
Abstract
Background
The gold standard for verifying COVID-19 mostly depends on microbiological tests like real-time polymerase chain reaction (RT-PCR). However, the availability of RT-PCR kits can be known as a problem and false negative results may be encountered. Although CT scan is not a screening tool for the diagnosis of COVID-19 pneumonia, given the widespread acquisition of it in the pandemic state, familiarity with different CT findings and possible differential diagnosis is essential in this regard.
Main text
In this review, we introduced the typical and atypical CT features of COVID-19 pneumonia, and discussed the main differential diagnosis of COVID-19 pneumonia.
Conclusions
The imaging findings in this viral pneumonia showed a broad spectrum, and there are no pathognomonic imaging findings for COVID-19 pneumonia. Although CT scan is not a diagnostic and screening tool, familiarity with different imaging findings and their differential diagnosis can be helpful in a rapid and accurate decision-making.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
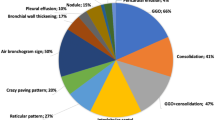
In December 2019, a series of pneumonia cases emerged in Wuhan, China. Thereafter, the disease rapidly spread worldwide. Accordingly, based on WHO declaration, it became pandemic on March 11, 2020. The gold-standard test for COVID-19 diagnosis is real-time reverse transcription–polymerase-chain-reaction (RRT-PCR). Although imaging is not considered as a diagnostic tool for COVID-19 and most radiology professional organizations and societies unanimously disagree with performing screening computed tomography (CT) for the identification of COVID-19, a large number of chest computed tomography (CT) scans have been done worldwide to assess the severity and extension of the lower respiratory tract involvement [1]. Therefore, radiologists should be more familiar with CT scan findings of COVID-19 pneumonia and its differential diagnosis. Typical imaging features are those frequently seen, which are more specific for COVID-19 pneumonia on the basis of the literature review in the current pandemic [2]. These findings include peripheral bilateral ground glass opacities (GGO) with or without consolidation or crazy-paving pattern, reverse halo sign or other findings related to organizing pneumonia (OP), and multifocal GGO of the rounded morphology with or without consolidation or visible intralobular lines (crazy-paving). However, this viral pneumonia showed imaging findings which are less specific for COVID-19 pneumonia or uncommonly reported; these findings can be classified as indeterminate or atypical findings. Correspondingly, they include diffuse GGO with no clear distribution, isolated lobar or segmental consolidation with no GGO, discrete small nodules (centrilobular, “tree in-bud”), lung cavitation, and smooth interlobular septal thickening with pleural effusion [3].
The Dutch radiological society developed a categorical CT scheme-CORADS-to assess the suspicion for pulmonary involvement of COVID-19 based on features seen at unenhanced chest CT. It ranges from CO-RADS category 1 with very low level of suspicion to CO-RADS category 5 with very high level of suspicion. If none of five categories can be assigned secondary to incomplete or insufficient images, its considered as CO-RADS category0. CO-RADS category 6 indicates proven COVID-19 by positive RT-PCR test results (Table 1) [4].
Moreover, there is a semi-quantitative scoring system for quantitatively estimating parenchymal abnormality on the basis of the area involved. Each one of the five lung lobes was individually evaluated and weighted based on parenchymal involvement scored on a scale ranged from 0 to 5, with 0 indicating no involvement, 1 indicating less than 5% involvement, 2 indicating 5–25% involvement, 3 indicating 26–49% involvement, 4 indicating 50–75% involvement, and 5 indicating more than 75% involvement. The total CT score was the sum of the individuals’ lobar scores, which was ranged from 0 (no involvement) to 25 (the maximum involvement) (Fig. 1) [5]. In this review, we introduced different CT features of COVID-19 pneumonia and discussed the main differential diagnosis. Recognition of these features could help radiologists to have a rapid and accurate diagnosis.

COVID-19 pneumonia: thin section CT shows bilateral multifocal subpleural and peribronchial GGO, semiqutitative score:18
Henceforth, each one of the imaging feature of COVID-19 pneumonia with RT-PCR is described, as confirmed at our referral hospital for COVID-19 pneumonia. Images illustrated in differential diagnosis were extracted from the images’ archive of the Department of Radiology.
Main text
Typical findings
Peripheral ground-glass opacities
On HRCT, GGO refers to the area of the increased lung opacity in which underlying bronchovascular markings are not obscured [6].
GGO is the most common manifestation (40–83%) of COVID-19 pneumonia. Right and left lower lobes are most commonly involved. Multilobar subpleural GGO is seen in most cases. However, COVID-19 pneumonia may manifest as unilateral GGO even before the onset of symptoms with rapid evolution into diffuse, bilateral disease [7] (Fig. 2).

COVID-19 pneumonia: thin section CT shows bilateral subpleural GGO and septal thickening
Differential diagnosis of GGO in the thin section CT was shown to be correlated with the clinical setting. In an acute setting, clinical history is more important than the distribution of GGO; however, in a chronic setting, its distribution is helpful in narrowing down the differential diagnosis. Notably, in patients with acute symptoms, some entities with peripheral distribution such as diffuse alveolar damage [6] (Fig. 3), simple pulmonary eosinophilia (Loffler syndrome) [8] (Fig. 4), and some viral pneumonia like influenza A have been described [9] (Fig. 5).

Diffuse alveolar damage: thin section CT shows patchy areas of GGO and consolidation in the lung periphery in upper lobes

Simple pulmonary eosinophilia: thin section CT shows consolidation and GGO involving mainly the peripheral regions of both upper lobes

Influenza A viral infection: thin section CT shows subpleural GGO in left lower lobe
In some patients with ground-glass opacity on HRCT, superimposition of a reticular pattern resulted in crazy paving appearance. This pattern was initially recognized in patients with pulmonary alveolar proteinosis (PAP) (Fig. 6), and it may also be seen in other differential diagnoses of GGO [10].

Pulmonary alveolar proteinosis: thin section CT shows bilateral GGO and reticulation (crazy-paving appearance)
Some recent studies have also reported the crazy paving pattern in 5–36% of patients with COVID-19 pneumonia [11]. This appearance can be considered as an indicator of disease progress or it may be recognized as secondary to the peak stage of COVID-19 pneumonia (Fig. 7) [5].

COVID-19 pneumonia: thin section CT shows bilateral multifocal subpleural and peribronchial GGO and reticulation (crazy -paving appearance)
Reverse halo appearance
Reverse halo sign, also known as the Atoll sign, can be defined as a round or ovoid GGO surrounded by the complete or crescent ring of consolidation [6].
This sign has been reported in several COVID-19 cases (Fig. 8). Moreover, it is assumed to be secondary to disease progression, which can consequently result in the development of consolidation around GGO or lesion absorption with the consequent decreased central density [12].

COVID-19 pneumonia: thin section CT shows multifocal peripheral GGO, with reverse halo appearance
Initially, the presence of reverse halo sign was believed to be specific for OP, but its differential diagnosis has broadened, such that we can remember it with mnemonic VISCERAL: Vasculitis, Infection, Sarcoidosis, Cryptogenic organizing pneumonia, Emboli, Radiation, and radioablation, Adenocarcinoma and Lymphomatoid granulomatosis. From non-infective processes, one important differential diagnosis that must be kept in mind is pulmonary infarction; in the patients with appropriate clinical history and laboratory data, in the presence of reverse halo sign on the non-contrast CT scan, the prompt evaluation of pulmonary vasculature, in contrast-enhanced CT with pulmonary thromboembolism(PTE) protocol, is essential (Fig. 9) [13, 14].

Pulmonary embolism: thin section CT in axial plane in lung window shows subpleural consolidation with reverse halo sign(RHS), coronal image in mediastinal window show filling defect in lower lobes pulmonary arteries suggestive for pulmonary embolism
In the infective process, this appearance is not specific. In immunocompromised patients, when there is a suspected fungal infection, the reverse halo sign is more frequently expected in mucormycosis than in invasive pulmonary Aspergillus [15] (Fig. 10). Additionally, in active tuberculosis, the Atoll sign can be expected, but it shows a nodular appearance [16].

Pulmonary zygomycosis: thin section CT shows multiple nodules with reversed halo sign (RHS) in the right upper and lower lobes
Findings of organizing pneumonia
OP is an inflammatory non-infectious abnormality, which can be idiopathic (cryptogenic OP) or secondary to the connective tissue disease, drug toxicity, infection, toxic inhalation, immunologic disorders, and graft versus host disease (GVHD). The most typical findings of the high-resolution computed tomography (HRCT) of OP include nodular or mass-like consolidation with peribronchovascular and subpleural predominance. The findings show more severity in the lower lobes [6]. Based on an expert panel review published in MARCH 2020, the most common reported CT findings in COVID-19 pneumonia are secondary to lung injury with organizing pneumonia pattern [17, 18] (Fig. 11). One finding that is highly suggestive of OP is the Atoll sign or reversed halo sign as described earlier in the previous paragraph [6].

COVID-19 pneumonia: thin section CT shows mass-like peribronchovascular and subpleural consolidation in lower lobes
Indeterminate-atypical findings
Diffuse GGO without clear distribution
This is a common finding in COVID-19 pneumonia (Fig. 12); however, it has been encountered in various diseases such as pneumocystis infection (Fig. 13), and diffuse alveolar hemorrhage (Fig. 14). So, differentiating these entities by imaging alone is difficult in such circumstances [3].

COVID-19pneumonia: parahilar GGO without round configuration and bilateral pleural effusion, despite indeterminate findings for COVID-19 pneumonia, RT-PCR test was positive for COVID-19

Pneumonia due to P jiroveci infection: thin section CT shows parahilar GGO with reticulation (crazy-paving appearance)

Pulmonary hemorrhage: thin section CT shows diffuse bilateral parahilar GGO without round configuration
Nodular opacities with ground-glass halo
Halo sign is defined as a condition in which GGO surrounds the central nodule or mass. This finding, in the thin section CT, is pathologically attributed to the presence of hemorrhage [19]. Although this appearance is unusual in COVID 19 pneumonia, it has been reported in some cases [20, 21] (Fig. 15). However, the main pathological stimulus of this manifestation still remains unknown.

COVID-19 pneumonia: thin section CT shows nodular opacity with ground glass halo
Differential diagnosis is broad, which includes infectious and noninfectious entities. Many infectious diseases including septic emboli, tuberculosis, herpes simplex virus, varicella-zoster virus, influenza, and invasive pulmonary Aspergillus (Fig. 16) have been described in this regard [19].

Angioinvasive aspergillosis represented by halo: thin section CT shows nodular area of consolidation with surrounding ground-glass opacities (halo sign) in left lower lobe
Focal consolidation
On HRCT, area of the increased lung opacity with obscuration of underlying bronchovascular markings refers to consolidation [6].
Parenchymal consolidation with multifocal, patchy, or segmental distribution in subpleural and peribronchovascular regions has been reported in 2–64% of cases infected with this disease [12]. In COVID-19 pneumonia, when there is a longer time interval between the symptom onset and CT scan, or in those patients older than 50 years old, lesions usually show a more consolidative appearance [22]. In COVID-19 pneumonia, unilateral lesions can be observed, especially immediately after the onset of symptoms, in asymptomatic patients or in those with minimal symptoms. Accordingly, they were described in 18.7% of cases in a meta-analysis of 34 studies performed on 4121 patients [23]. In these situations, sublobar pneumonia could be simulated (Fig. 17).

COVID-19 pneumonia: thin section CT shows non segmental parenchymal consolidation with airbronchogram in right lower lobe.
Differential diagnosis of parenchymal consolidation is related to the patient history; in an acute clinical setting, the infective process is highly considered. Notably, most bacterial pneumonias such as Streptococcus (Fig. 18) and Klebsiella pneumonia appear as lobar consolidation [24].

Streptococcus pneumonia: thin section CT shows segmental consolidation and GGO in left lower lobe
Centrilobular nodules
Centrilobular nodules are present in those diseases involving centrilobular bronchiole, arteriole, or lymphatic. There is sparing of subpleural interestitium, with similar spaces between adjacent nodules [6]. In COVID-19 pneumonia, imaging findings of acute bronchiolitis with centrilobular nodules have been demonstrated [1] (Fig. 19).

COVID-19 pneumonia: thin section CT shows peribronchial thickening and centrilobular nodules with tree in bud appearance. despite atypical findings for COVID-19 pneumonia, RT-PCR test was positive for COVID-19
Differential diagnosis is broad, which includes different etiologies. Although bronchiolitis is the most common cause of centrilobular nodules [6], the most common type of bronchiolitis is infectious bronchiolitis, which can be classified as acute or chronic. In addition, acute bronchiolitis is typically viral or bacterial (staphylococcus) (Fig. 20), and chronic bronchiolitis is frequently mycobacterial (Fig. 21). Acute infectious bronchiolitis in CT scan often manifests itself as centrilobular nodules with a tree in bud appearance and peribronchial thickening [25].

Infectious bronchiolitis: thin section CT shows diffuse clustered branching tree-in-bud opacities

Post primary pattern of tuberculosis: thin section CT shows bilateral tree-in-bud opacities and a cavitary masslike consolidation in the right upper lobe
Conclusion
The imaging findings in this viral pneumonia showed a broad spectrum, which indicate a considerable overlap with various infectious and non-infectious etiologies. So, there are no pathognomonic imaging findings for COVID-19 pneumonia. Although CT scan is not a diagnostic and screening tool, familiarity with different imaging findings and their differential diagnosis can be helpful in rapid and accurate decision-making.
Availability of data and materials
Not applicable.
Abbreviations
- COVID-19:
-
Novel corona virus2019
- RT-PCR:
-
Real-time polymerase chain reaction
- CT:
-
Computed tomography
- CO-RADS:
-
COVID-19 reporting and data system
- GGO:
-
Ground glass opacity
- PAP:
-
Pulmonary alveolar proteinosis
- PTE:
-
Pulmonary thromboembolism
- OP:
-
Organizing pneumonia
- GVHD:
-
Graft versus host disease
- HRCT:
-
High-resolution computed tomography
References
Wei Zhaom, Zheng Zhon, et al (2020) Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: a multicenter study AJR 215:1–6.
Salehi S, Abedi A, et al (2020) Coronavirus disease 2019(COVID-19): a systematic review of imaging findings in 919 patients. AJR 2020:2151–7
Scott Simpson, Ferendo U. Key, et al (2020) Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Rdiology 35(4)219–227
Prokop M, Van Everdingen W, Van Rees Vellinga T (2020) CO-RADS: a categorical CT assessment scheme for patients suspected of having COVID-19 definition and evaluation. Radiolog 296:E97–E104
Pan F, Ye T, Sun P, Gui S, Liang B, Li L et al (2020) Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology 295:715–721
Brett M. Elicker, Richard Webb. Fundamentals of high-resolution of lung CT. 2013
Bayraktaroğlu S, Çinkooğlu A, Ceylan N, Savaş R (2020) The novel coronavirus pneumonia (COVID-19): a pictorial review of chest CT features. Diagn Interv Radiol
Yeon Joo Jeong, Kun-Il Ki, et al (2007) Eosinophilic lung disease: a clinical, radiologic, and pathologic overview. Radiographics 619:617–637
Tomás Franquet MD (2011) Imaging of pulmonary viral pneumonia. Radiology 260(18–39)
W. Richard Webb, Nestor L. Muller, et al. High resolution CT of the lung. 2015
Kunhua Li JW, Wu F, Guo D, et al (2020) The clinical and chest CT features associated with severe and critical COVID-19 pneumonia. Invest Radiol 55(6):327–331
Zheng Ye, Yun Zhang, et al (2020) Chest CT manifestations of new coronavirus disease (COVID-19): a pictorial review. Eur Radiol 30:4381–4389
Zaere Mehrjardi M, Kahkouee S, et al (2017) Radio-pathological correlation of organizing pneumonia (OP): a pictorial review BJR 90(1071)
Edson Marchiori, Gláucia Zanetti, et al (2011) The reversed halo sign on high-resolution CT in infectious and noninfectious pulmonary diseases. AJR 197:W69–W75
Moon Hyung Choi, Jung Im Jung, et al (2014) Acute pulmonary complications in patients with hematologic malignancies. Radiographics 34:1761
MCB GOdoy, Viswanathan C, et al (2012) The reversed halo sign: update and differential diagnosis. BJR 85(1017):1226–35
Pierre Kory, Jeffrey P Kanne (2020) SARS-CoV-2 organising pneumonia:‘Has there been a widespread failure to identify and treat this prevalent condition in COVID-19. BMJ Open Resp Res 7:e000724
Kanne JP, Little BP, Chung JH et al (2020) Essentials for radiologists on COVID-19: an update—Radiology Scientific Expert Panel. Radiology 296:E113–E114
Y R Lee, Y W Choi, et al (2005) CT halo sign: the spectrum of pulmonary diseases. BJR (78):862–865
Yan Li, Liming Xia (2020).Coronavirus Disease 2019(COVID-19): role of chest CT in diagnosis and management. AJR 215:1–7
Li X, Zeng X et al (2020) COVID-19 Infection presenting with CT halo sign. Radiology 2(1):e200026
Song F, Shi N, Shan F et al (2020) Emerging coronavirus 2019-nCoV pneumonia. Radiology 295(1):210–217
Anna Rita Larici, Giuseppe Cicchetti et al (2020) Multimodality imaging of COVID-19 pneumonia: from diagnosis to follow-up. A comprehensive review. Europ J Radiol 131(109217)
Nambu A, Ozawa K et al (2014) Imaging of community-acquired pneumonia: Roles of imaging examinations, imaging diagnosis of specific pathogens and discrimination from noninfectious diseases. World J Radiol 779–793
Peter J, Winning ham, Santiago MartínezJiménez, et al (2017) Bronchiolitis: A Practical Approach for the General Radiologist. Radiographics 777–794
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
SH was a major contributor in writing the manuscript. SH and ASH contributed in collecting data. ASH and FSH contributed in revising article for important intellectual content. All authors read and confirmed the final manuscript. The author (s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shirani, F., Shayganfar, A. & Hajiahmadi, S. COVID-19 pneumonia: a pictorial review of CT findings and differential diagnosis. Egypt J Radiol Nucl Med 52, 38 (2021). https://doi.org/10.1186/s43055-021-00415-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00415-2