
Abstract
Background
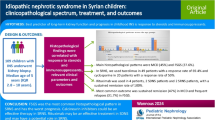
Nephrotic syndrome (NS) is a disease with favorable outcomes in most cases. Failure to respond to steroids is one of the most important predictors of clinical outcome. We performed a retrospective study on 51 primary idiopathic SRNS cases presenting between January 2011 and June 2021 at Alexandria University Children’s Hospital (AUCH) by retrieving data from their clinic files. Cases with secondary causes of NS or suspected genetic causes were excluded from our study. Patients’ demographic data, clinical and laboratory findings at the time of presentation, complications occurring during the course of treatment, immunosuppressants used along with steroids, and outcomes at the last follow-up were recorded. The mean duration of follow-up was 5.67 ± 3.07 years.
Results
Our results showed that there was male predominance (2.9:1), the mean age at first presentation was 4.53 ± 3.03 years, and persistent hematuria and systemic hypertension were found in 41.6% and 57.1%, respectively.
The most common biopsy finding was MesPGN (37.3%). The most utilized immunosuppressant was cyclosporine (80.4%). Complete remission was fortunately the most prevalent outcome among our cases (52.2%).
Conclusions
Our study concluded that biopsy findings and thepresence of hematuria in SRNS cases are the most crucial factors in determining the final outcome. MCNS finding in biopsy is significantly correlated with complete remission (p value = 0.043). Persistent hematuria whether gross or microscopic was significantly correlated with unremitting disease (p value = 0.017).
Similar content being viewed by others

Background
Nephrotic syndrome (NS) is the most common chronic glomerular disease in the pediatric age group. It is characterized by nephrotic range proteinuria, hypoalbuminemia associated with generalized edema, and hyperlipidemia [1, 2]. The most convenient way to classify idiopathic NS is to do so based on clinical response to corticosteroid therapy (CST) into steroid-sensitive NS (SSNS) and steroid-resistant NS (SRNS). Steroid-sensitive patients constitute between 80 and 90% of children with idiopathic NS, they respond to treatment with steroids within 4 weeks of induction. Those who fail to respond to CST are classified as having SRNS [3].
Minimal change disease is associated with a younger age of onset, typically between 2 and 6 years, no family history of NS, normal serum creatinine at presentation, normal serum C3, and absence of other nephritic manifestations such as hypertension (HTN) and/or gross hematuria. Complete clinical and laboratory remission is usually achieved within 4 weeks of oral CST and the incidence of progression to end-stage kidney disease (ESKD) is minimal [3].
SRNS is usually associated with other histological variants than minimal change nephrotic syndrome(MCNS), typically focal segmental glomerulosclerosis FSGS [4]. It is linked to onset at an age older than 6 years, there could be an underlying genetic cause, so it is possible to find NS among other family members. It could present with HTN, gross hematuria, persistent microscopic hematuria, elevated serum creatinine, abnormal serum complement levels, and most importantly poor response to CST after 4 weeks of oral induction regimen. Unfortunately, the rate of progression to ESKD among SRNS patients was recorded to be up to 30–40% [2, 5].
The pathogenesis of idiopathic NS is suggested to be either immune-mediated, due to a systemic podocyte-directed circulating permeability factor, or less likely a genetic variant [3].
The integrity of the glomerular filtration barrier can also be affected by genetic mutations such as in inherited familial cases of nephrotic syndrome. Genetic testing is a crucial step in SRNS especially when a family history of NS is present, especially in cases of consanguinity among parents. Presentation at an age < 1 year, presence of FSGS or mesangial proliferation on kidney biopsy should also prompt early genetic testing [1, 6, 7].
Genetic testing is important because it is unlikely that monogenic forms of SRNS will respond to immunosuppressive medications, so it is wise to spare the patient from the harmful side effects from the start if the response is unexpected. It may also provide patients and their families with a better understanding of their diagnosis, risk of recurrence among future offspring, and consequentially rate of recurrence post-transplantation [2].
The outcome of patients suffering from SRNS remains highly unpredictable given the heterogeneous number of factors that affect it. Nevertheless, certain factors can give pediatric nephrologists clues when assessing the possible outcome in each individual patient separately. The presence of persistent multidrug-resistant proteinuria, an early decline in kidney functions, as well as extensive segmental sclerosis, are predictors of early and rapid progression to chronic kidney disease (CKD). FSGS patients who have unresponsive proteinuria have been recorded to reach ESKD in 60% of the cases. On the other hand, tip lesions and success in achieving remission with steroid-sparing medication predicts good outcome [8].
Perhaps because SRNS is at the end a rare disease, research on these patients in Egypt is still scarce. Similar studies have been done in developed and developing countries to help reach a better understanding of their SRNS patients [9,10,11,12,13]. These studies are also reevaluated regularly as there is emerging evidence that the incidence of SRNS and particularly FSGS is increasing over time [10].
Methods
This study retrospectively reviewed all records of children diagnosed to have idiopathic SRNS who had been followed up in the Pediatric Nephrology Unit, Alexandria University Children’s Hospital between January 2011, and June 2021. Criteria for diagnosis of the nephrotic syndrome were nephrotic range proteinuria (urinary protein to creatinine ratio [pr/cr] in first-morning urine sample ≥ 2 mg/mg), hypoalbuminemia (serum albumin < 3 g/dl), and edema.
Inclusion criteria were resistance to steroids which was defined as failure to achieve remission at 4 weeks of daily standard dose CST (60 mg/m2/day of either prednisone or prednisolone) [2], after ensuring patients’ adherence to treatment, in patients with onset at an age older than 1 year. Exclusion criteria were secondary NS such as cases with systemic diseases as in systemic lupus erythromatosus, thrombotic microangiopathy, NS associated with malignancy, or cases with infectious and post-infectious nephritis. Those with syndromic, congenital, or hereditary forms such as Alport syndrome were excluded. Patients with a positive family history of NS were also excluded.
Data were collected from the clinic files using a standard data collection sheet. Demographic data such as age at presentation, gender, and consanguinity among parents was recorded. The presence of nephritic manifestations such as systemic HTN and/or gross hematuria was noted. Systemic HTN was diagnosed according to the American Academy of Pediatrics (AAP) guidelines [14].
Blood tests, including initial CBC at diagnosis, serum albumin, cholesterol, triglycerides, creatinine, and complement 3 (C3) levels were retrieved and those with a low C3 were excluded. Laboratory data were evaluated as “low,” “normal,” or “high” according to normal values for age [15]. Serum creatinine (Scr) was used to calculate estimated glomerular filtration rate (eGFR) using the Schwartz formula; where eGFR = 0.413[height]/Scr [16]. Urine tests, including initial pr/cr and urine analysis for the presence or absence of persistent microscopic hematuria (> 2 weeks), were reviewed. Urine was considered positive for hematuria only if RBCs in freshly voided centrifuged urine showed 5 or more cells per high power field [17]. Renal histopathology reports, treatment protocols received by each patient, responses, complications, and outcomes were also recorded.
Outcome measures were complete remission (CR), partial remission (PR), unremitting disease, progression to CKD, lost to follow-up, and death. CR was defined as proteinuria negative or trace dipstick, or first-morning pr/cr ≤ 0.2 mg/mg for 3 or more consecutive occasions. PR was defined as the persistence of proteinuria (pr/cr ratio ≥ 0.2 but < 2 mg/mg), and when available serum albumin > 3 g/dL. Unremitting patients were those who had persistent nephrotic range proteinuria and/or edema clinically [18] CKD was defined as GFR < 60 ml/min/1.73 m2 for > 3 months [19]. Patients were considered lost to follow-up if they did not show up at the clinic and there was no communication by any means at the predicted time of follow-up.
Statistical analysis of the data
Data were fed to the computer and analyzed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp) Qualitative data were described using number and percent. Kolmogorov–Smirnov test was used to verify the normality of distribution. Quantitative data were described using range (minimum and maximum), mean, standard deviation, median, and interquartile range (IQR). Significance of the obtained results was judged at the 5% level. The used tests were the chi-square test, Fisher’s exact or Monte Carlo correction, and logistic regression analysis.
Results
A total of 738 NS cases were presented between January 2011 and June 2021, and 63 (8.5%) of them were SRNS. After excluding patients with a positive family history or genetic etiology, the study included a final number of 51 idiopathic SRNS cases as shown in Fig. 1.

Study population
Among SRNS patients, males predominate with a male-to-female ratio of 2.9:1. The mean age at first presentation was 4.53 ± 3.03 with most of our patients (62.7%) presenting between 2 and 6 years. Positive consanguinity was found among 21.6% of the cases, as shown in Table 1.
Regarding systemic HTN, 54.9% of the patients were hypertensive at presentation even before CST was initiated, and continued to be hypertensive but controlled on antihypertensive medication throughout the duration of this study. At presentation, hematuria was found in 41.2%. Persistent microscopic hematuria was found in 21.6% of the cases, while 3.9% reported gross hematuria. Hematuria was transient in 15.7% of the cases (Fig. 2).

Distribution of the studied cases according to hematuria
In about one-third of the cases, the biopsy finding was MesPGN (37.3%). This was followed by both FSGS and MCNS which had an equal prevalence of 27.5%, followed by MN (5.4%) and MPGN (3.6%), as shown in Figs. 3 and 4.

Distribution of the studied cases according to biopsy results

Renal biopsy specimen from one of our patients where glomeruli show diffuse mesangial hypercellularity with non-thickened GBM, typical of MesPGN
The most commonly used drug among the SRNS patients was cyclosporine in 80.4% of the patients. Mendosa protocol was also commonly used (39.2%). The third most commonly used drug was MMF (35.3%), followed by cyclophosphamide (33.3%), rituximab (29.4%), tacrolimus (9.8%), and levimasole (3.9%), as shown in Fig. 5.

Frequency of the drugs used in the treatment of SRNS
Complications and outcome
During the duration of follow-up (mean duration 5.67 ± 3.07 years) complications were noted in 21 (41.2%) patients. Recurrent infection was recorded in 8 (15.7%) patients, with repeated hospital admissions primarily due to recurrent pneumonia, peritonitis, and urinary tract infections.
Thromboembolic complications (TECs) were recorded 7 times, in the form of cerebrovascular stroke in one patient, superior sagittal sinus thrombosis in one patient, internal jugular vein thrombosis in another patient, renal vein thrombosis in two patients, while one patient suffered from both pulmonary embolism and lower limb deep vein thrombosis. Therefore 6/51 patients (11.8%) suffered from TECs.
Ocular complications due to prolonged CST therapy were recorded 4 times. Posterior subcapsular cataract (PSC) was present in the 3 patients, while one of them developed both PSC and glaucoma. Hence, ocular complications occurred in 3/51 patients (5.9%) Hypertensive heart disease was diagnosed by echocardiography in 3/51 patients (5.9%). Glucose intolerance was recorded in 1/51 patients, this patient had a prediabetic HbA1c and fasting blood sugar tests. Another patient (1/51) developed type II diabetes mellitus and is now on both basal bolus insulin and metformin.
Other complications such as cushingoid appearance, suppressed growth velocity, and short stature were also frequently recorded in 17.6%, 17.6%, and 13.7% of the patients, respectively.
Renal re-biopsy was done in 19/51 patients (37.2%), among those who repeated their renal biopsy, evidence of CNI toxicity was found in 3/19 patients (15.8%).
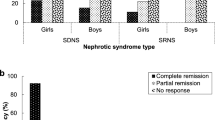
On studying the outcome at the last follow-up, 5 patients were lost to follow-up. As for the remaining 46 patients, the most common outcome was a complete remission in 24 patients (52.2%). Unfortunately, unremitting disease was the second most common outcome occurring in 16 patients (34.8%). Among those 16 patients, 7 developed ESKD, and one of them died of dialysis-related complications. A second patient also died due to unremitting disease and overwhelming sepsis. Therefore, the mortality rate was 4.3%. As for partial remission, it was achieved in 6 patients (13%).
On univariate analysis of factors affecting complete remission as an outcome, MCNS on renal biopsy was found to be a predictor of complete remission (p value = 0.043) Table 2. On univariate and multivariate analysis of factors affecting unremitting course as outcome showed that the presence of persistent hematuria is a predictor of unremitting course (p value = 0.045) (Tables 3 and 4).
Discussion
Steroid response varies greatly with the original ethnicity, for example, SRNS is three times more common among African Americans than European Americans residing in the USA. The incidence of SRNS is also lower among European studies than among African studies [20].
In this study, the prevalence of idiopathic SRNS was 6.9%. This was similar to rates reported in another study from upper Egypt, which stated that the prevalence of SRNS is 6% in a retrospective study [21]. Regional discrepancies may be ascribed to selection bias because regional tertiary care centers are used as samples rather than all children with NS. Differences in rates reported could also be attributed to the sampling technique used some studies included also patients with late steroid resistance, secondary NS, patients with low C3, or patients with a family history of NS [22,23,24,25,26].
Unlike several other studies, in this study we decided against including patients with a family history of nephrotic syndrome, this was because we believed that even if these patients had an inconclusive genetic analysis, it was still likely that they had a genetic form of NS. In Kaddah et al.’s study in Cairo, a family history of NS was present among 11.7% of SRNS patients, and when comparing their SRNS and SSNS patients, there was a significant correlation between family history and SRNS (p = 0.013) [26]. Moreover, AlHarthi reported a positive family history in 71.4% of their SRNS patients [22]. As for consanguinity among parents, it was found in 21.6% of our patients, and expectedly was found in an even higher percentage in Saudi Arabia (76%). AlHarthi actually justified that the higher percentage of SRNS patients in his study (24%) was due to this extreme rate of consanguinity among parents and positive family history [22].
Hypertension at presentation was found among 54.9% of our cases. All of them continued to be hypertensive and controlled on antihypertensive medication throughout the duration of this study. The reported rates of HTN in Cairo, Saudi Arabia, Bangladesh, and Nigeria varied between 7.5% and 81% [11, 12, 22, 27]. In Sudan their definition of HTN was clearly stated to be blood pressure above 95th percentile for age, therefore their methods were similar to ours, and not surprisingly the rate of HTN recorded was 48% which is very close to our reported rate of 54.9% [23].
As for hematuria, 25.5% of our cases had persistent hematuria either microscopic or gross. Great variation in reported incidences of persistent hematuria was noted in several other studies, with incidence ranging from 15.1 to 81% [12, 22, 23, 25, 27]. In Sudan, they used a lower cutoff value of 3 RBCs/ HPF, which might explain why they reported a higher number of cases [23]. Other studies did not clarify their cut-off values for diagnosing hematuria, so this huge discrepancy between our results and their results could be due to different definitions used. Again, we have to note that in Bangladesh they also included patients with low C3 in their study which are more likely to present with nephritic manifestations [12, 22, 23, 25].
Most of our patient’s biopsies showed MesPGN, followed by FSGS and MCNS. MesPGN was also the most common biopsy finding in several other studies [12, 26, 28, 29], while other studies reported that MCNS was the most prevalent among SRNS patients [13, 30]. Focal segmental glomerulosclerosis was the most common biopsy finding in many studies [10, 22, 24, 31]. These differences between different countries could be aroused because of ethnic differences and genetic factors. The limitation in resources might have affected these results as well. It is not clear whether all centers examined their biopsy specimens by all 3 methods, light microscope, electron microscope, and immunofluorescence. It is also uncertain whether all immune stains were readily available, especially in developing countries. Differences perhaps also occur because biopsy readings are subjective and not all centers might have an experienced pathologist in nephrology, this might have also contributed to these discrepancies between the results, as early features of FSGS might be missed.
Recurrent infections were a common complication in this study, occurring in 8/51 patients (15.7%). Details of the organisms isolated by blood or urine culture in those patients suffering from recurrent infections were lacking, however, it is well known that the most common cause of infection in cases of NS are pneumococci and E. coli. [2]. In a study from Sudan, among the most encountered complications were recurrent infections (13%) as well. Patients in their study suffered from recurrent infections in the form of respiratory tract infections, urinary tract infections, and peritonitis [23]. Pneumococcal vaccination is not present in the routine vaccination schedule in our country, so most of our patients have not received vaccinations against pneumococci, which explains their susceptibility and the high rate of recurrent infections recorded.
The reported incidence of thromboembolic complications in NS is 3% [32]. We reported an incidence of 11.8% (6/51) among our SRNS patients. When screened for abnormalities of thrombophilia, two of these patients were proven to have an abnormal thrombophilia profile and are currently on lifelong anticoagulants. Nevertheless, the incidence reported in our cases is high probably due to the prolonged duration of proteinuria in cases of steroid resistance, associated with a persistent hypercoagulable state.
A retrospective study performed in New Delhi, India, by Sharma et al. in SRNS patients, showed that the rate of CNI toxicity for both tacrolimus and cyclosporin in follow-up biopsies after an average of 30 months was 7.5% and 17.5%, respectively. They concluded that longer durations of proteinuria, higher doses of CNIs, concomitant HTN, as well as initial steroid resistance were associated with a significantly increased risk of CNI toxicity [33].
In this study, we fortunately reported a lower rate of CNI toxicity in 3 of the 19 patients who underwent re-biopsy (15.8%). To avoid nephrotoxicity even when remission was achieved with the help of cyclosporine, it was gradually replaced by a less nephrotoxic drug such as MMF. Periodic assessment of GFR is also performed, so that re-biopsy is considered in case of GFR affection or after completion of 2 years on cyclosporine regimen. Nevertheless, cyclosporine was also administered for an even shorter duration in patients who showed unremitting disease when it failed to induce remission.
There is no clear consensus regarding the interval for testing for ocular complications; however, we have adapted the practice of requesting full ophthalmological assessment at least annually or earlier if indicated for our patients. Complications were recorded 4 times, where 3 patients had PSC, and one of them suffered from glaucoma as well. Hence, ophthalmological complications were recorded in 3/51 patients (5.9%).
HbA1C and fasting blood sugar are performed at least every 6 months as advised by IPNA, especially in cushingoid patients, the finding that 1/51 of patients has glucose intolerance and another patient (1/51) developed type II DM is therefore a true representative of the magnitude of the problem [2].
We also found that the most frequently recorded complications in this study were drug-related rather than disease-related. The 2 most recorded complications were cushingoid appearance (17.6%) and suppressed growth velocity (17.6%). Short stature was recorded in 13.7% of the cases. A similar observation was found in a retrospective study done in Saudi Arabia by Kari et al. [34]. According to IPNA’s guidelines for the management of SRNS patients, height and weight measurements should be obtained and plotted on a growth chart at least every 3 months, an annual height velocity should also be calculated based on these measurements [2].
The mean duration of follow-up in this study was 5.67 ± 3.07 years. Surprisingly, the most common outcome in this study and in several other studies was remission [12, 13, 24], with complete remission still having the highest prevalence. However, AlHarthi in Saudi Arabia has described that more than half of SRNS patients in their study developed CKD [22]. Moreover, the mortality rate in this study (4.3%), was also lower than that recorded in other studies [12, 22]. We think that our studied group of patients had a better outcome because we excluded cases with a positive family history, those with secondary causes of NS and those with positive genetic studies.
In this study, the results show that initial results of renal pathology and the presence of hematuria are the strongest predictors of outcome. The most important predictive factor for remission in this study was MCNS on renal biopsy (p value = 0.043). There was a significant correlation between failure to achieve remission and patients with persistent hematuria whether gross or microscopic (p value = 0.045). Inaba et al. concluded that patients with FSGS on biopsy, especially those who did receive initial treatment with cyclophosphamide rather than cyclosporine had the lowest renal survival rate [13]. Mendonca et al. concluded that steroid resistance, along with hematuria at presentation, as well as age of onset were the prime factors predicting patients’ outcomes [35].
Conclusion
This study concluded that achieving remission in patients with primary SRNS is possible. Nevertheless, maintaining this remission and avoidance of frequent relapses, while avoiding long-term exposure to immunosuppressants remains challenging. The presence of persistent microscopic hematuria or gross hematuria is a predictor of poor outcome (unremitting disease).
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available to protect patient confidentiality but are available from the corresponding author on reasonable request.
Abbreviations
- ACEis:
-
Angiotensin-converting enzyme inhibitors
- ARBs:
-
Angiotensin receptor blockers
- C3:
-
Complement 3
- CKD:
-
Chronic kidney disease
- CNIs:
-
Calcineurin inhibitors
- CR:
-
Complete remission
- CST:
-
Corticosteroid therapy
- DDD:
-
Dense deposit disease
- eGFR:
-
Estimated glomerular filtration rate
- EM:
-
Electron microscopy
- ESKD:
-
End stage kidney disease
- FSGS:
-
Focal segmental glomerulosclerosis
- GBM:
-
Glomerular basement membrane
- HTN:
-
Hypertension
- IF:
-
Immunoflouresence microscopy
- IPNA:
-
International pediatric nephrology association
- IV:
-
Intravenous
- LM:
-
Light microscopy
- MCNS:
-
Minimal change nephrotic syndrome
- MesPGN:
-
Mesangioproliferative glomerulonephritis
- MMF:
-
Mycophenolate mofetil
- MN:
-
Membranous nephropathy
- MPGN:
-
Membranoproliferative glomerulonephritis
- NS:
-
Nephrotic syndrome
- PR:
-
Partial remission
- pr/cr:
-
Protein to creatinine ratio
- PSC:
-
Posterior subcapsular cataract
- SRNS:
-
Steroid-resistant nephrotic syndrome
- SSNS:
-
Steroid-sensitive nephrotic syndrome
- TECs:
-
Thromboembolic complications
References
Nourbakhsh N, Mak RH (2017) Steroid-resistant nephrotic syndrome: past and current perspectives. Pediatric Health Med Ther 8:29–37
Trautmann A, Vivarelli M, Samuel S, Gipson D, Sinha A, Schaefer F et al (2020) IPNA clinical practice recommendations for the diagnosis and management of children with steroid-resistant nephrotic syndrome. Pediatr Nephrol 35(8):1529–1561
Downie ML, Gallibois C, Parekh RS, Noone DG (2017) Nephrotic syndrome in infants and children: pathophysiology and management. Paediatr Int Child Health 37(4):248–258
Trautmann A, Lipska-Zietkiewicz BS, Schaefer F (2018) Exploring the clinical and genetic spectrum of steroid resistant nephrotic syndrome: The PodoNet Registry. Front Pediatr 6:200
Trautmann A, Schnaidt S, Lipska-Zietkiewicz BS, Bodria M, Ozaltin F, Emma F et al (2017) Long-term outcome of steroid-resistant nephrotic syndrome in children. J Am Soc Nephrol 28(10):3055–3065
Shatat IF, Becton LJ, Woroniecki RP (2019) Hypertension in childhood nephrotic syndrome. Front Pediatr 7:287
Dogra S, Kaskel F (2017) Steroid-resistant nephrotic syndrome: a persistent challenge for pediatric nephrology. Pediatr Nephrol 32(6):965–974
Abeyagunawardena AS, Sebire NJ, Risdon RA, Dillon MJ, Rees L, Van’t Hoff W et al (2007) Predictors of long-term outcome of children with idiopathic focal segmental glomerulosclerosis. Pediatr Nephrol 22(2):215–221
Rahbar M (2016) Histopathology review of idiopathic steroid resistant nephrotic syndrome and outcome in children in north-west of Iran. Open J Nephrol 06(04):188–199
Mubarak M, Kazi JI, Shakeel S, Lanewala A, Hashmi S (2012) The spectrum of histopathological lesions in children presenting with steroid-resistant nephrotic syndrome at a single center in Pakistan. SciWorldJ 2012:681802
Asinobi AO, Ademola AD, Okolo CA, Yaria JO (2015) Trends in the histopathology of childhood nephrotic syndrome in Ibadan Nigeria: preponderance of idiopathic focal segmental glomerulosclerosis. BMC Nephrol 16:213
Roy RR, Rahman F, Arju J, Sultana J, Chaki A, Akter A, et al (2014) Steroid resistant nephrotic syndrome in children: Clinical presentation, renal histology, complications, treatment and outcome at Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. IOSR J Pharm 4(11):1–7
Inaba A, Hamasaki Y, Ishikura K, Hamada R, Sakai T, Hataya H et al (2016) Long-term outcome of idiopathic steroid-resistant nephrotic syndrome in children. Pediatr Nephrol 31(3):425–434
Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al (2017) Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140(3):e20171904
Colantonio DA, Kyriakopoulou L, Chan MK, Daly CH, Brinc D, Venner AA et al (2012) Closing the gaps in pediatric laboratory reference intervals: a CALIPER database of 40 biochemical markers in a healthy and multiethnic population of children. Clin Chem 58(5):854–868
Copelovitch L, Warady BA, Furth SL (2011) Insights from the Chronic Kidney Disease in Children (CKiD) study. Clin J Am Soc Nephrol 6(8):2047–2053
Viteri B, Reid-Adam J (2018) Hematuria and Proteinuria in Children. Pediatr Rev 39(12):573–587
Kidney Disease: Improving Global Outcomes Glomerular Diseases Work G. KDIGO 2021 Clinical practice guideline for the management of glomerular diseases. Kidney Int. 2021;100(4S):S1-S276.
Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J et al (2005) Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 67(6):2089–2100
Chanchlani R, Parekh RS (2016) Ethnic Differences in Childhood Nephrotic Syndrome. Front Pediatr 4:39
Abd-Elrehim GA, Ahmed AA, Fadda S, Ali SH, Ahmed NF (2017) Patterns of idiopathic nephrotic syndrome in upper egyptian children. Sohag Med J 21(1):153-60
Alharthi AA (2017) Patterns of childhood steroid-sensitive and steroid-resistant nephrotic syndrome in Saudi Children. Clin Pediatr (Phila) 56(2):177–183
El-Tigani MAA, Makki HFK, Mohamed BA, Salwa OM, Allidir RA (2017) Childhood idiopathic steroid-resistant nephrotic syndrome at a single center in Khartoum. Saudi J Kidney Dis Transpl 28(4):851–9
Kari JA, Halawani M (2010) Treatment of steroid resistant nephrotic syndrome in children. Saudi J Kidney Dis Transpl 21(3):484–7
Wasiu AO, Kayode AA, Adefehinti O (2010) Childhood Idiopathic Steroid Resistant Nephrotic Syndrome in Southwestern Nigeria. Saudi J Kidney Dis Transpl 21(5):979–90
Kaddah A, Sabry S, Emil E, El-Refaey M (2012) Epidemiology of primary nephrotic syndrome in Egyptian children. J Nephrol 25(5):732–737
Seif EI, Ibrahim EA, Elhefnawy NG, Salman MI (2013) Histological patterns of idiopathic steroid resistant nephrotic syndrome in Egyptian children: A single centre study. J Nephropathol 2(1):53–60
Shah SSH, Akhtar N, Sunbleen F, Fahim ur Rehman M, Ahmed T (2015) Histopathologic patterns in pediatric idiopathic steroid resistant nephrotic syndrome J Ayub Med Coll Abbottabad 27(3):633–6
Zhou TB, Lin N, Qin YH, Liu YG (2014) Distribution of pathological finding in the children with nephrotic syndrome from Guangxi. Saudi J Kidney Dis Transpl 25(3):684–8
Bakr A, Eid R, Sarhan A, Hammad A, El-Refaey AM, El-Mougy A et al (2014) Pathological profile of biopsied egyptian children with primary nephrotic syndrome: 15-year single center experience. J Nephrol 27(4):419–423
Javadilarijani F, Ahmadpanah A, Seddigh L, Movahhed SM, Arefi M, et al (2015) Histopathologic characteristics of steroid-resistant nephrotic syndrome children in Iran. J Ped Nephrol 3(3):100–3
Kerlin BA, Haworth K, Smoyer WE (2014) Venous thromboembolism in pediatric nephrotic syndrome. Pediatr Nephrol 29(6):989–997
Sinha A, Sharma A, Mehta A, Gupta R, Gulati A, Hari P et al (2013) Calcineurin inhibitor induced nephrotoxicity in steroid resistant nephrotic syndrome. Indian J Nephrol 23(1):41–46
Kari JA, El-Desoky SM, Gari M, Malik K, Vega-Warner V, Lovric S et al (2013) Steroid-resistant nephrotic syndrome: impact of genetic testing. Ann Saudi Med 33(6):533–538
Mendonca AC, Oliveira EA, Froes BP, Faria LD, Pinto JS, Nogueira MM et al (2015) A predictive model of progressive chronic kidney disease in idiopathic nephrotic syndrome. Pediatr Nephrol 30(11):2011–2020
Acknowledgements
Special thanks are also in order to our hard-working colleagues in the pathology department at Alexandria University, Prof. Dr. Nahed Baddour, Dr. Maram Allam, and Dr. Heba Refaat. Your cooperation with us is always highly appreciated.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
YE collected patient data from clinic files, performed statistical analysis of data, interpreted the results, and wrote the study design and manuscript. ME created the study design, interpreted the data, and revised, read, and approved the final manuscript. HF created the study design, interpreted the data, and revised, read, and approved the final manuscript. NA perfomed renal biopsy sampling of most patients, interpreted the data, and revised, read, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This manuscript was accepted according to the ethical standards of scientific research set by the Ethics Committee, Faculty of Medicine, Alexandria University.
Serial Number: 0106736.
Date: 19/3/2021.
Consent for publication
Verbal consent for publication was obtained after confirming approval of the patient’s guardians’ agreement on informed consent in accordance to publication regulations as anonymous data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elbeltagi, Y.A.H., Kersh, M.M.E.D.E., Fathy, H.M. et al. Study of steroid-resistant nephrotic syndrome: a single center experience. Egypt Pediatric Association Gaz 72, 35 (2024). https://doi.org/10.1186/s43054-024-00267-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-024-00267-1