
Abstract
Background
Internet gaming disorder (IGD) is a momentously growing issue of all ages, and medical students are not immune from the ever-increasing online gaming vogue. The Indian context is little comprehended, necessitating further research on the magnitude and variables. This study aims to determine the prevalence and risk variables of IGD among female medical students. This cross-sectional survey was conducted from March to May 2023 on 512 female (a calculated sample size) medical undergraduate students enrolled in a tertiary center located in a rural area of North India. A stratified random sampling technique was used to choose the participants. The study included a semi-structured questionnaire containing socio-demographic and personal details and gaming characteristics. It also includes a standardized tool, i.e., the Gaming Disorder and Hazardous Gaming Scale (GDHGS) to assess the outcome. The Binary logistic regression analysis was used to investigate the determinants of the dependent variable.
Results
Among the participants, only 236 (46.1%) were identified as gamers. The mean age of the gamers was 21.09 (SD = 1.65) years. Among the gamers, around 31 (13.1%) medical undergraduate students had IGD. The Binary logistic regression analysis identified a few significant determinants of IGD such as dissatisfaction with academic performance (COR = 24.8), playing internet games for more than 2 h per day (COR = 5.9), playing paid games (COR = 2.8), and playing games daily (COR = 4.99).
Conclusion
IGD is highly prevalent among professional medical college students, and its propensity is linked with poor academic performance, using paid games, and spending long hours and days on gaming. Thus, administrators should identify at-risk students and help them in seeking therapy.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Playing games online has been more accessible over the past few years as broadband internet access becomes more readily available, especially in nations with limited resources. However, excessive internet use, especially internet gaming, is making populations extremely vulnerable to a variety of physical, cognitive, emotional, and social changes, and may experience unfavorable consequences in the form of symptoms associated with internet gaming disorder (IGD) [1]. Notwithstanding its social usefulness as a source of amusement, surveys have shown that excessive internet gaming has negative effects such as sadness, anxiety, academic difficulties, poor sleep quality, and inferior real-life relationships, and have become a significant concern [2]. It was first recognized, in the DSM–5, as a mental health condition causing clinically significant distress and impairment [3], and later on, it was classified as a globally recognized mental health threat by the WHO and was incorporated into the ICD-11 in 2018 [4]. Thus, a few investigators have also concluded that IGD is an emerging mental health issue that has garnered a greater spotlight over the past few years worldwide [2, 5,6,7].
A recent systematic meta-analysis conducted on 53 studies from 2009 to 2019 found a global gaming disorder prevalence of around 3.05% [6]. A few recent studies have found a much higher prevalence in university students than in the general population ranging from 9.1 to 23% [7,8,9]. Literature has demonstrated that the heightened academic and psychological problems among medical students may trigger behavioral disorders such as anxiety and addictions through emotional regulations [10,11,12]. Thus, a higher likelihood of IGD was reported among medical students [5]. Owing to the paucity of research in a few developing nations, it was acknowledged that detailed information regarding IGD was unknown among medical students. In a recent meta-analysis, medical students from a cohort of 2236 were found to have a pooled prevalence of IGD of roughly 6.2%, with Egypt reporting the greatest prevalence at 10.9%, followed by Saudi Arabia (8.8%), Indonesia (6.1%), and India (3.8%) [13]. Such investigations among Indian medical students are just a few that have assessed that the prevalence of IGD among medical students was observed to be substantially higher, ranging from 4.25 to 30.9% [5, 14,15,16,17]. Given the higher prevalence of IGD among medical students, it is imperative to comprehend the antecedents of this problem. It has been reported in the past that low self-control, poor self-esteem, anxiety, depression, impulsivity, excess screen time, social networking site addiction, paid games, and having multiple and long-term game partners were found as the risk factors for the emergence of this disorder across countries and cultural groups [18,19,20,21]. Furthermore, a Saudi Arabia study established that a few socio-demographic and personal characteristics such as male gender, limited family support, higher family disputes, social dissatisfaction and weakness, and fear of missing out on chances were found to be linked with IGD [22]. Researchers discovered that a few gaming characteristics, such as the desire to protect one’s in-game reputation, an innate drive to defend oneself, escaping from reality, contending with other people, equalizing up by achieving gratification, and video game character growth, were additionally associated with an elevated likelihood of IGD especially among medical school graduates [18, 23]. Moreover, early identification of associated risk at an optimal time may reduce the incidence of IGD among high-risk students.
Notwithstanding this, the studies investigating these diverse variables linked with these outcomes are prominent throughout developed countries [2, 6, 12], but there remains a gap in the literature when it comes to understanding the unique risk variables in developing nations [5, 18,19,20,21]. Furthermore, considering the sole exception of the Indian sub-continent, reports of more females than males suffering from gaming problems, cultural variations do not appear to alter the gender ratio of addictive gaming behavior which appears to be male-dominated among most of the nation [24, 25]. To validate the aforementioned assertion and fill the missing link in the literature, this study incorporated the measurements of both prevalence and risk variables associated with IGD among female students solely in the Indian context.
Methods
Study design and settings
This descriptive cross-sectional study was designed and conceptualized at a tertiary care institution located in a rural area of Northern India which allows only female medical students in the MBBS (Bachelor of Medicine and Bachelor of Surgery) course and was conducted from March to May 2023. Presently, 580 undergraduate medical students are enrolled in the institute, 120 students in each professional year, and 100 students doing internships. The Institutional Ethical Committee Board granted ethical permission before the start of the study, which was consistent with the Helsinki Declarations and Ethical Committee norms. Throughout the research, the anonymity of the responses submitted by the participants was ensured.
Sample size
The sample size for the current study (n = 512) was calculated using a single-population proportion formula: Sample Size (N) = Z2 P(1-P)/d2; where Z is the confidence interval (CI) at 95%, P is the estimated prevalence (P) of IGD in an Indian survey (30.9%) [17], and d is the absolute precision which was considered to be 4%.
Study sample
The research sample entailed all (580) eligible medical undergraduate students above the age of 18 years, who were proficient in reading and writing English and were willing to provide written informed consent. These students came from all professional years, including the internship batch. Students unwilling the consent were excluded from the study.
Sampling and data collection procedure
Utilizing a stratified random sampling technique, students from each professional year (1–4) and internship batch were categorized into strata. After that, the total sample population was allocated proportionately to each stratum consisting of undergraduate and internship students. The calculated sample size (n = 512) of students was obtained by selecting 88 students from the internship batch and 106 students from each of the first four academic years and then enrolled using a computer-generated random number table. Before the distribution of the data collection sheets, one of the researchers briefed the students regarding the purpose and intent of the research, and the connotation of their replies, and was also assured about the confidentiality and anonymity of their responses and particulars. Queries, if any, were clarified before the initiation of the survey. A detachable information sheet about the survey and questionnaires were distributed by hand to the respondents before their clinical postings or lectures to record their responses under the supervision of one of the researchers, and written informed consent was taken. Departmental helpline numbers and email addresses were also shared so that they could seek professional help if required. Among 512 selected undergraduate students, around 236 (46.1%) students were recognized as gamers as they had riposted “yes” to the following statement “use of the internet for playing games in the previous year.” Thus, a total of 236 gamers were recruited for the final analysis.
Data collection measures
A semi-structured, pre-tested, and self-administered questionnaire was drafted after extensive literature research [5, 13, 15, 17, 18]. Then, a pilot study was conducted on 35 students from the same population to evaluate for any possible issues. No difficulty was reported in comprehending, recording responses, or completing the questionnaire. The final survey excluded these responses. Data collection was done using this questionnaire which had the following sections A to E: Section A had the details about the aim of the study; Section B had the written informed consent; Section C had the proforma for the socio-demographic and personal characteristics of the study participants (professional year, age, locality, family type, sibling, relationship status, sleep habits, and substance abuse such as tobacco, alcohol, and cannabis in last one year); Section D had a proforma for assessing gaming characteristics of the participants (hours spent on gaming, days spent per week in gaming, type of game, i.e., paid or non-paid, mode of gaming, preferred timing for gaming, and preferred location for gaming); Section E included GDHGS scale to monitor IGD.
Gaming Disorder and Hazardous Gaming Scale (GDGHS)
This scale was developed by Balhara et al. to assess gaming disorders and hazardous gaming. The scale consisted of six items. Items from 1 to 5 are rated on a 5-point Likert scale ranging from 0 (never) to 4 (almost daily/daily) and the 6th item response is recorded in a yes/no format to evaluate for impairment in different domains of functioning like personal, family, social, educational, occupational, and others. Scores are summed for items 1 to 4 for evaluation of gaming disorder and the 5th item response is for evaluating hazardous gaming behavior [26]. In the present study, students with GDGHS scores of ≥ 9 were considered to be having problematic internet gaming behavior. Cronbach’s alpha of GDHGS is 0.854 with a range from 0.800–0.837, and the mean inter-item correlation (mean IIC) is 0.669, illustrating strong internal reliability as well as consistency. This scale has been applied in an Indian context and has been determined to be culturally appropriate [5].
Statistical analysis
Statistical Package for Social Sciences (SPSS) version 25.0 was used for the statistical analysis of the data. The scales’ internal consistency and reliability were evaluated using Cronbach’s alpha. Mean and SD were determined for continuous data, and frequency and percentage were estimated for the nominal data. Then, univariate analysis was done on categorical data using the χ2 test or Fischer-exact test and an independent Student’s “t-test” or Mann–Whitney’s U test (continuous variables with normal and skewed distribution, respectively). The Shapiro–Wilk test was used to determine the normality of the present data. The independent risk factors were identified by using Binary logistic regression analysis (COR = crude odds ratio) after adjusting the variables found significant in univariate analysis.
Results
General characteristics (socio-demographic, personal, and gaming characteristics)
Among the 512 female undergraduate medical students who completed the questionnaire, only 236 (46.1%) students reported as gamers due to their affirmative responses to the question “use of the internet for playing internet games in the previous year.” The mean age of the participants was 21.09 (SD = 1.65) years, with the age ranging between 18 and 25 years. Students from pre-clinical and para-clinical years comprised more than half (54.6%) of the sample. Most of the gamers belonged to the nuclear family (64.4%) and did not reveal their relationship status (60.2%). Almost half of them hailed from urban backgrounds (53.4%). A greater proportion of the students had one or more siblings (94.5%). Furthermore, 71% of the participants had decent sleeping habits (> 6 h/day). A marginal proportion of gamers (1 in 5) used to consume any type of substance (tobacco, alcohol, or cannabis) in the last year. Furthermore, 1 out of 6 students who played games expressed dissatisfaction with their previous years’ academic achievement. Additionally, the average amount of time that players spent gaming was 1.97 days per week or 1.43 h per day as depicted in Table 1.
Prevalence of IGD and variations in its outcome due to influencing variables
Based on the GDHGS criteria, with the threshold score of 9 for impairment of functioning (mean (SD), 6.19 (2.71) (Table 1), 31 students (13.1%) with an average age of 20.97 (1.62) years were classified as having IGD. Univariate analysis showed that the prevalence of IGD did not vary significantly among the socio-demographic and personal characteristics except for academic achievement where a larger percentage of students in the IGD group were significantly dissatisfied with their previous years’ academic achievement (68% vs. 8%; p < 0.001) as depicted in Table 2.
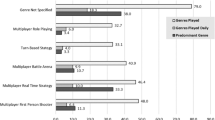
Among gaming characteristics (Table 3), the chi-squared analysis revealed that more percentages of students in the IGD group were playing games for more than 2 h (58.1% vs. 19%; p < 0.001). Additionally, those students who played games daily (39%) showed a higher dependence on IGD as compared to those who played games only on weekdays (11%). Univariate analysis found that those students who had paid for games (25.6% vs. 9.3%) were significantly (p < 0.05) higher in the IGD group.
Variables associated with the development of IGD among gamers
In the present study, the variables that were found to be statistically significantly associated with IGD on the chi-square test were also found statistically significant on bivariate analysis (Tables 2 and 3) and variables were assigned as potential risk factors of IGD. The most striking finding was that students who were unsatisfied with their academic achievement were far more likely to experience IGD (COR = 24.806; 95% CI = 9.988–61.606; p < 0.001) than academically satisfied students. Furthermore, among gaming characteristics, only three variables such as playing games for more than 2 h per day (COR = 5.893; 95% CI = 2.664–13.039; p < 0.001); playing paid games (COR = 3.405; 95% CI = 1.340–8.654; p < 0.05); and playing games on every day (weekdays and weekends) (COR = 4.998; 95% CI = 2.151–11.610; p < 0.001) were found to be significantly associated with development of IGD among medical students.
Discussion
IGD among medical students is a neoteric emerging mental health issue around the world [5, 13, 17]. To the best of our knowledge, this investigation was among the first conducted among only female medical students in the Indian context and contributed to the body of literature already available on internet gaming. This descriptive cross-sectional survey in a resource-constrained setting observed that less than half of the participating medical students were engaged in playing games, and one out of seven gamers were afflicted with IGD along with a few risk variables (dissatisfaction with academic performance, playing games daily and for more than 2 h per day, and engaging in paid games). Therefore, emphasizing these variables might aid in the use of a comprehensive preventive strategy for the development of IGD among medical students.
The present study reported the prevalence of IGD in medical students is 13.1%. In previous cross-sectional research conducted on Chinese gamers using DSM-5 diagnostic criteria, the prevalence of IGD in the last 12 months was reported among 13.6%, which nearly corroborates the findings of the current study [27]. A few research conducted globally among medical students revealed comparable results (12.2% of 294 gamers in the Indian context using a similar scale) [5]. Furthermore, compared to the current survey, other national (21%) [17] and international studies (26%) [28] of medical students discovered a significantly greater prevalence of IGD. Studies on medical students from Middle-East countries reported a lower prevalence of IGD (4.0–8.8%) than the current study [8, 29, 30]. Other studies reported from the Indian sub-continent also reported a lower prevalence (3.2–9%) of IGD than the current survey [16, 31,32,33]. These discrepancies in the prevalence of IGD might be attributable to variations in the methodology, population size, IGD-estimating questionnaires, and socio-cultural systems and attitudes of the populations being studied. Furthermore, this much higher rate of IGD observed in the present study might be due to the research-conceptualized location, i.e., a rural Indian institution where students might have a limited availability of recreational activities. Therefore, activities like getting engaged on the internet and playing internet games might be an opportunity for these students in their stressful situations in this resource-constrained setting.
In the current study population, IGD was not influenced by included socio-demographic and personal variables similar to a study done by Singh et al. [31]. This finding indicates that during their medical school, students of all ages and groups, having siblings or not, single or in a relationship, and having poor or bad sleep may have had similar gaming habits. Contrary to the present survey, multiple researchers across the globe revealed a significant association between IGD and socio-demographic and personal factors [5, 21, 34]. Among the socio-demographic and personal variables, the only variable that was significantly linked to participants’ IGD was their dissatisfaction with their academic achievement. Previously, it has been indicated that poor academic achievement among medical students is a cardinal factor for the development of psychological problems [34] and the emergence of harmful internet gaming behavior [35]. This finding is exactly in line with findings from research conducted in India [33], Hong Kong [35], and Nigeria [36]. The current research revealed that the likelihood of IGD had increased 24 times in students who were unsatisfied with their academic performance than those who did not, which was examined as the leading risk factor for gaming disorders. This finding is in concordance with research done by Suryawanshi et al. [33] on medical students which showed that poor academic scores were a significant risk factor for gaming behavior (1.9 times higher odd risk). Another study conducted on medical students in Nigeria found that students with lower academic achievement were two times at higher odds of risk for IGD which is much lower than reported in the present study [36]. Therefore, it can be assumed that students with poor academic performances have adopted a diversion motive or strategy of emotion regulation (i.e., escapism) as well as achievement-related motives, which eventually resulted in addictive behavior (internet gaming), similar to the results of several previous investigations [18, 37].
The present study investigated that the IGD proclivity had increased to 5.9 odd times in medical students who were involved in gaming for more than 2 h per day, as the second highest determinant. This finding is in line with the research conducted in the past where spending more hours in a day on gaming was identified as an independent risk factor for IGD [5, 28, 38]. A study conducted on 400 female students in the Middle East found that the odds of risk of IGD were around 5 times higher in students involved in gaming for more than 4 h per day during weekends and weekdays, aligned with the findings of current research [39]. In addition, another study conducted on 639 Indonesian medical students also revealed a significant association between long gaming hours and IGD (OR = 4.2) [40]. Another Indian institution-based survey conducted on 306 medical students found that there are 3.5 times higher odds of risk of IGD in medical students who spend a greater amount of average time on internet gaming [31], whereas another Indian research [41] conducted on university students did not corroborate the data showing relationship between gaming time and IGD in multivariate linear regression analysis. It was revealed that most of the students were playing internet games mainly on weekdays while the prevalence of IGD was higher among students who were playing games for the whole week or also on weekends. In binary logistic analysis, students getting engaged in gaming on weekdays and weekends had nearly 4.9 times higher odds of developing IGD than those who were playing games only on weekdays. In concordance with the notions of the present research, a few studies conducted in Korea [18] and Saudi Arabia [42] also established that students who were playing games daily or at maximum in a week have an increased likelihood of IGD among students. Such an association between IGD and gaming time/gaming days can be postulated through the Operant Conditioning Theory (OCT) [43]. OCT holds that behavior (in the present study—playing online games) that is repeatedly and positively reinforced may prompt a reflexive response when exposed to the reward. This response would eventually lead to habit formation and would lead to loss of control over oneself while playing games. Therefore, it would be required to be involved in long gaming hours/days to achieve the same level of rewards (tolerance), hence, increasing the probability of IGD. Therefore, it may be more advantageous to adopt intervention measures aimed at reducing internet gaming usage to prevent and manage IGD among medical students.
It has been reported that internet gamers spend real money on online games. Expenditure done by the gamers for the booming gaming market is either in the form of buying actual games or micro-transactions done in free-to-play games. And these micro-transactions are usually done for aesthetic changes in games, purchasing in-game items, and the loot boxes (rewards of uncertain value) to keep the game going and win in the game [44,45,46]. The present survey revealed that playing paid games increased the tendency of IGD by 2.9 times. In assonance with the present study, existing literature across the globe has also indicated that gaming expenditures have a strong predilection for IGD [18, 42, 46, 47]. A survey conducted in South Korea reported a 1.005 times higher risk of IGD in respondents playing paid games [18]. Similarly, a survey conducted on 5593 gamers in China found that there are 1.003–1.005 times higher odds of risk of gaming disorder in respondents having monthly monetary expenditure on games [47]. The plausible link between IGD and expenditure could be that they had to spend money to increase the duration of gaming. Also, the impulsivity trait [46] has been linked to both IGD and spending money in games, and thus, the association can be hypothesized and tested in future research.
The primary strength of the present investigation is that it ranks as one of the very few among female students studying medicine in rural India to look into IGD using standardized and validated tools with very good internal reliability along with the identification of several significant covariates. Therefore, the results were remarkable and have substantial therapeutic ramifications for minimizing the risk of IGD among medical students. Furthermore, a high response rate makes it possible to perform pertinent statistical analysis on the many confounders that were included in the research. Lastly, IGD was also analyzed separately for each batch in the present study.
This study has various limitations, some of which suggest areas for further investigation. Firstly, it is a cross-sectional study with a sample population having limited representation as it is a single-center study with only female medical students in a rural institution; hence, findings could not be generalized and extrapolated to both genders. Thus, in the future multi-centric studies from both rural and urban institutions can be planned. Secondly, this study design could not establish a causal relationship between IGD and the determinants; therefore, longitudinal studies can be organized to establish this link. Finally, self-administered questionnaires were used which might have resulted in recollection and response bias. Hence, it is recommended to use several kinds of measurements, such as behavioral assessments and comprehensive interviews.
Conclusion
The present research suggested that a significant proportion of female medical undergraduate students are suffering from IGD. Also, the quintessence of the study is that it has reported the recent prevalence of IGD and determinants associated with it in a remotely located medical institution. Given the high prevalence, medical faculty and administrators should identify students at risk for IGD, and help them in seeking treatment. Awareness about IGD could be increased through lectures and campaigns. Also, recreational activities could be organized by the institutions regularly. Regular efforts should also be made to dispel the stigma associated with the therapy.
Availability of data and materials
The datasets that were generated during and/or analyzed during the current study are available from the corresponding author on request.
Abbreviations
- COR:
-
Crude odd ratio
- DSM-5:
-
Diagnostic and Statistical Manual-5
- GDHGS:
-
Gaming Disorder and Hazardous Gaming Scale
- ICD-11:
-
11Th revision of the International Classification of Diseases
- IGD:
-
Internet gaming disorder
- SD:
-
Standard deviation
- WHO:
-
World Health Organization
References
Wang Q, Ren H, Long J, Liu Y, Liu T (2019) Research progress and debates on gaming disorder. Gen Psychiatry 32:e100071
Wong HY, Mo HY, Potenza MN, Chan MNM, Lau WM, Chui TK et al (2020) Relationships between severity of internet gaming disorder, the severity of problematic social media use, sleep quality, and psychological distress. Int J Environ Res Public Health 17:1879
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (DSM-5). American Psychiatric Association, Arlington, VA
World Health Organization (2019) The ICD-11 classification of mental and behavioural disorders: diagnostic criteria for research. World Health Organization, Geneva
Garg S, Kharb A, Verma D, Antil R, Khanna B, Sihag R et al (2023) The mediating role of sleep quality on the relationship between internet gaming disorder and perceived stress and suicidal behaviour among Indian medical students. Gen Psychiatry 36:e100997
Stevens MW, Dorstyn D, Delfabbro PH, King DL (2021) The global prevalence of gaming disorder: a systematic review and meta-analysis. Aust NZ J Psychiatry 55:553–568
Khan S, Narasannavar A, Angolkar M (2021) Prevalence of internet gaming disorder among engineering students of Engineering Institute of Belagavi City, Karnataka, India. Int J Community Med Public Health 9:175–180
Khrad H, Marhoomi A, Alkhiri A, Al-Shamrani A, Bajabir D, Mosli M (2022) Prevalence of internet gaming disorder among Saudi Arabian university students: relationship with psychological distress. Heliyon 8:e12334
Bisht B, Goyal SK, Kaur N (2021) Prevalence of internet gaming disorder (IGD) in university students and its relationship with depression. Indian J Forensic Med Toxicol 14:921–927
Garg S, Chauhan A, Sharma D, Sharma A, Singh S (2022) Coping styles to vitiate the risk of psychological morbidities among pre/paraclinical and clinical undergraduate medical students: a comparative cross-sectional study in India. Middle East Curr Psychiatry 29:e29
Kharb A, Garg S, Yadav A, Yadav E, Kumar S (2023) Covariates associated with mental health problems faced by undergraduate medical students undergoing competency-based medical education at a rural institution in North India. Indian J Soc Psychiatry 2024;40:153–63.
Quek TT, Tam WW, Tran BX, Zhang M, Zhang Z, Ho CS et al (2019) The global prevalence of anxiety among medical students: a meta-analysis. Int J Environ Res Public Health 16:2735
Chiang CLL, Zhang MWB, Ho RCM (2022) Prevalence of internet gaming disorder in medical students: a meta-analysis. Front Psychiatry 12:e760911
Karthikeyan E, Norman P, Thirunaaukarasu D, Geetha M, Kumar H (2021) Relationship between internet gaming disorder and insomnia among medical college students of Kanchipuram district, Tamil Nadu. Int J Community Med Public Health 8:4786–4791
Bhaskar R, Babu BP, Sebastian SR (2021) Internet gaming disorder among medical students: an observational study from Central Kerala, India. J Curr Res Sci Med 7:114–118
Aggarwal A, Pandian JD (2019) Internet gaming disorder in undergraduate medical and dentistry students. CHRISMED J Health Res 6:237–241
Singh A, Shree T, Kumar P (2022) Internet gaming disorder and its harmful health effects among the medical students in a tertiary care teaching hospital. MAMC J Med Sci 8:33–39
Rho MJ, Lee H, Lee TH, Cho H, Jung DJ, Kim DJ et al (2017) Risk factors for internet gaming disorder: psychological factors and internet gaming characteristics. Int J Environ Res Public Health 15:e40
Macur M, Pontes HM (2021) Internet gaming disorder in adolescence: investigating profiles and associated risk factors. BMC Public Health 21:e1547
Ropovik I, Martoncik M, Babincak P, Baník G, Vargova L, Adamkovic M (2023) Risk and protective factors for (internet) gaming disorder: a meta-analysis of pre-COVID studies. Addict Behav 139:e107590
Liao Z, Huang Q, Huang S, Tan L, Shao T, Fang T et al (2020) Prevalence of internet gaming disorder and its association with personality traits and gaming characteristics among Chinese adolescent gamers. Front Psychiatry 11:e598585
Unal E, Gokler ME, Turan S (2022) An evaluation of the factors related to internet gaming disorder in young adults. Addict Health 14:279–287
Beard CL, Haas AL, Wickham RE, Stavropoulos V (2017) Age of initiation and internet gaming disorder: the role of self-esteem. Cyberpsychol Behav Soc Netw 20:397–401
Rajanna SH, Sharma MK, Palanichamy TS (2016) Exploration of technology use pattern among teenagers and its relationship with psychological variables. ASEAN J Psychiatry 17:239–249
Su W, Han X, Yu H, Wu Y, Potenza MN (2020) Do men become addicted to internet gaming and women to social media? A meta-analysis examining gender-related differences in specific internet addiction. Comp Human Behav 113:106480
Balhara YPS, Singh S, Saini R, Kattula D, Chukkali S, Bhargava R (2020) Development and validation of gaming disorder and hazardous gaming scale (GDHGS) based on the WHO framework (ICD-11 criteria) of disordered gaming. Asian J Psychiatry 54:e102348
Yu Y, Yang X, Wang S, Wang H, Chang R, Tsamlag L et al (2020) Serial multiple mediation of the association between internet gaming disorder and suicidal ideation by insomnia and depression in adolescents in Shanghai. China BMC Psychiatry 20:460
Severo RB, Soares JM, Affonso JP, Giusti DA, de Souza Junior AA, de Figueiredo VL et al (2020) Prevalence and risk factors for internet gaming disorder. Braz J Psychiatry 42:532–535
Almigbal TH, Alrasheed AA, Almutairi ES, Alrehaili RA, Alzahrani AM, Alhassan NA et al (2022) Relationship between medical students’ perceived stress and gaming behavior at King Saud University. Biomed Res Int 2022:e3220042
Al-Asqah MI, Al-Orainey AI, Shukr MA, Al-Oraini HM, Al Turki YA (2020) The prevalence of internet gaming disorder among medical students at King Saud University, Riyadh, Saudi Arabia. A cross-sectional study Saudi Med J 41:1359–1363
Singh S, Dahiya N, Singh AB, Kumar R, Balhara YPS (2019) Gaming disorder among medical college students from India: exploring the pattern and correlates. Ind Psychiatry J 28:107–114
Shrestha MV, Shrestha N, Sharma SC, Joshi SK (2020) Gaming disorder among medical college students during COVID-19 Pandemic Lockdown. Kathmandu Univ Med J 18:48–52
Suryawanshi DM, Rajaseharan D, Venugopal R, Mathew M, Joy A, Goyal R (2021) The association between gaming practices and scholastic performance among medical students in India: case-control study. JMIR Med Educ 7:e22235
Garg S, Chauhan A, Singh S, Bansal K (2022) Epidemiological risk factors of suicidal behavior and effects of the components of coping strategies on suicidal behavior in medical students: an institution-based cross-sectional study in India. J Neurosci Rural Pract 13:382–392
Wang CW, Chan CL, Mak KK, Ho SY, Wong PW, Ho RT (2014) Prevalence and correlates of video and internet gaming addiction among Hong Kong adolescents: a pilot study. Sci World J 2014:e874648
Chime OH, Chinawa AT, Nduagubam OO (2021) Prevalence and predictors of gaming disorder among undergraduate medical students in Enugu, Nigeria: video game addiction in focus. Niger J Med 30:615–619
Zanetta Dauriat F, Zermatten A, Billieux J, Thorens G, Bondolfi G, Zullino D et al (2011) Motivations to play specifically predict excessive involvement in massively multiplayer online role-playing games: evidence from an online survey. Eur Addict Res 17:185–189
Wang Y, Liu M, Nogueira OCBL (2023) Prevalence and risk factors of internet gaming disorder under the COVID-19 pandemic among university students in Macao. SAGE Open Nurs 9:e23779608231158160
Bumozah HS, Al-Quwaidhi AJ, Al-Ghadeeb R (2023) Prevalence and risk factors of internet gaming disorder among female secondary school students in Al-Ahsa. Kingdom of Saudi Arabia Cureus 15:e40375
Siste K, Hanafi E, Sen LT, Wahjoepramono POP, Kurniawan A, Yudistiro R (2021) Potential correlates of internet gaming disorder among Indonesian medical students: cross-sectional study. J Med Internet Res 23:e25468
Ansari M, Patel NM, Mahida AN, Phatak AG, Prabhakaran A, Varma JR (2022) Correlates of internet gaming among violent and nonviolent gamers and comparison of their psychological well-being with non-gamers in a university student population. Indian J Psychiatry 64:98–101
Alhamoud MA, Alkhalifah AA, Althunyan AK, Mustafa T, Alqahtani HA, Awad FAA (2022) Internet gaming disorder: its prevalence and associated gaming behavior, anxiety, and depression among high school male students, Dammam, Saudi Arabia. J Fam Community Med 9:93–101
de Miguel A, Yamauchi R, Simoes V, da Silva CJ, Laranjeira RR (2015) From theory to treatment: understanding addiction from an operant behavioral perspective. J Modern Edu Rev 5:778–787
Tomic NZ (2018) Economic model of microtransactions in video games. J Econ Sci Res 1:17–23
Zendle D, Meyer R, Cairns P, Waters S, Ballou N (2020) The prevalence of loot boxes in mobile and desktop games. Addiction 115:1768–1772
Costes JM, Bonnaire C (2022) Spending money in free-to-play games: sociodemographic characteristics, motives, impulsivity, and internet gaming disorder specificities. Int J Environ Res Public Health 19:e15709
Liao Z, Chen X, Huang S, Huang Q, Lin S, Li Y et al (2023) Exploring the associated characteristics of Internet gaming disorder from the perspective of various game genres. Front Psychiatry 13:e1103816
Acknowledgements
We are grateful to all the medical students who participated in the study.
Funding
None.
Author information
Authors and Affiliations
Contributions
AK, SG, and VS conceived the idea of this study. DS and RB collected the data, and AK, SG, and VS analyzed the data. SG and AK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript. SG, AK, and VS are responsible for the overall supervision of this project.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The informed consent was obtained from all the participants and the study protocol was approved by the institute's ethical board/committee before the start of data collection. This institute-based original study was approved by the Ethical Committee.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kharb, A., Garg, S., Sharma, V. et al. Determinants associated with internet gaming disorder in female medical students: a logistic regression analysis using a random sampling survey. Middle East Curr Psychiatry 31, 49 (2024). https://doi.org/10.1186/s43045-024-00438-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-024-00438-1