
Abstract
Background
Poor adherence to health behaviors is one of the considerable challenges among drug users. This issue is especially noticeable among people who use injection methods for consumption, which increases the possibility of contracting HIV and hepatitis B and C. Therefore, it seems that adopting appropriate intervention approaches focusing on all dimensions of health-related behaviors to promote health behaviors is considered. As a result, in the present study, the effectiveness of a comprehensive educational program on promoting health behaviors and awareness of HIV, hepatitis B, and hepatitis C in drug users was investigated.
Methods
This pretest–posttest quasi-experimental study was performed. The participants were 81 men with substance use disorders residing in a rehabilitation center. The participants took part in four training workshops. The workshops focused on mental health, awareness of HIV, and hepatitis B and C with learner-centered approaches.
Results
According to the results, the mean score of the health behavior scale in the participants after receiving the intervention of the comprehensive program increased significantly (P < .001). Additionally, the analysis showed that 1 month after the end of the intervention, there was a significant increase in the AIDS, hepatitis B, and hepatitis C scale scores compared to before the intervention (P < .001).
Conclusion
Considering the adverse consequences of drug use, especially in users without social support, the need for education as a cost-effective approach to prevent diseases transmitted through high-risk behaviors such as HIV, and hepatitis B and C is considered a basic necessity.
Similar content being viewed by others


Background
According to the United Nations Office on Drugs and Crime report in 2023, the number of drug users has reached 39.5 million people in a way that, over 10 years, there was a 45% increase [1]. Drug use and related problems are considered as public health issues with extensive destructive consequences for the individual, family, and society [2].
One of the most common challenges among drug users is poor adherence to health behaviors. Health behaviors include any action people take to improve their physical, social, emotional, and mental health [3]. Based on the conducted studies, people suffering from drug use report serious problems related to their sleep, mental health, and nutrition [4,5,6].
Using injection as a way of using drugs is regarded as a risky behavior among drug users such that global data estimated injector users up to 13.2 million people in a year, which is 18% greater in number compared to previous statistics. On the other hand, half of these people suffer from hepatitis C, 14 million people with HIV, and 1.2 million people suffer from both viruses [7]. Transferred viruses via blood, such as HIV, hepatitis C, and hepatitis B (HBV), are the most typical virus pathogens among injector users. These infections are severely accompanied by chronic hepatic diseases such as alcoholic liver disease, fulminant hepatic failure, hepatocellular carcinoma in HBV and HCV infections, and severe diseases in HIV infection [8, 9]. In this regard, the results of a systematic study showed that Iran had the highest spread of HIV, with 11.0% statistics in injector users among the three countries: Iran, Pakistan, and Afghanistan. Additionally, the spread of HCV in Iran was 47.7% higher than that in the other two countries. Overall, HIV, HBV, and HCV spread is much higher among drug users in the Iranian community. Thus, making people aware of the risks of HIV and HCV spread via shared syringes seems necessary [10].
However, today, there are various ways to boost health behaviors; nevertheless, education and training are primary tools for presenting health behaviors [3]. Applying educational interventions to observe behaviors related to lifestyle can boost health conditions by strengthening self-efficiency, empowering factors, and changing attitudes [11]. Furthermore, according to The Statement on Monitoring the Results of Future National Poll About Drug Use, the requirement to convey extensive research on epidemiology, development, and devising interventions, testing, and evaluating policymaking packages on addiction is regarded as a necessity in healthcare [12].
In sum, considering the widespread outcomes of chronic drug use in different ways, ignoring the issue can lead to high levels of mental and cognitive inability as well as early death due to poisoning, infection by infectious diseases such as HIV, and improper sanitation. Therefore, drug use disorders are categorized as sanitary challenges for communities. On the other hand, since the number of conducted surveys on these individuals as a high-risk group in the HIV, HBV, and HCV transferring chain in our country, Iran, especially in health education, is considerably limited, most studies have been dedicated to epidemiologic investigations. Then, it is expected that the results of the present study will create helpful insights into the planning and effectiveness of educational programs in high-risk groups. Hence, our aim in carrying out this study was to investigate the effectiveness of a comprehensive educational program on health behaviors and awareness of HIV, hepatitis B, and hepatitis C among drug users.
Methods
Design
This quasi-experimental study evaluated the effectiveness of a comprehensive educational program on improving health behaviors and awareness of HIV, hepatitis B, and hepatitis C among drug users residing in a rehabilitation center.
Participants
The participants were 81 men with substance use disorders residing in a rehabilitation center. The sample size in the present study was determined using NCSS software, type one error 0.05, and 80% power based on an article by Bastami et al. (2015), as well as the average of changes before and after the intervention in an 80-person group [13]. One of the ways to increase the power of studies is to use a large sample size. However, due to operational and resource limitations, it is usually attempted to use the results of previous studies to estimate the sample required to achieve adequate power before starting a study [14]. Therefore, in this research, considering the power of 80%, the sample size was estimated to be 81 people. In this regard, we increased the number of samples to 100 due to the possibility of missing data.
Sampling
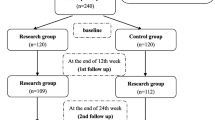
The participants making up the sample for this study were selected using a random sampling method from among the list of individuals residing in a rehabilitation center and considering entrance criteria. In this survey, simple random sampling was used. Each participant qualified to enter the investigation according to the entrance criteria, which were being an adult, having a drug use disorder based on DSM5 or the psychotherapist diagnosis, tendency for participation, and having reading and writing literacy dedicated to a code. Finally, 100 participants were selected using a computer-based randomization method to enter the study. To ensure unbiased and random allocation of subjects to receive the intervention, we implemented a computerized random number table to assign a unique 3-digit code to each participant who met the inclusion criteria. The total number of participants in the study was 167. To select a sample of 100 participants, we chose the codes along a column until we reached 100 samples. It is worth noting that we accepted any codes that were smaller than 167. By utilizing this method, we aimed to minimize the potential for selection bias. Considering the possible drops in the number of participants during the study process, 20 people were added to the sample.
Study procedure
Initially, all the participants completed an informed written consent letter, a demographic information questionnaire, the International AIDS Questionnaire, the awareness of hepatitis B and C questionnaire, and the health behaviors questionnaire. The exclusion criteria were suffering from severe cognitive, learning, and psychiatric disorders of any kind.
The participants took part in four training workshops in groups, where the first session was dedicated to becoming familiar with transmissible infectious diseases via high-risk behaviors such as HIV, hepatitis B, and hepatitis C. At the beginning of the workshop, the researcher explained receiving training on healthcare and infectious diseases, the process of the disease, contagion methods, disease symptoms, preemptive considerations, and treatments using educational videos and multimedia content. Then, the participants’ ideas were heard through group discussions. Last, at the end of the session, the participant’s questions were answered. Additionally, treatment health centers that support such patients and specialize in providing counseling treatment services to people suffering from social harm were introduced.
The second session included training on sleep health and healthy nutrition. In this session, the educational content was presented through lectures and using videos and multimedia content initially. Afterward, the participants had a group discussion and pointed out their ideas. At the end of the workshop, the participants asked questions and received answers.
The third session was about physical education and sports. This session was fully practical and provided the participants with exercise programs based on their characteristics. Moreover, in this session, the participants’ abilities and skills in sports and physical education were identified by a trainer.
The fourth session was about life skills and mental health. In this workshop, the participants practiced life skills through role-play, practice, and repetition. Similarly, at the end of the session, the supporting, welfare, and treatment centers and institutes were introduced, among which the individuals could refer to considering their specific issues to receive the necessary services.
Finally, 1 month after the last educational session, the participants, who made up 81 people (19 people dropped out of this intervention), completed the questionnaires again.
Data gathering tools
The data gathering tools in this investigation consisted of an individual demographic questionnaire, an International AIDS Questionnaire (IAQ), an informative questionnaire on hepatitis B and hepatitis C, and a health behaviors questionnaire.
Demographic information questionnaire
This questionnaire included individual information (age, marital status, occupation) as well as disease-related information (drug use duration/the type of used drug/the starting age).
International AIDS questionnaire
The International AIDS Questionnaire [15] contains 18 questions about HIV devised to evaluate four different dimensions of awareness and attitude toward AIDS. They are myths and misconceptions about HIV contagion (questions 1–7), attitudes about people with HIV (questions 8–12), people’s statements related to comprehending the risk of infection with AIDS (questions 13–15), and awareness of AIDS-related facts (questions 16–18). The answers were scored based on a 5-point Likert scale ( (1) strongly disagree, (2) disagree, (3) neither agree nor disagree, (4) agree, (5) strongly agree). For each choice, there was a Likert point from (1) strongly disagree to (5) strongly agree, in a way that a higher score per choice shows a higher level of awareness and attitude. For four reversed questions that were 10–16-17–18, the points will be reversed; therefore, the points will be in the 18–90 range. In a study by Eskandar et al. (2013) [16], the Cronbach’s alpha points were reported as follows: myths and misconceptions scale, 0.79; individual risks, 0.78; attitudes, 0.78; and spread and infection, 0.60, and for the whole test 0.80. This scale has been translated into different languages. In the present study, the Persian version of the scale, which was psychometrically tested by Eskandar et al. (2013) on Iranian society, was used.
The awareness of hepatitis B and hepatitis C checklist
The questionnaire [17] contains 58 questions (17 questions on hepatitis B, 6 questions on hepatitis C, and 35 questions on HIV) to evaluate the patients’ primary knowledge of diseases, ways of infection and spread, awareness of risks, reporting behaviors, and prevention. The participants answer the questions by yes/no and I don’t know. In this way, random answers will be avoided. The questionnaire was evaluated in terms of content, clarity, and readability by 10 participants before applying the intervention. In this study, the questions in the two parts of hepatitis B and hepatitis C will be used. This questionnaire has Persian and English versions.
Health behavior questionnaire
This questionnaire was developed by Alavi (2018) (Alavi, 2018) and has 43 questions. The questionnaire includes seven variables: welfare, daily hygiene, nutrition, substance use, risky behavior, environmental dangers, and medical healthcare. The questions in this questionnaire are scored based on a 5-point Likert scale (always 5, often 4, sometimes 3, rarely 2, and never 1). This questionnaire is in Persian and has been psychometrically tested in Iranian society. Alavi (2018) obtained the content validity of the questionnaire at 0.83 and calculated the reliability and its variables using Cronbach’s alpha as 0.91.
Statistical analysis
Data were analyzed using descriptive and inferential statistical methods in SPSS 22 software. The value of P < 0.05 was considered statistically significant. The analysis of the data consisted of two sections: descriptive and inferential. The descriptive section presented the mean and standard deviation, frequency and percentage, and minimum and maximum values. In the inferential part, the paired samples t-test was used to compare the mean of a quantitative factor before and after the intervention.
Results
In the present study, 81 male drug users residing in a rehabilitation center participated. The participants’ age range was 39.01 ± 10.78. The mean duration of drug use was 16.17 ± 9.95, and the mean age at the start of consumption was 20.99 ± 7.36 among the participants; according to the reports, the youngest age was 11, and the oldest was 50. Additionally, most participants had high school education 59.3%, employed 50.6%, and married 45.7%. Most participants use more than one type of drug. In addition, although most of the participants did not report any psychiatric disorder records, 49.4% of them complained about a psychiatric disorder (Tables 1 and 2).
Also, the results of the study showed that there was a meaningful significant difference between health behaviors before and after the intervention in a way that the score was reported (132.56 ± 30.36) before and (145.65 ± 29.23) after the intervention (p: 0.000). Among the subscales of health behaviors, a meaningful significant difference was reported for six subscales of welfare (p: 0.000), daily hygiene (p: 0.000), drug use (p: 0.006), risky behavior (p: 0.000), environmental dangers (p: 0.000), and medical healthcare (p: 0.000) before and after the intervention. However, there were no significant differences reported for the subscale nutrition before and after the intervention (p: 0.334) (Table 3).
Other results of the study that have been presented based on the paired t-test revealed that there was a meaningful significant difference between the total score of AIDS before and after the intervention (p = 0.000) in that the mean score was reported 53.82 ± 8.86 before and 69.06 ± 7.82 after the intervention. In investigating the subscales, for each of the four subscales of myths and misconceptions about AIDS (p: 0.000), attitudes toward people with AIDS (p: 0.044), people’s remarks related to perceiving the risk of AIDS (p: 0.040), and awareness of facts related to AIDS (p: 0.000), a meaningful significant difference was reported before and after the intervention. However, the least level of changes was for the attitudes dimension, and most changes were seen for the misconception dimension (Table 4).
Moreover, according to another set of results obtained from this study, in both awareness of hepatitis B and awareness of hepatitis C subscales, the mean score of the participants showed a meaningful significant difference before and after the intervention (p = 0.000), in a way that, in hepatitis B, the mean score was 10.17 ± 3.545 before the intervention and increased up to 13.62 ± 3.87 after the intervention. Similarly, the mean score for hepatitis C was 2.49 ± 1.33 before the intervention and then increased to 3.85 ± 1.351 after the intervention (Table 5).
Discussion
In the present study, the researchers attempted to evaluate the effectiveness of a comprehensive educational program on health behaviors and awareness of HIV, hepatitis B, and hepatitis C in drug users. The outcomes of the study indicated that health behaviors in the samples of this study increased remarkably after presenting the comprehensive educational program compared to the number before applying the intervention. Additionally, in investigating the scales, a meaningful significant difference was reported before and after the intervention for the six subscales of welfare, daily hygiene, drug use, risky behavior, environmental dangers, and medical healthcare. For the subscale of nutrition, there was no meaningful significant difference. However, the mean score for this subscale increased after the intervention.
In this regard, a study by Limberger indicated that training social skills will lead to a meaningful increase in avoidance skills and expressing negative feelings and the quality of life (psychological realm). It will remarkably decrease depression symptoms and improve people’s quality of life (environmental realm) among drug users [18]. In addition, training psychological skills can enhance social skills in vulnerable groups [19]. Thus, in the present educational program, education related to social skills has been considered because social skills are among the significant criteria for mental health. They are categorized as a part of the activities that can effectively improve health behaviors.
In addition, the results of a study by Ashdown-Franks revealed that the advantages of positive mental health aiming at improving a healthy lifestyle by exercising in people with psychological disorders and alcohol use are considerable [20]. The potential advantages of integrating physical activities related to addiction treatment are various and include physical health and mental health. However, the researcher has specified that in people with SUD, adherence to physical activity programs and enjoying full privileges of many health-related activities may not be fully achieved due to the recurrent nature of addiction and its psychological problems [21]. Nevertheless, in the present program, we attempted to discover the participants’ sports capabilities and enhance the interest and motivation level among them using different specialized techniques by the sports trainer.
Additionally, in this regard, the results of a study carried out in Iran showed that training sleep health can effectively improve the quality of sleep and decrease depression, stress, and anxiety in patients with substance use disorders [22]. On the other hand, since drug users, particularly chronic users, are exposed to weaker health conditions and have less access to healthcare services due to social factors such as rejection and fear of social stigma, it is essential to provide education in line with increasing awareness [23].
Considering that there were no meaningful changes in the nutrition dimension, and since various infrastructural factors form an individual’s diet habits, customs, beliefs, and access to food, initiating changes in wrong diet beliefs and reaching nutritional health call for a greater level of intervention. Therefore, we recommend conducting specialized studies to identify factors affecting food health and drug users’ nutrition.
Other results of the study showed that in the knowledge and attitude toward AIDS scales, there was a meaningful difference before and after the intervention, in a way that 1 month after the intervention, a remarkable increase was reported in the total score, as well as the dimensions: myths and misconceptions about AIDS, attitudes about people infected by HIV, the person’s remarks about perceiving the risk of AIDS, and awareness of facts related to AIDS. These outcomes indicate that a comprehensive program based on teaching hygiene has a considerable effect on knowledge and attitudes toward AIDS in drug users. Consequently, the results of a study by Chizoba revealed that applying educational intervention by healthcare service providers led to an increase in knowledge of HIV and a decrease in risky behaviors among youth [24]. Additionally, Jiao pointed out in their research that promoting educational campaigns among drug users, specifically the elders, women, and those with lower education, is of great significance [25]. The results of a pilot study aiming at investigating the effect of an educational intervention using an application on improving knowledge toward HIV revealed that HIV educational intervention is accompanied by considerable stable advances in knowledge on HIV contagion, and high-risk behaviors in the vulnerable group made up of people with drug use. Therefore, since the continuation of the drug use epidemic, urgent attempts seem necessary to slow down the spread and contagion of HIV among people with opioid use disorder (OUD). Hence, we can claim that healthcare educational interventions may present a more reasonable approach to dealing with these risks [26]. Moreover, the results of an intervention study by Khezri et al. revealed that education can improve street children’s knowledge and attitudes toward HIV. Such improved knowledge and attitude can protect them against risky behaviors because knowledge is a vital necessity for changing attitudes and taking protective actions against risky behaviors [27] .The results obtained from the mentioned study are in line with the outcomes of the present study that signal the importance and effectiveness of education on improving awareness toward HIV.
Other results noted that educational intervention on awareness of hepatitis B and C also has had considerable effectiveness. Thus, the scores for both the hepatitis B and hepatitis C dimensions increased meaningfully after receiving the intervention. In this regard, the results of a study revealed that expanding the education related to employees and caretakers can lead to the improvement of tests and the number of referrals, which, in effect, is necessary for strengthening treatments for the two diseases [28]. Additionally, Mahmoudi et al., in their investigation, indicated that health belief model-based education can enhance acceptance levels for preventive behaviors for hepatitis B in healthcare volunteers [29]. The outcomes of another study conducted by Maqsood emphasized that to eliminate hepatitis B and C, appropriate awareness of the reasons and preventive methods need to be implemented. Sufficient knowledge of HBV and HCV, the ways of their contagion, symptoms of the diseases, and awareness of treatments and available vaccines are crucial for encouraging a desirable attitude toward seeking a cure and preventing the spread of infection [30]. The outcomes of this study are in line with the results of the present study that explicitly indicate the importance of presenting educational intervention to improve knowledge and awareness toward hepatitis B and C.
Because drug users are mainly prone to HIV/HCV and drug overuse, their communities can successfully spread knowledge, strategies, and harm-decreasing norms for those exposed to danger. Thus, preventive programs, along with empowering drug users, can unite them to fight HIV/HCV and facilitate health-protective actions [31].
Hygiene-improvement behaviors are defined as any activity done to improve, maintain, or regain health, whether such behavior is specifically oriented to achieve the purpose [32]. Therefore, a healthy life and increased welfare for people of all ages are solely achieved by improving health through hygiene-improvement programs and public cooperation [32, 33]. The results of a study also revealed that most drug users are reported to have low or medium literacy levels. Then, the participants with lower literacy levels have a weak quality of life and mental health [34]. It seems that it is necessary to take hygiene-improvement measures to prevent other harmful behaviors, such as the side effects of drug use. In this regard, multilateral interventions related to changing health behaviors target risk factors and, in essence, are considered promising methods for lifelong health improvement. This approach provides evidence that changing lifestyles can enhance self-efficacy for improving health-related behaviors [35].
Conclusion
Overall, the results of the present study highlight the effectiveness of a comprehensive educational program concentrating on different dimensions of health behaviors and healthy lifestyles. Considering the adverse consequences of drug use, especially in users without social support, the need for education as a cost-effective approach to prevent diseases transmitted through high-risk behaviors such as HIV, hepatitis B, and C is considered a basic necessity.
Limitations of the study
The main limitation of the present study was the lack of a control group. This limitation was due to the residence conditions of the participants. Since the participants resided in a shared location, it was possible to share information between the two groups. Then, it is recommended that other researchers utilize a controlled trial design to evaluate the effectiveness of the comprehensive intervention.
Availability of data and materials
The datasets during the current study will be available upon reasonable request. The author from whom data can be accessed: Zakiye Ghelbash, PhD Student. Department of Nursing, School of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran. Email: z.ghelbashp@yahoo.com.
Abbreviations
- AIDS:
-
Acquired immunodeficiency syndrome
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus
- HIV:
-
Human immunodeficiency viruses
- SUD:
-
Substance use disorders
- OUD:
-
Opioid use disorder
- UNODC:
-
The United Nations Office on Drugs and Crime
References
UNODC (2023) World Drug Report, The United Nations Office on Drugs and Crime
Davis JP et al (2018) Substance use outcomes for mindfulness based relapse prevention are partially mediated by reductions in stress: results from a randomized trial. J Subst Abuse Treat 91:37–48
Hayden J (2022) Introduction to health behavior theory. Jones & Bartlett Learning: The United States
Mahboub N, Rizk R, Karavetian M, de Vries N (2021) Nutritional status and eating habits of people who use drugs and/or are undergoing treatment for recovery: a narrative review. Nutr Rev 79:627–635. https://doi.org/10.1093/nutrit/nuaa095
Valentino RJ, Volkow ND (2020) Drugs, sleep, and the addicted brain. Neuropsychopharmacology 45:3–5
SAMHSA (2020) Key substance use and mental health indicators in the United States: results from the 2019 National Survey on Drug Use and Health, Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration.
UNODC (2022) World Drug Report, The United Nations Office on Drugs and Crime.
Asif A, Ayub S, Komal A, Noor S, Jalal U (2019) Prevalence of human immunodeficiency virus and hepatitis (B & C) among drug users in a tertiary care public hospital. Pak J Med Sci 35:459–463. https://doi.org/10.12669/pjms.35.2.500
Sanyaolu A, Badaru O, Okorie C, Marinkovic A, Ayodele O (2020) The prevalence of hepatitis B, C and HIV among injection drug users in the USA. J Microbiol Microb Infect 2:56–62
Shayan SJ, Nazari R, Kiwanuka F (2021) Prevalence of HIV and HCV among injecting drug users in three selected WHO-EMRO countries: a meta-analysis. Harm Reduct J 18:59. https://doi.org/10.1186/s12954-021-00505-4
Solhi M et al (2020) The effect of educational intervention on health-promoting lifestyle: intervention mapping approach. J Educ Health Promot 9:196. https://doi.org/10.4103/jehp.jehp_768_19
Johnston L et al (2020) Monitoring the future national survey results on drug use, 1975–2019: overview, key findings on adolescent drug use, Institute for Social Research The University of Michigan
Bastami F, Mostafavi F, Hassanzadeh A (2015) Effect of educational intervention on knowledge, perceived benefits, barriers and self-efficacy regarding AIDS preventive behaviors among drug addicts. J Educ Health Promot 4:90. https://doi.org/10.4103/2277-9531.171804
Suresh K, Chandrashekara S (2012) Sample size estimation and power analysis for clinical research studies. J Hum Reprod Sci 5:7–13. https://doi.org/10.4103/0974-1208.97779
Davis C, Sloan M, MacMaster S, Hughes L (2007) The International AIDS Questionnaire—English version (IAQ-E) assessing the validity and reliability. J HIV/AIDS Prev Child Youth 7:29–42
Escandary N, Alipour Z, Lamyian M, Ahmaritehran H, Hajizadeh E (2013) Validity and reliability of the international AIDS questionnaire for Iranian student population. J Arak Univ Med Sci 15:1–12
Dehghani B, Dehghani A, Sarvari J (2020) Knowledge and awareness regarding hepatitis B, hepatitis C, and human immunodeficiency viruses among college students: a report from Iran. Int Q Community Health Educ 41:15–23. https://doi.org/10.1177/0272684x19896727
Limberger J, Andretta I (2022) Effects of social skills training for drug users under treatment. Psico-USF 27:211–223
Ghelbash Z, Zarshenas L, Dehghan Manshadi Z (2021) A trial of an emotional intelligence intervention in an Iranian residential institution for adolescents. Clin Child Psychol Psychiatry 26:993–1002
Ashdown-Franks G et al (2020) Exercise as medicine for mental and substance use disorders: a meta-review of the benefits for neuropsychiatric and cognitive outcomes. Sports Med 50:151–170
Abrantes AM, Blevins CE (2019) Exercise in the context of substance use treatment: key issues and future directions. Curr Opin Psychol 30:103–108. https://doi.org/10.1016/j.copsyc.2019.04.001
Barati AA, Zhoolideh M, Moradi M, Sohrabi Mollayousef E, Fürst C (2022) Multidimensional poverty and livelihood strategies in rural Iran. Environ Dev Sustain 24:12963–12993
Aldridge RW et al (2018) Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. The Lancet 391:241–250
Chizoba A, Chineke H, Adogu P, Nwafia A, Chizoba C (2021) Effects of peer and provider-based education interventions on HIV/AIDS knowledge and behaviour-risk among in-school adolescents in Ebonyi State, Nigeria. Asian J Med Health 18:100–114
Jiao K et al (2022) Drug users’ awareness of and willingness to use HIV non-occupational post-exposure prophylaxis (nPEP) services in China: a mixed methods study. BMC Infect Dis 22:1–10
Ochalek TA, Heil SH, Higgins ST, Badger GJ, Sigmon SC (2018) A novel mHealth application for improving HIV and hepatitis C knowledge in individuals with opioid use disorder: a pilot study. Drug Alcohol Depend 190:224–228
Khezri M, Farokhzadian J, Nematollahi M, Foroughameri G, Sharifi H (2019) HIV/AIDS prevention education: an effective tool for enhancing street children’s knowledge and attitude A randomized controlled trial. Child Youth Serv Rev 104:104351
Brooks R et al (2023) Improving HIV and HCV testing in substance use disorder programs (SUDs) that provide medications for opiate use disorder (MOUD): role of addressing barriers and implementing universal and site-specific approaches. Health Promot Pract 24:1018–1028
Mahmoudi TB, Khorsandi M, Shamsi M, Ranjbaran M (2020) Effect of education based on health belief model on preventive behaviors of hepatitis B disease in health volunteers. J Educ Community Health 7:169–175
Maqsood S, Iqbal S, Zakar R, Zakar MZ, Fischer F (2021) Determinants of overall knowledge and health behaviours in relation to hepatitis B and C among ever-married women in Pakistan: evidence based on Demographic and Health Survey 2017–18. BMC Public Health 21:2328
Mateu-Gelabert P et al (2018) Young drug users: a vulnerable population and an underutilized resource in HIV/HCV prevention. Curr HIV/AIDS Rep 15:324–335. https://doi.org/10.1007/s11904-018-0406-z
Nutbeam D, Muscat DM (2021) Health promotion glossary 2021. Health Promot Int 36:1578–1598
Aygun O, Cerim S (2021) The relationship between general health behaviors and general health literacy levels in the Turkish population. Health Promot Int 36:1275–1289
Degan TJ, Kelly PJ, Robinson LD, Deane FP (2019) Health literacy in substance use disorder treatment: a latent profile analysis. J Subst Abuse Treat 96:46–52
Champion KE et al (2019) Effectiveness of school-based eHealth interventions to prevent multiple lifestyle risk behaviours among adolescents: a systematic review and meta-analysis. The Lancet Digital Health 1:e206–e221. https://doi.org/10.1016/S2589-7500(19)30088-3
Acknowledgements
The author highly appreciates all participants for participating in the study and also the cooperation of Mr. Arash Mojodi Zamani in holding educational workshops.
Ethics code
IR.MUI.NUREMA.REC.1402.106.
Scientific code of the project proposal
1402123
Ethics approval in animal studies
Not applicable.
Funding
This study was financially supported by the Vice-Chancellor for Research Affairs of Isfahan University of Medical Sciences.
Author information
Authors and Affiliations
Contributions
ES, ZG, AK, and AM, contributed to the conceptualization, methodology, writing — original draft, visualization, supervision, and writing — reviewing and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Isfahan University of Medical Sciences, Isfahan, Iran. All the participants and their legal guardians were informed about the study objectives and signed written informed consents for taking part in the study. Moreover, the participants’ privacy and confidentiality were observed all through the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sharifi, E., Ghelbash, Z., Karami, A. et al. Effects of a comprehensive educational program on health behaviors and awareness of HIV, hepatitis B, and hepatitis C in men with substance use disorders. Middle East Curr Psychiatry 31, 43 (2024). https://doi.org/10.1186/s43045-024-00432-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-024-00432-7