rare incidental anomaly. Cureus 11(11):e6094
Vitošević F, Vitošević Z, Rasulić L (2020) The right vertebral artery arising from the right common carotid artery: report of a rare case. Surg Radiol Anat 42:1263–1266
Kesler WW, Sabat SB (2018) Isolated anomalous origin of the vertebral artery from the common carotid artery. Interact Cardiovasc Thorac Surg 27(4):615–616
Kim Y-D, Yeo H-T, Cho Y-D (2009) Anomalous variations of the origin and course of vertebral arteries in patients with retroesophageal right subclavian artery. J Korean Neurosurg Soc 45(5):297
Palmer F (1977) Origin of the right vertebral artery from the right common carotid artery: angiographic demonstration of three cases. Br J Radiol 50(591):185–187
Woraputtaporn W, Ananteerakul T, Iamsaard S, Namking M (2019) Incidence of vertebral artery of aortic arch origin, its level of entry into transverse foramen, length, diameter and clinical significance. Anat Sci Int 94(4):275–279
Acknowledgements
Not applicable.
Funding
This study was not supported by any funding.
Author information
Authors and Affiliations
Contributions
ÖFT: Manuscript writing/editing. HC: manuscript writing/editing. AK: manuscript editing. HÖ: manuscript editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
For this type of study formal consent is not required.
Consent for publication
For this type of study formal consent is not required.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Topaloğlu, Ö.F., Cebeci, H., Kılınçer, A. et al. Abnormal origin of the vertebral arteries with Bicarotid trunk: a case report. Egypt J Radiol Nucl Med 53, 95 (2022). https://doi.org/10.1186/s43055-022-00773-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00773-5