
Abstract
Objective
The aim of this study is to evaluate the relationship between dental caries, food intake, and body composition in school-age children.
Methods
The study was conducted on 210 children, 105 boys and 105 girls, aged 6–12 years, without mental and/or physical disorders. Oral examinations of the children were performed by paediatric dentists and DMFT–DMFS and dmft–dmfs values were recorded. A detailed food frequency questionnaire was applied to determine the consumption frequency of dairy products and sugar‐added foods. Children’s height, waist and hip circumference measurements were taken by the researcher; body weight and body composition were evaluated with a Tanita body analyzer.
Results
The DMFS value of children who consumed white cheese daily is lower than children who did not (p < 0.05). The DMFT and DMFS values were found to be higher in children who consumed sweets, biscuits, and spreadable chocolate daily compared to children who did not (p < 0.05). Body weight and waist circumference are positively correlated with DMFT and negatively correlated with dmft. BMI is positively correlated with DMFT and negatively correlated with dmft (p < 0.05). In binary logistic regression, it was found that maternal education level, frequency of added sugar intake and body fat ratio were predictors of the presence of caries.
Conclusion
In this study, dental caries was associated with food consumption and body mass index. In children, consumption of sugary foods should be reduced and consumption of dairy products should be increased.
Similar content being viewed by others


Background
In the transition from childhood to adolescence, the school-age period is a critical life phase in which nutritional and oral health habits develop [1]. Dental caries are a common chronic disease in school-age children, although it is now known that it is almost completely preventable. Dental caries are frequently seen due to the changing lifestyle and the increase in the consumption amount and frequency of sugar and sugary foods [2].
While studies indicate that the prevalence of caries in children has decreased in many developed countries, dental caries is still an important public health problem in developing countries [3, 4]. Globally, the World Health Organization (WHO) reports that the prevalence of dental caries in school-age children in most countries is between 60 and 90% [5].
The main factors controlling the risk of dental caries in school-age children are dietary habits, oral hygiene and fluoride exposure [6]. The frequency and amount of consumption of simple sugars are associated with dental caries. According to epidemiological, animal and human intervention studies, both frequency and amount of sugar consumption are important in caries etiology. The frequency of added sugar consumption is a more dominant factor in the etiology of dental caries, but there is evidence that the amount of sugar consumption affects the development of dental caries regardless of frequency [2].
The prevalence of childhood obesity has increased due to changes in diet and lifestyle. Childhood obesity is likely to continue into adulthood and causes many problems, including the increased risk of developing chronic diseases. Many studies in the literature have associated dental caries with childhood obesity. Since childhood obesity is generally evaluated with body mass index, BMI is generally used to evaluate between dental caries and childhood obesity. In addition to BMI, anthropometric measurements (such as circumferences), BMI and bioelectric impedance analysis (BIA) are used for estimation of body composition, particularly body fat ratio. Body fat ratio provides a more specific assessment of body composition compared to BMI and is a reliable screening tool for obesity. BIA is an effective method used in determining body composition, with rapid results and reproducibility in both children and adults. BIA is also used to evaluate the relationship between dental caries and childhood obesity [6,7,8,9].
There is a limited number of studies evaluating the relationship between dental caries, food consumption and body composition in school-age children. We hypothesized children who consume more milk and dairy products have less dental caries and children who consume more sugar and sugary foods have more dental caries. Also, we hypothesized that there is an association between body mass index (BMI) and dental caries. In this context, this study was conducted to evaluate the relationship between dental caries, food consumption and body composition in 6–12 years old children.
Methods
Study design and procedure
A total of 210 children aged 6–12 years, 105 boys and 105 girls without mental and/or physical disorders who applied to Hacettepe University Faculty of Dentistry Department of Pedodontics with dental problems were included in this study. In this study, the sample size was determined as 210 children using the GPower software version 3.1 (α = 0.05, 1-β = 0.95) based on a similar study [10]. This study was conducted as a master’s thesis and was approved by the Ethics Committee of Ankara University (protocol numbered 56,786,525–050.04.04/14466). Before the questionnaire was applied, children and their families were informed about the content of the study. Parents gave written consent, and children gave verbal consent.
Assessment of children’s dental health
In order to evaluate the oral health practices of children, using of toothbrushes, frequency of tooth brushing, using of fluoride toothpaste and the frequency of dentist visiting were questioned with a questionnaire form. Dental examinations of the children were conducted at Hacettepe University, Faculty of Dentistry, Department of Pediatric Dentistry. Dental examinations were performed by two paediatric dentists under a reflector light with a mirror and a probe. Dental caries of the primary and permanent teeth were measured by the total number of decayed, missing, filled teeth (DMFT and dmft) according to the guidelines of the WHO. Also decayed, missing, filled tooth surfaces (DMFS and dmfs) were measured for each child [11]. Inter-examiner and intra-examiner reliability was evaluated with Cohen’s kappa test. The intra-examiner reliability was 0.89 and 0.90, and the inter-examiner reliability was 0.90.
Assessment of food consumption
Dietary intake was obtained from mothers by a 24-h dietary recall method. Dietary intake was completed by asking the child himself/herself when it was necessary. All the foods and beverages children consumed the other day were recorded. Detailed data about food preparation methods, ingredients used in mixed dishes and the brand names of commercial products were recorded. The amounts of each food consumed were estimated in reference to a common size container (e.g. bowls, cups, and glasses), standard measuring cups and spoons. A detailed food frequency questionnaire was applied to determine the consumption frequency of dairy products and sugar‐added foods (biscuits, spreadable chocolate, sweets, etc.) in the past month. Frequency was categorized as 1–2 times a day, 4–5 times a week, 3 times a week, 1–2 times a week, 1–2 times a month and never.
Measurements
Body height was measured to the nearest 0.1 cm with a stadiometer. Body weight and body fat (%) were measured with the bioelectrical impedance analysis (BIA) method. For this, Tanita’s body analyzer was used in children after overnight fasting. BMI (kg/m2) values were calculated according to the formula (body weight (kg)/ height2 (m2)). Waist and hip circumferences were measured to the nearest 0.1 cm using a nonelastic measuring tape. Waist circumference was measured at mid-distance between the bottom of the rib cage and the top of the iliac crest. Hip circumference measurement was taken around the widest portion of the buttocks [12]. BMI classification in children was made according to WHO (2007) reference values. Children were divided into four groups according to the BMI for age percentile: underweight, less than the 5th percentile; healthy weight, 5th percentile up to the 85th percentile; overweight, 85th to less than the 95th percentile; and obese, equal to or greater than the 95th percentile [13].
Statistical analysis
The statistical analysis of the data was performed using the SPSS 22 program. Whether the quantitative data has a normal distribution or not was evaluated with the “Kolmogrov–Smirnov” test. Descriptive statistics were expressed with mean ± standard deviations (X̄ ± SD) for normally distributed variables, median and interquartile ranges for variables with non-normal distribution, and numbers (n) and percentages (%) for nominal variables. Fisher’s exact chi-square test was used to compare categorical data. For examining the correlations between two quantitative variables, the Pearson correlation coefficient was used when at least one of the variables showed normal distribution, and the Spearman correlation coefficient was used when did not. A binary logistic regression model was developed to estimate the likelihood of having caries in permanent dentition, considering as independent variables: maternal and paternal education level, frequency of tooth brushing, frequency of intake of added sugar, and body fat ratio. For logistic regression, caries was classified as present or not present according to DMFT values. 95% confidence intervals were used in this study.
Results
Oral health behaviours of children by sex are given in Table 1. Of all the children, 43.8% brushed their teeth once a day, 29.5% brushed twice a day and 26.7% brushed irregularly. But there was no statistically significant difference between tooth brushing frequency groups (p = 0.177, p > 0.05). The vast majority of children (86.1%) reported that they visit the dentist when they have dental complaints. There was a statistically significant difference between dentist visiting frequency groups (p < 0.05).
The mean values of dental health indicators by the daily consumption of milk and dairy products are shown in Table 2. The DMFS of children who consumed white cheese daily is lower than children who did not (p < 0.05).
The mean values of dental health indicators by daily consumption of sugar and sugary foods are given in Table 3. The DMFT and dmfs values were found to be higher in children who consumed biscuits daily compared to children who did not (p < 0.05). The DMFS values were found to be higher in children who consumed sweets and spreadable chocolate daily compared to children who did not (p < 0.05).
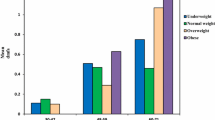
The correlations between anthropometric measurements, body composition and dental health indicators are shown in Table 4. Height and body weight are found to be correlated with DMFT–dmft and DMFS–dmfs indexes. Waist circumference is found to be positively correlated with DMFT and DMFS and negatively correlated with dmft, but waist-to-hip ratio was found to be positively correlated with only DMFS (p < 0.05). BMI was found to be positively correlated with DMFT and DMFS and negatively correlated with dmft (p < 0.05).
Factors associated with dental caries were analyzed using logistic regression as shown in Table 5. Various factors including maternal and paternal education levels, frequency of brushing, frequency of added sugar intake and body fat ratio were included in the model. After simple logistic regression, maternal education level, paternal education level, frequency of added sugar intake and body fat ratio were found significant variables (p < 0.2). Among the covariates maternal education level, frequency of sugar intake and body fat ratio remained significantly associated with the presence of caries (p < 0.05) in the multiple logistic regression model.
Children with mothers at a primary school level of education were 2.64 times more likely to have dental caries than children who had mothers with a higher level of education (AOR = 2.64; 95% CI 0.77–9.01). Children who consumed sugar daily were 1.67 times more likely to have dental caries (AOR = 1.67; 95% CI 0.80–3.48). Children with a higher body fat ratio were 12% more likely to have caries in permanent dentition (AOR = 1.12; 95% CI 1.04–1.22).
Discussion
In this cross-sectional study, the effects of dietary habits and body composition on dental caries were examined. Children with mixed and permanent dentition were included in this study. Those who brush their teeth more than once a day until the age of 12 are more likely to continue this habit in adolescence and adulthood [14]. In this study, even half of the children do not brush their teeth once a day. Considering the use of fluoride toothpaste, 72.4% of the children use it and there was no difference between sexes (Table 1).
DMFT and dmft indexes are widely used in studies to determine dental health in the world. In the present study, the mean DMFT value of the children was found as 2.02 ± 1.89 (data not shown in the table). In studies conducted in different regions of Turkey, different DMFT and dmft values were obtained [10, 15,16,17,18]. In a study conducted with a total of 4657 people across Turkey, the average DMFT index for children aged 12 was determined to be 1.9 ± 2.2 [15].
Milk and dairy products have a low cariogenic potential, but also laboratory studies have suggested that milk or milk components might have cariostatic properties [19, 20]. However, the results of epidemiological studies on the relationship between dental caries and the consumption of dairy products in children have been inconsistent [20,21,22,23].
In this study, the DMFT value was lower in children who consumed milk daily than those who did not but this correlation is not statistically significant. Similar to our study, Raj et al. found that whole-milk intake showed an inverse correlation with dental caries and BMI in children aged 6–10 years, but this correlation was statistically non-significant [24]. Tanaka et al. and Marshall et al. reported that milk had a neutral association with dental caries in young children [23, 25]. Also, Petti et al. (1997) have suggested that milk had a caries preventive effect only on those subjects with the highest frequency of sucrose consumption in children aged 6–11 [26].
In the literature, it has been reported that children with overweight and obesity prefer sugary and fatty snacks more frequently than children with normal weight. Sugary food consumption increases not only the risk of obesity but also increases the risk of dental caries [27,28,29]. In this study, DMFT and DMFS values were higher in children who consumed sweets, biscuits and spreadable chocolate daily than those who did not (p < 0.05). Similarly to our study, a study conducted in Spain found that the frequency of biscuit intake in school-age children was associated with the prevalence of caries [29]. In another study conducted with children aged 6–11 years, consumption of sugary foods was one of the predictors of caries experience [30]. In this study, the frequency of added sugar intake was a predictor of caries experience (1.67; 95% CI 0.80–3.48).
In the present study, a positive association was observed between BMI and DMFT–DMFS indexes (p < 0.05). This finding is consistent with many cross-sectional studies that showing a positive association between dental caries and childhood obesity in the permanent dentition [9, 10, 27, 28, 31]. However, some studies show that dental caries were more common in underweight children [9, 32, 33]. In addition, one study reported that dental caries is associated with both high and low BMI [27].
There is a growing body of scientific literature about the relationship regarding dental caries and obesity which is increasingly recognized as a global concern among children. However, the number of studies examining this relationship is not sufficient, and there are conflicting opinions on this issue [34,35,36].
For identifying the association between dental caries and body composition, body fat ratio and anthropometric measurements were used in this study. A positive association was observed between the body fat ratio assessed by the BIA method and permanent teeth indicators; a negative relationship was observed between the body fat ratio and primary teeth indicators but these correlations are not statistically significant (p > 0.05). A similar study showed that the body fat ratio measured by the same method was negatively correlated with dmft scores and positively correlated with DMFT scores but the correlations were significant [37]. Also in this study, the binary logistic regression model showed that children with higher body fat ratios were more likely to have caries in permanent dentition (OR, 1.12; 95% CI 1.04–1.22).
Although body mass index is the most common measure of general obesity, waist circumference is also considered an accurate marker of central obesity in children [38]. In this study, waist circumference is positively correlated with DMFT in permanent dentition and dmft in primary dentition. Peng et al. reported that dental caries experience was associated with central adiposity in children aged 5 years and 12 years, respectively [35, 36].
Parents have a great influence on the children’s dental health. Gaining dental care habits begins at home with parents, especially mothers [39,40,41]. In this study, children whose mothers had higher education levels were less likely to have dental caries. This result supports the findings of several studies that maternal educational level is an influential factor in the odds of having dental caries [39, 40, 42].
The biggest strength of this study is that it is one of the limited number of studies evaluating the relationship between dental caries and body composition. We assessed the body fat ratio by the BIA method and measured waist-hip circumferences, in addition to conventional anthropometric indices like BMI. However, this study has some limitations. The findings of this study are only valid within children applied to Hacettepe University Faculty of Dentistry Department of Pedodontics with dental problems. The sample size could have been larger. This is because of the difficulty and cost of assessing body composition.
Conclusion
In conclusion, dental caries has been associated with both food consumption and body composition in a sample of Turkish school-age children. Also, this study demonstrates a direct relationship between dental caries and childhood obesity through a correlation between dental health indicators and BMI. In children, consumption of added sugar and sugary foods should be reduced and consumption of dairy products should be increased. Further studies with a multidisciplinary diagnostic approach (nutritionists and paediatric dentists) are needed to examine the relationship between childhood obesity and dental caries in depth.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request. The data are not publicly available due to privacy or ethical restrictions.
References
World Health Organization (2003) Oral health promotion: an essential element of a health-promoting school. World Health Organization. p 64. https://apps.who.int/iris/handle/10665/70207
Zero DT, Moynihan P, Lingstrom P, Birkhed D (2008) The role of dietary control. In: Fejerskov O, Kidd E, editors. Dental caries: The disease and its clinical management. 2nd ed. UK: Blackwell Munksgaard p 329–352
Edelstein B (2006) The dental caries pandemic and disparities problem. BMC Oral Health 6(Suppl 1):2
Moynihan P, Petersen PE (2004) Diet, nutrition and the prevention of dental diseases. Public Health Nutr 7(1A):201–226
Petersen PE (2003) The World Oral Health Report 2003: continuous improvement of oral health in the 21st century–the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol 31(1):3–24
Kantovitz KR, Pascon FM, Rontani RMP, Gaviao MBD (2006) Obesity and dental caries-a systematic review. Oral Health Prev Dent 4:137–144
Hayden C, Bowler JO, Chambers S, Freeman R, Humphris G, Richards D et al (2013) Obesity and dental caries in children: a systematic review and meta-analysis. Community Dent Oral Epidemiol 41(4):289–308
Li LW, Wong HM, Peng SM, McGrath CP (2015) Anthropometric measurements and dental caries in children: a systematic review of longitudinal studies. Adv Nutr 6(1):52–63. https://doi.org/10.3945/an.114.006395
Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N (2012) Body mass index and dental caries in children and adolescents: a systematic review of literature published 2004 to 2011. Syst Rev 21:1–57
Köksal E, Tekçiçek M, Yalcın SS, Tuğrul B, Yalçın S, Pekcan G (2011) Association between anthropometric measurements and dental caries in Turkish school children. Cent Eur J Publ Heal 19(3):147–151
WHO (2013) Oral Health Surveys Basic Methods. 5th Edition. WHO Library Cataloguing 1–137
Willett W (2012) Nutritional Epidemiology, 3rd edn, Monographs in epidemiology and biostatistics (online edn, Oxford Academic, 24 Jan. 2013)
WHO. Growth reference data for 5–19 years. 2007. https://www.who.int/growthref/who2007_bmi_for_age/en/
Koivusilta L, Honkala S, Honkala E, Rimpela A (2003) Toothbrushing as part of the adolescent lifestyle predicts education level. J Dent Res 82(5):361–366
Gökalp S, Doğan B, Tekçiçek M, Berberoğlu A, Ünlüer Ş (2007) Beş, on iki ve on yaş çocukların ağız diş sağlığı profili, Türkiye-2004. Hacettepe Diş Hekimliği Fakültesi Dergisi 31(4):3–10
Altun C, Güven G, Başak F, Akbulut E (2005) Altı-onbir yaş grubu çocukların ağız-diş sağlığı yönünden değerlendirilmesi. Gülhane Tıp Dergisi 47:114–118
Yıldız E, Şimşek M, Gündoğar Z, Aktan AM (2015) Oral health survey of children referring to faculty of dentistry in Gaziantep. Gaziantep Medical Journal 21:118–124
Güler Ç, Eltas A, Güneş D, Görgen V, Ersöz M (2012) Evaluation of oral-dental health status of the children aged among 7–14 years in Malatya. İnönü Üniversitesi Sağlık Bilimleri Dergisi 2:19–24
Clemens RA, Hernell O, Michaelsen KF (eds): (2011) Milk and milk products in human nutrition. Nestlé Nutr Inst Workshop Ser Pediatr Program 67: 55–66, Nestec Ltd., Vevey/S. Karger AG, Basel
Shkembi B, Huppertz T (2023) Impact of dairy products and plant-based alternatives on dental health: food matrix effects. Nutrients 15(6):1469. https://doi.org/10.3390/nu15061469
Dror DK, Allen LH (2014) Dairy product intake in children and adolescents in developed countries: trends, nutritional contribution, and a review of association with health outcomes. Nutr Reviews 72(2):68–81
Levine RS, Nugent ZJ, Rudolf MC, Sahota P (2007) Dietary patterns, toothbrushing habits and caries experience of schoolchildren in West Yorkshire. England Community Dent Health 24(2):82–87
Tanaka K, Miyake Y, Sasaki S (2010) Intake of dairy products and the prevalence of dental caries in young children. J Dent 38(7):579–583
Raj A, Kashyap S, Kundra K, Kandari S, Rela R, Naz F (2022) Correlation between bmi, caries prevalence, and sugar-containing beverage intake in 6–10 year old children. J Pharm Bioallied Sci 14(Suppl 1):S991–S994. https://doi.org/10.4103/jpbs.jpbs_814_21
Marshall TA, Levy SM, Broffitt B, Warren JJ, Eichenberger-Gilmore JM, Burns TL, Stumbo PJ (2003) Dental caries and beverage consumption in young children. Pediatrics 112(3 Pt 1):e184–e191. https://doi.org/10.1542/peds.112.3.e184
Petti S, Simonetti R, SimonettiD’Arca A (1997) The effect of milk and sucrose consumption on caries in 6-to-11-year-old Italian schoolchildren. Eur J Epidemiol 13(6):659–664. https://doi.org/10.1023/a:1007343904877
Sharma S, Hegde AM (2009) Relationship between body mass index, caries experience and dietary preferences in children. J Clin Pediatr Dent 34:49–52
Alm A, Fåhraeus C, Wendt LK, Koch G, Andersson-Gäre B, Birkhed D (2008) Body adiposity status in teenagers and snacking habits in early childhood in relation to approximal caries at 15 years of age. Int J Paediatric Dent 18(3):189–196
Monteagudo C, Téllez F, Heras-González L, Ibañez-Peinado D, Mariscal-Arcas M, Olea-Serrano F (2015) School dietary habits and incidence of dental caries. Nutr Hosp 32(1):383–388
Amato JN, de Sousa Eskenazi EM, Massaoka C, de Araújo de Assis CR, Castelo PM, (2022) Relation between caries experience and the consumption of sweetened drinks and processed food in children: a population-based study. Int J Dent Hyg. https://doi.org/10.1111/idh.12662.Advanceonlinepublication.10.1111/idh.12662
Paisi M, Kay E, Bennett C, Kaimi I, Witton R, Nelder R et al (2019) Body mass index and dental caries in young people: a systematic review. BMC Pediatr 19(1):122
Alkarimi HA, Watt RG, Pikhart H, Sheiham A, Taskos G (2014) Dental caries and growth in school-age children. Pediatrics 133(2):616–623
Markovic D, Ristic-Medic D, Vucic V, Mitrovic G, NkolicIvosevic J, Peric T et al (2015) Association between being overweight and oral health in Serbian schoolchildren. Int J Paediatr Dent 25(6):409–417
Palmer CA (2005) Dental caries and obesity in children: different problems, related causes. Quintessence Int 36:457–461
Peng SM, Wong HM, King NM, McGrath C (2014) Is dental caries experience associated with adiposity status in preschool children? Int J Pediatr Dent 24(2):122–130. https://doi.org/10.1111/ipd.12039
Peng SM, Wong HM, King NM, Mcgrath C (2014) Association between dental caries and adiposity status (general, central, and peripheral adiposity) in 12-year-old children. Caries Res 48(1):32–38
Yen CE, Lin YY, Hu SW (2021) Anthropometric status, diet, and dental caries among schoolchildren. Int J Environ Res Public Health 18(13):7027. https://doi.org/10.3390/ijerph18137027
Hubert H, Guinhouya CB, Allard L, Durocher A (2009) Comparison of the diagnostic quality of body mass index, waist circumference and waist-to-height ratio in screening skinfold-determined obesity among children. J Sci Med Sport 12(4):449–451. https://doi.org/10.1016/j.jsams.2008.05.002
Chen L, Hong J, Xiong D, Zhang L, Li Y, Huang S, Hua F (2020) Are parents’ education levels associated with either their oral health knowledge or their children’s oral health behaviors? A survey of 8446 families in Wuhan. BMC Oral Health 20(1):203. https://doi.org/10.1186/s12903-020-01186-4
van der Tas JT, Kragt L, Elfrink MEC, Bertens LCM, Jaddoe VWV, Moll HA, Ongkosuwito EM, Wolvius EB (2017) Social inequalities and dental caries in six-year-old children from the Netherlands. J Dent 62:18–24. https://doi.org/10.1016/j.jdent.2017.04.008
Marshall TA, Eichenberger-Gilmore JM, Broffitt BA, Warren JJ, Levy SM (2007) Dental caries and childhood obesity: roles of diet and socioeconomic status. Community Dent Oral Epidemiol 35(6):449–458. https://doi.org/10.1111/j.1600-0528.2006.00353.x
Folayan MO, Kolawole KA, Oyedele T, Chukwumah NM, Onyejaka N, Agbaje H, Oziegbe EO, Oshomoji OV (2014) Association between knowledge of caries preventive practices, preventive oral health habits of parents and children and caries experience in children resident in sub-urban Nigeria. BMC Oral Health 14:156. https://doi.org/10.1186/1472-6831-14-156
Acknowledgements
The authors would like to thank all individuals who participated in this project; without their support and patience, this study would not be feasible. We would like to thank the children who participated in this study, and their parents/primary caregivers for providing assistance with this study.
Funding
The authors declare that no funds, grants or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by İ.Ç.Ö., G.E.Ü and P.S.E. The first draft of the manuscript was written by İ.Ç.Ö., and all authors commented on previous versions of the manuscript. İ.Ç.Ö, N.Y.A, G.E.Ü and P.S.E read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted as a master’s thesis and approval was granted by the Ethics Committee of Ankara University (Date: 02.25.2019/ No: 56786525-050.04.04/1446). Written informed consent was obtained from the parents.
Consent for publication
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient/parent/guardian/relative of the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Özel, İ.Ç., Erbaş Ünverdi, G., Serdar Eymirli, P. et al. The relationship between dental caries, dietary intake and body composition in school-age children. Egypt Pediatric Association Gaz 72, 14 (2024). https://doi.org/10.1186/s43054-024-00255-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-024-00255-5