
Abstract
Background
Leydig cell tumors (LCTs) represent the most common form of stromal tumors. We reported the 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) findings of a patient with testicular LCT.
Case presentation
A 50-year-old man with a history of end-stage renal disease and renal transplantation 19 years ago. One year earlier, he started to have a chronic rejection. During the investigation to determine the cause of chronic rejection, a suspicious lesion in the graft with a collection around it was seen on ultrasound (US) images, raising the possibility of post-transplant lymphoproliferative disorder (PTLD). The patient was referred for further evaluation by whole body 18F-FDG PET/CT imaging. The image finding revealed an incidental hypermetabolic focal lesion in the right testicle—no other specific findings in the remaining parts of the body nor definitive FDG avid lymphadenopathy to suggest PTLD. Testicular US was requested and showed a well-defined right-sided heterogeneous hypoechoic intratesticular focal mass at the upper pole of the right testis with significant internal vascularity on the color Doppler imaging. The patient underwent a right radical orchidectomy, and the tumor was pathologically confirmed as an LCT.
Conclusion
In our case, 18F-FDG-PET/CT has been helpful in incidentally detecting this rare testicular tumor in a patient with suspected PTLD.
Similar content being viewed by others


Background
Although LCTs are rare, it is considered the most frequent non-germ cell tumors of the testis, accounting for 1–3% of all adult testicular tumors and 0.4–9% of prepubescent testicular tumors [1, 2]. LCTs are usually unilateral. In most cases, they originate from testicular Leydig cells, but rarely they may arise from the epididymis [3]. A small percentage of LCTs are malignant and have a poor metastatic prognosis since they react poorly to chemotherapy and radiation treatment [1]. Adults may have unusual symptoms associated with testicular tumors and endocrine problems or may remain entirely asymptomatic and be detected accidentally by ultrasonography (US) [4].
The US has shown high sensitivity in identifying testicular abnormalities among all imaging modalities and is considered the gold standard technique for evaluating the testes. However, relying only on gray-scale and color Doppler information is inadequate to describe lesions, particularly small lesions, in which LCTs and seminomas may be quite similar [5, 6]. LCTs usually exhibit a homogenous hypoechoic appearance in the testicular US imaging. Heterogeneity may be indicative of aggressive behavior [7].
The use of 18F-FDG PET/CT may not assist in distinguishing between benign and malignant testicular tumors, but it is helpful in managing and monitoring an LCT patient. FDG PET/CT has a very high negative predictive value in FDG-avid testicular tumors, but its positive predictive value varies across studies [8]. FDG PET/CT findings of LCTs have been reported in few studies [9, 10]. The present clinical case report described the 18F-FDG PET/CT findings of testicular LCT detected during imaging of a patient with the possibility of post-transplant lymphoproliferative disorder (PTLD).
Case presentation
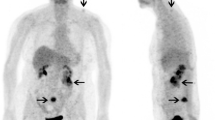
A 50-year-old man with a history of end-stage renal disease and renal transplantation 19 years ago. One year earlier, he went into chronic rejection and started on hemodialysis. During the investigation by the nephrology team to determine the cause of chronic rejection, a suspicious lesion in the graft with a surrounding collection was clear on the US examination, raising the possibility of PTLD. The nephrology team referred the patient for further evaluation by 18F-FDG PET/CT examination. The 18F-DG PET/CT was done and revealed an incidental finding of focal increase right testicular uptake with more metabolic activity (SUVmax = 2.9) in relation to the remaining testicular tissues (Fig. 1). No specific findings in other areas nor definitive FDG avid lymphadenopathy to suggest PTLD. The testicular US was requested and showed a corresponding focal mass at the upper pole of the right testicle (Fig. 2a) with significant internal vascularity on color Doppler imaging (Fig. 2b). During that time, the patient showed no testicular swelling, testicular pain, weight loss, or a decrease in appetite. The patient was referred to the urology department and underwent a right radical orchidectomy. A right inguinal incision was made, the spermatic cord was exposed and dissected, which was normal looking, and then ligation of the vas deferens and vessels was done at the internal inguinal ring. The right testis was exposed and looked normal in size and contour compared to the left one. The right epididymis looked unremarkable. The testis was then dissected and delivered with the cord included in the tunica. Homeostasis was maintained. After the operation, the patient did well with no complaints. He is currently under active surveillance.

a–c FDG PET/CT images demonstrate incidental finding of focal increase right testicular uptake seen with more metabolic activity in relation to the remaining testicular tissues (SUVmax 2.9). No specific findings in other areas or definitive FDG avid lymphadenopathy

a Testicular US shows a well-circumscribed, encapsulated mass at the upper pole of the right testicle, measures 1.1 x 1.1 cm. b Color Doppler image shows significant internal vascularity of mass
An orchidectomy specimen with the attached spermatic cord was sent for histopathology. The specimen revealed a 1 × 1 × 1 cm well-defined mass on serial cut sections. The surface was homogenous tan (Fig. 3). The tumor displayed a diffuse pattern of large polygonal cells with round nuclei, profuse eosinophilic cytoplasm, and prominent nucleoli (Fig. 4a). No definite Reinke crystals were identified. There was no evidence of tumor necrosis, nuclear pleomorphism, increased mitosis, or vascular invasion. The Ki67 proliferative index was low, with 1–2% (Fig. 4b). The tumor cells were diffusely positive for vimentin, inhibin, and calretinin and focally positive for Mart-1 (Figs. 4c–f). The spermatic cord showed benign adrenal rest and Leydig cell hyperplasia. The findings were consistent with benign LCT.

An orchidectomy specimen was received with an attached spermatic cord, revealing a 1 × 1 × 1 cm, well-defined mass on serial cut sections. The surface is tan homogenous in an unremarkable testicular background

a Light microscopic examination of the tumor shows a diffuse pattern of large polygonal cells with abundant eosinophilic cytoplasm, round nuclei, and prominent nucleoli. No definite Reinke crystals were identified. There is no evidence of tumor necrosis, nuclear pleomorphism, increase mitosis, or vascular invasion. b The Ki67 proliferative index is low with 1–2%. c The tumor cells are diffusely positive for inhibin. d The tumor cells are diffusely positive for vimentin. e The tumor cells are diffusely positive for calretinin. f The tumor cells are focally positive for Mart-1. The spermatic cord shows benign adrenal rest and Leydig cell hyperplasia. The diagnosis was consistent with benign LCT
Discussion
PET/CT has been widely used to identify and discriminate benign and malignant tumors in various organs [11, 12]; however, a few papers have been published on its application to detect testicular lesions and assess the functional status of testes [13]. Our case illustrated the 18F-FDG PET/CT findings of an LCT in a 50-year-old male patient who had a renal transplant 19 years ago. The 18F-FDG PET/CT demonstrated an incidental finding of focal increase right testicular uptake with more metabolic activity in relation to the remaining testicular tissues (SUVmax = 2.9).
A few studies have addressed the PET/CT imaging of LCT using 18F-FDG. One of these case studies was a 43-year-old man submitted to whole-body 18F-FDG PET/CT imaging for healthcare screening. The 18F-FDG PET/CT imaging showed a focal hypermetabolic lesion in the right testis. The tumor was pathologically verified as LCT [9]. Another case of a 50-year-old man with lymphoma was described, in which increased 18F-FDG uptake was noted in a right testicular lesion. After right radical orchidectomy, a benign LCT was histopathologically proved [10].
SUVmax is a semi-quantitative biomarker with a particular clinical reference value for benign and malignant tumor distinction [14, 15]. Many factors affecting testicular SUV such as age, testicular volume, and sexual activity [16]. Discrepancies in normal SUVs may exist because of differences in patient demographics and PET technology [17]. A study included 203 men showed that the normal SUV ranges between 1.23 and 3.85 with a mean value of 2.44 [18]. Shoe et al. [19] discovered statistically significant variations in SUVmax values for benign and malignant testicular tumors. SUVmax of 3.75 was found to be the optimal cutoff value for distinguishing malignant from benign testicular lesions; this value has a sensitivity of 90.6% and a specificity of 80.9%. In our study, the right testis showed more focal uptake than the left one (SUVmax = 2.9). The left testis was seen with unified, homogeneous uptake, and the SUVmax was in the normal range (SUVmax = 2.0).
In our case, testicular uptake of FDG prompted a medical referral to a urologist consultation and scrotal US. The US was done and demonstrate a well-defined heterogeneous hypoechoic focal mass at the upper pole of the right testicle with significant internal vascularity on color Doppler imaging, which corresponding to the focal hypermetabolic lesion in the right testicle on 18F-FDG PET/CT imaging. However, neither intratumoral calcification nor testicular microlithiasis was observed in US images. A review of one article describing the US findings of testicular LCTs shows that 90% of the cases are homogeneous hypoechoic, and 88% have a distinctive pattern of increased peripheral blood flow [20].
Conclusion
In our case, 18F-FDG-PET/CT was valuable in incidentally detecting this uncommon testicular tumor in a patient with suspected PTLD. Further researches are required to determine the mechanism of FDG uptake and the role of FDG PET/CT in this tumor type.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CT:
-
Computed tomography
- FDG:
-
Fluorodeoxyglucose
- LCTs:
-
Leydig cell tumors
- PET:
-
Positron emission tomography
- PTLD:
-
Posttransplant lymphoproliferative disorder
- SUV:
-
Standardized uptake value
- US:
-
Ultrasound
References
Idrees MT, Ulbright TM, Oliva E et al (2017) The World Health Organization 2016 classification of testicular non germ cell tumours: a review and update from the International Society of Urological Pathology Testis consultation panel. Histopathology 70:513–521
Gheorghisan-Galateanu AA (2014) Leydig cell tumors of the testis: a case report. BMC Res Notes 7:656
Giacaglia LR, Kohek MBF, Carvalho FM, Fragoso MC, Mendonca B, Latronico AC (2000) No evidence of somatic activating mutations on gonadotropin receptor genes in sex cord stromal tumors. Fertil Steril. 74:992–995
Zhu J, Luan Y, Li H (2018) Management of testicular Leydig cell tumor: a case report. Medicine 97:e11158
Dogra VS, Gottlieb RH, Oka M et al (2003) Sonography of the scrotum. Radiology 227:18–36
Yagil Y, Naroditsky I, Milhem J et al (2010) Role of Doppler ultrasonography in the triage of acute scrotum in the emergency department. J Ultrasound Med 29:11–21
Maxwell F, Izard V, Ferlicot S et al (2016) Colour Doppler and ultrasound characteristics of testicular Leydig cell tumours. Br J Radiol 89:20160089
Calabrò D, Telo S, Ambrosini V (2020) PET imaging in testicular tumours. Curr Opin Urol 30:665–671
Lee G, Lee JH, Lee WA (2010) F-18 FDG PET/CT imaging of a Leydig cell tumor. Clin Nucl Med 35:202–204
Van Der Gucht A, Maged Z, Burruni R, Barras JL, Schaefer N (2018) Testicular Estrogen-secreting leydig cell tumor in 18F-FDG PET/CT: an incidental detection in a patient treated by chemotherapy for Hodgkin Lymphoma. Clin Nucl Med 43:41–43
Xia Q, Feng Y, Wu C et al (2015) Differentiation between malignant and benign solitary lesions in the liver with 18FDG PET/CT: accuracy of age-related diagnostic standard. J Cancer 6:40–47
Wang SY, Wang SX, Liao JQ, Chen G (2016) 18F-FDG PET/CT and contrast-enhanced CT of primary malignant tracheal tumor. Clin Nucl Med 41:595–605
Bochiński A, Sujenthiran A, Al-Hussini M, Fruhwirth GO, Shabbir M, Yap T (2021) 18F-FDG PET/CT use in functional assessment of the testes: a systematic review. Andrology 9:1410–1421
Ali I, Johns W, Bottger B, Gupta SM (2007) Serendipitous detection of testicular seminoma on F-18 FDG positron tomography. ClinNucl Med 32:201–202
Buchler T, Simonova K, Fencl P, Jarkovsky J, Abrahamova J (2012) Clinical outcomes of patients with nonseminomatous germ cell tumours and negative postchemotherapy positron emission tomography. Cancer Invest 30:487–492
Moon SH, Eo JS, Lee JJ, Chung JK, Lee DS, Lee MC (2011) 18 F-FDG uptake of human testis on PET/CT: correlation with age, sex hormones, and vasectomy. Nucl Med Mol Imaging 45:291–298
Harper L, Simmons C, Nathan M, Thanarajasingam G, Kim H, Young J (2021) Establishing normal testicular 18F-FDG PET/CT SUVs. Am J Roentgenol 216:1634–1640
Cathomas R, Klingbiel D, Bernard B et al (2018) Questioning the value of fluorodeoxyglucose positron emission tomography for residual lesions after chemotherapy for metastatic seminoma: results of an International Global Germ Cell Cancer Group Registry. J Clin Oncol 36:3381–3387
Shao D, Gao Q, Tian XW, Wang SY, Liang CH, Wang SX (2017) Differentiation and diagnosis of benign and malignant testicular lesions using 18F-FDG PET/CT. Euro j radiol 93:114–120
Maizlin ZV, Belenky A, Kunichezky M, Sandbank J, Strauss S (2004) Leydig cell tumors of the testis: gray scale and color Doppler sonographic appearance. J Ultrasound Med 23:959–964
Acknowledgements
The author expresses his great gratitude to King Fahd Specialist Hospital in Dammam, Saudi Arabia. Also, the author is particularly very grateful to Dr. Yassir Assiri, Dr. Muhannad Alnami, and Mr.Vipin Jayakrishnan for their collaboration.
Funding
The author declares that this work has not received any funding.
Author information
Authors and Affiliations
Contributions
Author read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Institutional review board’s approval was obtained. Written informed consent was obtained from the patient.
Consent for publication
Not applicable
Informed consent
Written informed consent was obtained.
Competing interests
The authors of this case report declare no relevant conflicts of interest, and no relationships with any companies, whose products or services may be related to the subject matter of the article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yassir, A. Leydig cell tumor of the testis: an incidental finding at 18F-FDG PET/CT imaging. Egypt J Radiol Nucl Med 52, 266 (2021). https://doi.org/10.1186/s43055-021-00646-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00646-3