
Abstract
Objectives
We aim to investigate the association between cognitive profiles of children and adolescents, classified using latent class analysis and emotional, behavioral and sociodemographic factors in a community-based sample of children and adolescents.
Methods
The sample consists of 161 participants recruited from a nationally representative household sample of 1517 children and adolescents who participated in a national mental health survey. Participants and their parents completed the following scales: Strengths and Difficulties Questionnaire, Mood and Feelings Questionnaire, and Screen for Child Anxiety Related Emotional Disorders. Participants were then administered a battery of cognitive tests from the Cambridge Automated Neuropsychological Assessment Battery as well as the Wechsler Nonverbal Scale of Ability.
Results
Latent class analysis showed a 2-class model that was stable and had good entropy (0.837). Class 1 included 58 participants (36.0%), and Class 2 included 103 participants (64.0%). Participants belonging to Class 1 performed better than those in Class 2 on all cognitive tasks. Chances for belonging to a specific Class varied based on different sociodemographic, behavioral and emotional factors: older participants with higher Intellectual Quotient, higher parental educational level, lower reported hyperactivity and better-reported mood were more likely to belong to Class 1.
Conclusion
Our results show a tight correlation between different emotional, behavioral and sociodemographic variables on one hand and cognitive functioning in children and adolescents on the other hand. This supports the continuous need for an integrative approach when building norms for cognitive tests that account at the least for all these variables.
Similar content being viewed by others


Background
Emotions and cognition have long been considered as 2 independent systems [37]. However, current research has shown that they influence one another, and even share underlying brain structures, such as the amygdala [50]. Brooks et al. [9] investigated the impact of depression on individuals’ attention, reaction times, and memory. Results showed that children and adolescents with depression performed worse than healthy participants on measures of verbal memory, visual memory, reaction time, and tasks of attention. A similar negative impact of depression on attention was also reported in adults by Sommerfeldt et al. [44] who showed that the presence of another disorder alongside depression exacerbates cognitive dysfunction. Furthermore, intellectual abilities were reported to be possibly influenced by emotions, with lower IQ scores being observed with severe symptoms of depression [6].
Recent studies investigated the ability of some cognitive measures to predict psychological distress later in life. For example, Kertz et al. [26] found that deficits in attention shifting during preschool years were linked to increased severity of anxiety three and half years later, and to increased depression severity five and a half years later,whereas deficits in inhibition were predictive of greater depression severity and increased anxiety several years later. Likewise, Gale et al. [19] showed that adolescents who had slow reaction times were at increased risk for depression and anxiety during adulthood. Finally, in a recent longitudinal study, Piek et al. [38] suggested that the development of motor skills during infancy and early childhood could predict anxiety and depressive symptoms at the ages 6 to 12 years.
Other studies have explored the clinical value of cognitive profiles in the course of psychiatric disorders. For example, our team has shown that deficits in executive functioning could be state markers rather than trait markers of depression [32], whereas sustained attention impairment seemed to be specific to patients with bipolar disorder [33]. F. Maalouf et al. [30] also showed that adolescents with depression who exhibited lower impulsivity and less difficulty in sustained attention showed greater improvement in symptoms after a six-week treatment with a selective serotonin reuptake inhibitor (SSRI).
In addition to this established correlation between emotions and cognition, one prominent contributor to cognitive development are sociodemographic factors. In fact, cognitive abilities are known to change with age mostly by improving over time, before they start to decline in late adulthood and old age. Sikora-Wachowicz et al. [42] examined age-related differences in short-term memory. Their results showed that humans become more prone to false memories as they age. Fandakova et al. [14] showed a similar effect of age on short term memory, with better results seen in young adults and teenagers compared to old adults and children. Amundsen et al. [3] also showed a significant age effect on visual-spatial working memory when comparing ninth graders’ performance on a “Visual Test for Learning” to that of younger children. On the other hand, Tao et al. [45] sought to study how attention, another cognitive process, develops among school-aged children. The study results showed that children aged between 9 and 12 years performed better on tasks measuring focused attention, alertness, attentional switching, supervisory attention, divided attention, sustained attention, and spatial attention compared to children aged between 7 and 8 years. These findings suggest that working memory and executive function improve with age in children.
Gender is another factor that was shown to possibly underly cognitive differences between individuals. For example, Rodríguez-Negro et al. [41] found gender differences in motor abilities of children between the ages of 6 and 8 years, with girls showing better balance skills and boys better motor precision and motor agility skills. On the other hand, Riley et al. [39] showed gender-related differences in sustained attention when comparing the performance of participants in countries where gender inequality pervades to that of others where no gender inequality was found. In a meta-analysis conducted by Voyer et al. [51] on gender differences in visual-spatial working memory in participants between the ages of 3 and 86, males were found to have better performance than females, but only in participants aged between 13 and 17 years.
Some of the previous results seemed to suggest that gender effect could be influenced by other moderating factors such as age. In fact, Kalyanshetti and Vastrad [25] examined the effect of both gender and age on tactile, auditory, and visual reaction times in children (between 8 and 12 years old) and adults (between 18 and 25 years old) of both genders. The results indicated that boys were significantly faster than girls,however, in adults, females and males did not differ on reaction times. Moreover, when comparing children and adults of both genders, adults (18 to 25 years old) exhibited faster reaction times than children of ages 8 to 12 years old. This study suggested that age could be a possible moderating factor between gender and reaction time. Likewise, Kokštejn et al. [27] examined the association among age, gender, and motor abilities in preschoolers between the ages of 3 and 6 years. Girls of ages 3 and 4 years old were found to have better fine motor and balance skills compared to boys of the same age,in contrast, six-year-old boys outperformed girls of the same age in catching and aiming. Moreover, when the authors controlled for age, they found a significant gender-related difference in motor abilities.
Cognitive abilities, such as motor abilities, working memory, and sustained attention, are also believed to be correlated with the socioeconomic status. For example, the development of motor abilities in school-aged children (6 to 10 years old) was found to increase as the socioeconomic status (SES) of the children’s families increased [15]. Aiman et al. [2] found that children who came from a low SES had lower fine motor performance compared to those who came from higher SES. Furthermore, Ferreira et al. [15] showed that better home environment quality was related to better development of motor abilities in children. However, they found that age moderated the relationship between SES, home environment, and motor abilities,younger children seemed to be impacted by SES more than older children. Similarly, Da Rosa Piccolo et al. [12] showed that children with higher SES had better performance on working memory and executive function tasks, but SES had a stronger influence on the performance of children who were younger than nine years old. Last, Lawson et al. [28] investigated the association between SES and executive functions across childhood, adolescence, and young adulthood. They found that participants of lower SES performed worse than those of higher SES. SES has also been shown to influence the neural systems of selective attention [52]. In conclusion, available evidence suggests that higher SES positively impacts the development of motor abilities, memory, and attention.
In summary, studies seem to support a significant correlation between cognitive performance and emotional disorders such as anxiety and depression in children and adolescents. However, none of these studies has explored the correlation between cognitive performance and reported symptoms of anxiety and depression in a non-clinical community-based population while controlling for the effects of different sociodemographic factors on cognition, such as age, gender, IQ, and parental SES.
This is the first study to examine the existing cognitive profiles in a community-based sample of children and adolescents, and to investigate the emotional symptoms as well as behavioral and sociodemographic factors associated with those cognitive profiles.
Methods
Sampling and recruitment
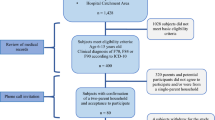
This study is part of a larger research project that was conducted by our team. A nationally representative household sample of 1517 children and adolescents living in Lebanon completed this study between February 2018 and November 2018 following recruitment using probability sampling as part of the Psychopathology in Children and Adolescents Study (PALS) [31] or the detailed methodology including sampling techniques). After completing the main study protocol, participants aged between 5 and 17 years 11 months were given the option to partake in the present study. A total of 161 agreed to participate and sat for the testing around within 1–3 months following the original interview. As presented in Table 1, compared to those who refused, participants were more likely to come from families of lower income (p = 0.02). With respect to father’s education, participants’ fathers were more likely to have elementary education or less, while non participants’ father were more likely to have high school education or less, but both groups were similar with respect to university education (Table 1). On the other hand, there was no difference between participants and non-participants with respect to age, sex, maternal education, paternal employment, maternal employment, or history of any chronic illness (Table 1). The two groups also differed on depression scores but there were no differences between the two groups on the other measures of emotional and behavioral symptoms.
The study was conducted in accordance with Helsinki Declaration. It was approved by the local Internal Review Board. Written informed consent was obtained from parents of children and child assent were obtained. Computerized cognitive tasks that take about 40–50 min to complete [40] as well as a short standardized assessment of intellectual abilities were administered.
Instruments and measures
General information sheet
A general information sheet was first completed by a parent/legal guardian who provided information on basic demographics including family structure, family income and parental level of education.
Emotions and behavior screening
The Strengths and Difficulties Questionnaire (SDQ)- parent and child version
The SDQ is a self-report that was used to screen for emotional, conduct, and hyperactivity difficulties in children aged 5 to 7 years and for conduct and hyperactivity symptoms in participants aged 8 to 17 years [20]. We used an Arabic version of the SDQ that was previously validated [53].
The Mood and Feelings Questionnaire MFQ
The MFQ is a 33 item self-report measure of depressive symptoms among children/adolescents aged 8 to 18 [11]. The previously validated Arabic version along with previously established cutoff scores in parents and children were used [46].
Screen for Child Anxiety Related Emotional Disorders (SCARED)
The SCARED screens for anxiety disorders in children and adolescents [7]. SCARED was completed by children and adolescents aged 8 to 17 and one parent/guardian and previously established local cut-off scores were used [24].
Cognitive tasks
A battery of CANTAB tasks was then administered by a trained clinical psychologist. The tests were done on an IPAD where software recorded the performance of each participant and data was later extracted and linked to the participants. Participants also underwent the Weschler Non-Verbal Abilities Assessment (WNV) test. The CANTAB battery of tests was done in 40–50 min whereas the WNV test took an additional 20 min.
The Motor Screening test (MOT)
MOT was administered at the beginning of the battery as an introduction to the touch screen for the participant. It screens for visual, movement, and comprehension difficulties. Participants are instructed to touch a cross that appears in different locations on the screen. Mean latency in milliseconds of correct responses (MOTML) is the main outcome measure.
Rapid Visual Processing Task (RVP)
RVP assesses sustained attention. Single digits in random order on the screen. Participants are instructed to respond to three sequences of three digits “2–4-6”, “3–5-7”, and “4–6-8”. RVP A and RVP Probability of Hit (RVPPH) were our main outcome variables as they measured how good the subject was at detecting target sequences. A higher score reflected a better performance.
Delayed Matching to Sample (DMS)
DMS assesses short-term memory by presenting participants with a complex pattern on a computer screen (the sample) followed by four patterns only one of which is identical to the first pattern. In some trials, the sample and choice items are presented consecutively, while in others there is a 0, 4, or 12-s delay between the sample and the choice items. Participants are instructed to touch the pattern on the screen that matches the sample. Our main outcome measure was the percentage of correct answers for all delays.
Stop Signal Task (SST)
The SST serves as an indicator of one's ability to inhibit responses. In this task, a white ring appears on a black screen, followed by a visual arrow (pointing left or right) after a 500 ms delay. Participants are instructed to touch the right-hand press pad for right-pointing arrows and the left-hand press pad for left-pointing arrows. However, they are required to withhold their response if a beep (auditory signal) is heard. The primary outcome variable, SSTSSRT (Stop Signal Reaction Time), quantifies the estimated time at which an individual can successfully inhibit responses 50% of the time.
Reaction Time (RTI)
Reaction Time was employed to evaluate both motor and mental response speeds, encompassing movement time, reaction time, response accuracy, and impulsivity. In the task, participants are required to choose and maintain a button press at the screen's bottom. Circles, one in the simple mode and five in the five-choice mode, are presented above. In each instance, a yellow dot emerges in one of the circles, prompting the participant to swiftly release the bottom button and select the circle containing the dot. The primary outcome measures include the median duration for a subject to release the response button and the median time taken for a subject to release the response button and choose the target stimulus.
Paired Associates Learning (PAL)
Paired Associates Learning assesses visual memory and the ability to acquire new information. In this task, boxes are presented on the screen and are randomly "opened." Within one or more of these boxes, a pattern is revealed. Subsequently, the patterns are individually displayed in the center of the screen, and the participant is tasked with identifying the box where the pattern was originally located. In the event of an error, the boxes are opened sequentially as a reminder of the pattern locations. The primary outcome is the number of times a subject correctly identifies the box on their initial attempt while recalling the pattern locations.
Spatial Working Memory (SWM)
The Spatial Working Memory task assesses the retention and manipulation of visuospatial information, serving as a metric for strategy and working memory errors. The test initiates with the display of colored squares on the screen. Participants, through a process of elimination, are required to identify one yellow 'token' in each set of boxes and utilize them to fill an empty column on the right side of the screen. The number of boxes can progressively increase, up to a maximum of 12, for participants to search. Primary outcome measures include the number of instances subjects incorrectly revisit a box where a token was previously found and the number of instances subjects initiate a new search pattern from the same starting box as before. Consistently starting from the same point suggests the use of a planned strategy in locating the tokens.
Wechsler Nonverbal Scale of Ability (WNV)
The WNV is an assessment tool designed to measure intellectual abilities in culturally and linguistically diverse groups, employing nonverbal content. The battery comprises two forms, each featuring four subtests. The first form, applicable to participants aged 4 to 7 years, includes matrices, coding, object assembly, and recognition. The second form, suitable for examinees aged 8 to 17 years, consists of matrices, coding, spatial span, and picture arrangement.
A condensed version allows the use of matrices and recognition subtests to calculate the Full-Scale Score for the younger group, and matrices and picture arrangement subtests for the older group. Raw scores obtained in each subtest are then converted into scale scores using norms specific to each age group.
Data analysis
In order to classify participants based on their performance on cognitive tests, latent class analysis (LCA) was performed using the scores of the tasks’ outcome measures. The analysis was initially performed using 1-class model (BIC = 4446.86), then the number of classes was increased to find the model with the best fit to the data, as determined by the Bayesian information criteria (BIC = 4446.86 for 1-class model, 4295.84 for 2-class model, and 4187.29 for 3-class model), and Lo-Mendell-Rubin (LMR) adjusted likelihood ratio tests (p 0.01 for 2-class model, and 0.13 for 3-class model. To be able to describe the cognitive profiles of those classes, they were compared with respect to the 12 cognitive measures using an independent sample t-test.
Classes were also compared with respect to demographics and parental education and employment using Pearson Chi-square or Fischer exact test and with respect to SDQ, SCARED, and MFQ scores using independent sample t-tests. Finally, variables significantly associated with “cognitive class” were entered into a multivariate binary logistic regression with the cognitive class being the outcome. This analysis was performed for all age groups using SDQ scores, and for patients above age 8 using MFQ and SCARED scores.
The latent class analysis was performed using Mplus, while the rest of the statistical analysis was performed using SPSS. P-values less than 0.05 were considered to be statistically significant.
Results
The sample consisted of 161 participants with 52.8% (N = 85) being males. Age was between 5 years and 7-years-11months for 7 participants (4.3%), between 8 years and 11-years-11-months for 86 participants (53.4%), and between 12 years and 17-years-11-months for 68 participants (42.2%). Baseline data are presented in Table 1.
Latent class analysis
Latent class analysis showed that the model that best fits the data was the 2-class model was stable and had good entropy (0.837). In addition, compared to the 1-class solution, the 2-class model had lower BIC (4295.84 vs. 4446.86) and significant Vuong-Lo-Mendell-Rubin and Lo-Mendell-Rubin Adjusted Likelihood Ratio Tests (p’s = 0.01).
The first class (Class 1) included 58 participants (36.0%), and the second class (Class 2) included 103 participants (64.0%). Class 1 had significantly higher raw scores on tasks measuring correct responses (i.e. DMS Percent Correct (All Delays), RVP A, RVP Probability of Hit, and PAL First Attempt Memory Score compared to the second class), and lower raw scores on tasks measuring speed (i.e. SST Stop Signal Reaction Time, MOT Mean Latency, RTI Median Five Choice Movement Time, RTI Median Five Choice Reaction Time, RTI Simple Median Movement Time, RTI Simple Median Reaction Time, SWM Between Errors, and SWM Strategy (6–8 Boxes)) (Table 2). In summary, these results suggest better performance of participants belonging to Class 1 on all tasks.
Factors associated with classes
As reflected in Table 2, there was no significant difference between the two classes with respect to sex (p = 0.59). On the other hand, there was a significant association with age, with Class 1 being significantly older (12.5 ± 2.87 years) than Class 2 (10.31 ± 2.88 years; p = 0.001). In addition, Class 1 was associated with higher parental education (p = 0.05) and parental income (p = 0.01) as compared to Class 2. Finally, participants in Class 1 were found to have a higher mean IQ score compared to class two (P < 0.001).
MFQ and SCARED reports were available for participants who were at least 8 years old. There was no significant difference between the two groups with respect to child report on MFQ and SCARED. On the other hand, Class 1 was significantly associated with lower parental report on the MFQ (p = 0.00) and SCARED as compared to Class 2 (p = 0.029) (Table 3).
Multivariate logistic regression
In the multivariate logistic regression (Table 4), odds of belonging to Class 2 compared to Class 1 were lower with increased age (OR = 0.74, 95% CI = 0.63–0.86), and in children of parents with high school educational level compared to those of parents with elementary educational level (OR = 0.09, 95% CI = 0.01–0.51). In addition, there was a borderline significant association with SDQ hyperactivity with odds of belonging to Class 2 being 1.2 times higher for higher “SDQ hyperactivity score as per parent report”.
As MFQ and SCARED instruments were administered to children above age 8, the above analysis was repeated among this age group only (Table 5). There were no changes in the results presented in Tables 2 and 3. With respect to the multivariate logistic regression (Table 5), age group, highest parental education level, and MFQ score as per parent report were independently associated with the cognitive class. The odds of being in class 2 compared to Class 1 decreased with each one-year increase in age (OR = 0.72, 95% CI = 0.61–0.85). In addition, participants with parents with at least high-school education were 0.1 times as likely to belong to Class 2 as compared to participants whose parents had elementary education. Finally, the odds of belonging to Classe 2 were 1.1 times higher for higher MFQ-parents scores.
Discussion
This is the first study to investigate the cognitive profiles of a community-based sample of children and adolescents through latent class analysis and examine their association with emotional symptoms and sociodemographic factors.
Results showed that there are 2 different “cognitive classes” within a community sample where participants belonging to Class 1 showed significantly better performance on all tests. Specifically, their raw scores were higher on tasks measuring precision and correct answers and were lower on tasks based on a speed component. Since all of the tasks rely mainly on executive abilities, it could be argued that participants who belong to Class 1 have better prefrontal cortex functioning, or possibly a higher maturity of this brain area. Both the ventromedial prefrontal cortex (vmPFC) and the dorsolateral prefrontal cortex (dlPFC) are believed to allow better executive functions such as planning and abstract reasoning, as well as inhibition and self-control [22, 35]. This neurofunctional hypothesis seems to be supported by this study’s outcome.
Our results showed that the odds of belonging to Class 1 were higher for older participants while controlling for all other variables. This significant age effect falls in line with previous studies that showed a better cognitive performance in older children, especially on executive tasks such as working memory or different attention tasks [3, 14, 42, 45]. Such abilities are known to develop with age, which explains why older children are expected to outperform younger ones. Another expected result that supports executive functioning differences between groups was the predictive value of IQ in determining group distribution: children with higher IQ scores had more chances to belong to Class 1 even after controlling for age. In fact, higher IQ is believed to reflect higher overall cognitive functioning and more specifically better executive functioning. For example, Arffa [4] showed that gifted children outperformed other children on executive tests. Also, Der and Deary [13] examined the association between intelligence and reaction time. Their results indicated a significant positive correlation that seemed to increase with age. Finally, Smits-Engelsman and Hill [43] showed that poor motor abilities in children were associated with a lower IQ.
Our results also showed that children with low hyperactivity scores on the SDQ had higher chances of belonging to Class 1, when controlling for their age, IQ, or SES aspects. This result comes as no surprise, since hyperactivity, which is usually controlled by the frontal lobes, has been reported to affect several cognitive abilities, including executive ones. For example, Bolfer et al. [8] looked at reaction time in children with attention deficit/hyperactivity disorder (ADHD). Results showed that male participants between the ages of 9 and 12 with ADHD had slower reaction times compared to the control group. Norvilitis [36] explored executive functioning in ADHD and showed that children with ADHD-Combined exhibit impairments in cognitive functions such as in planning, sustained attention, and spatial working memory. Also, Mokobane et al. [34] reported that school-aged children with ADHD had poor fine motor abilities.
Higher family income and educational status are known to be predictors of better cognitive abilities [12, 15].They are also usually expected to vary in the same direction, with higher family income typically found in communities with higher educational levels [10]. As expected, our results showed a significant effect for parental education in predicting cognitive abilities in our sample, and the odd of belonging to Class 2 was lower for children whose parents have a high school educational level. However, our results did not show that family income predicted cognitive profiles. This result is not compatible with previously published studies [12, 28] that showed a positive correlation between high SES and cognitive performance. Nevertheless, this discrepancy between our results and the literature could stem from two aspects: In previous studies, educational level and family income are referred to as SES, which makes it harder to determine the exact contribution of parental education and/or income in that concept. Moreover, and despite analyzing the effect of age in some studies, none of the previous studies controlled for additional variables, such as IQ, that can be affected by low SES [16, 49] and explain the variability of the cognitive outcome. The same argument could be made to explain the absence of a significant predictive value for gender in our study. In previous studies, cognitive differences were reported between males and females [51], and this effect seemed to be moderated by age. However, none of the previous studies pertaining to this aspect controlled for sociodemographic factors or IQ.
When controlling for all factors in the general sample, we found no significant effect for SDQ emotional symptoms in predicting participants’ belonging to the different “cognitive classes”. However, in the logistic regression model in which we only included participants who were at least 8 years old, higher parental reports of depressive symptoms as measured by the MFQ were significantly associated with belonging to Class 2 and hence, with having poorer performance on executive function tasks. This is in line with findings showing that depressive symptoms in community samples are associated with impaired performance on executive function tasks [1], a finding that seems to be age-specific since depressive symptoms have been shown to have a larger effect on neuropsychological functioning in early adolescence relative to later adolescence [1].
In clinical samples, depressive symptom severity and earlier age of onset of depressive disorders have also been associated with worse executive functions in youth [32]. In addition, executive functioning has been shown to predict prognosis in this population. Specifically, worse executive function predicted a lack of improvement in youth treated for depression [30] and later worse socio-occupational outcome among outpatient youth with depression in a cohort study [29].
Neural circuits that subserve executive functioning have emerged as important biological markers in depression in youth. Indeed, adolescents with depression showed reduced activation in the right dorsolateral and anterior cingulate gyrus when performing relevant tasks compared to healthy controls [21] and reduced connectivity between the prefrontal cortex and neural circuits that respond to positive and negative emotional information [18, 48].
The association between mood symptoms and executive functioning is complex and bi-directional. While we were able to show a correlation in our present cross-sectional study, we cannot confirm whether poor executive functions are a predictor or a consequence of long-lasting depressive symptoms on a vulnerable developing brain. Future studies should consider examining the association of neurocognitive deficits and mood symptoms in a developmental context and a longitudinal fashion [17].
Our findings should be considered in light of the following limitations: Our sample may not be representative of the population and our results may not be generalizable to other contexts knowing that not all participants who were recruited for the national survey opted to participate in the present study. This may have led to a self-selection bias. In addition, our data examined the presence of emotional and behavioral symptoms based on reports from participants and their parents and we did not examine clinical diagnoses per se. Hence, the association with the cognitive classes needs to be understood in that context although subclinical symptoms predict the presence of disorders [5]. Lastly, an important limitation is the fact that self-reports were not completed on the day of testing which wasn’t possible for logistics reasons. This time lag would not affect sociodemographic factors which typically do not change over a short period of time but may have impacted emotional symptoms which could have worsened or improved by the time of testing.
Conclusion
In conclusion, this study is the first to examine sociodemographic factors and emotional symptoms at play in neurocognitive performance in a community-based sample. Our results suggest that different factors correlate with cognitive abilities and most of which are rarely considered in clinical settings. In fact, while most of the cognitive assessment tools typically control for age and/or sex, they rarely do so for other pertinent factors such as SES. This study also sheds the light on an existing gap in several clinical tools, and strongly advocates for an integrative approach when building norms for cognitive tests.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Afzali MH, O’Leary-Barrett M, Séguin JR, Conrod PJ (2018) Effect of depressive symptoms on the evolution of neuropsychological functions over the course of adolescence. J Affect Disord 229:328–333. https://doi.org/10.1016/j.jad.2017.11.060
Aiman, S., Yusof, S. M., Kadir, Z. A., & Sabturani, N. (2015). The Relationship Between Socioeconomic Status and Fine Motor Skills Among Six-Year-Old Preschool Children. Proceedings of the 2nd International Colloquium on Sports Science, Exercise, Engineering and Technology 2015 (ICoSSEET 2015), 141–148. https://doi.org/10.1007/978-981-287-691-1_15
Amundsen ML, Garmannslund PE, Stokke H (2014) Visual working memory- gender and age differences. European J Educ Sci 01(03):1–7. https://doi.org/10.19044/ejes.v1no3a1
Arffa S (2007) The relationship of intelligence to executive function and non-executive function measures in a sample of average, above average, and gifted youth. Arch Clin Neuropsychol 22(8):969–978. https://doi.org/10.1016/j.acn.2007.08.001
Aronen ET, Soininen M (2000) Childhood depressive symptoms predict psychiatric problems in young adults. Canadian J Psychiatr 45(5):465–470. https://doi.org/10.1177/070674370004500507
Barrera-Valencia M, Calderón-Delgado L, Trejos-Castillo E, O’Boyle M (2017) Cognitive profiles of post-traumatic stress disorder and depression in children and adolescents. Int J Clin Health Psychol 17(3):242–250. https://doi.org/10.1016/j.ijchp.2017.05.001
Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, Neer SM (1997) The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J American Acad Child Adolescent Psychiatry 36(4):545–553. https://doi.org/10.1097/00004583-199704000-00018
Bolfer C, Casella EB, Baldo MVC, Mota AM, Tsunemi MH, Pacheco SP, Reed UC (2010) Reaction time assessment in children with ADHD. Arq Neuropsiquiatr 68(2):282–286. https://doi.org/10.1590/s0004-282x2010000200025
Brooks BL, Iverson GL, Sherman EMS, Roberge M (2010) Identifying cognitive problems in children and adolescents with depression using computerized neuropsychological testing. Appl Neuropsychol 17(1):37–43. https://doi.org/10.1080/09084280903526083
Chevalier A, Lanot G (2002) The relative effect of family characteristics and financial situation on educational achievement. Educ Econ 10(2):165–181. https://doi.org/10.1080/09645290210126904
Costello EJ, Angold A (1988) Scales to assess child and adolescent depression: checklists, screens, and nets. J American Acad Child Adole Psychiatry 27(6):726–737. https://doi.org/10.1097/00004583-198811000-00011
Da Rosa Piccolo L, Arteche AX, Fonseca RP, Grassi-Oliveira R, De Salles JF. (2016). Influence of family socioeconomic status on IQ, language, memory and executive functions of Brazilian children. Psicologia-Reflexao E Critica, 29(1). https://doi.org/10.1186/s41155-016-0016-x
Der G, Deary IJ (2017) The relationship between intelligence and reaction time varies with age: results from three representative narrow-age age cohorts at 30, 50 and 69 years. Intelligence 64:89–97. https://doi.org/10.1016/j.intell.2017.08.001
Fandakova Y, Sander MC, Werkle-Bergner M, Shing YL (2014) Age differences in short-term memory binding are related to working memory performance across the lifespan. Psychol Aging 29(1):140–149. https://doi.org/10.1037/a0035347
Ferreira L, Godinez I, Gabbard C, Vieira JLL, Caçola P (2018) Motor development in school-age children is associated with the home environment including socioeconomic status. Child Care Health Dev 44(6):801–806. https://doi.org/10.1111/cch.12606
Fischbein S (1980) IQ and social class. Intelligence 4(1):51–63. https://doi.org/10.1016/0160-2896(80)90006-9
Forbes EE (2020) Chasing the holy grail: developmentally informed research on frontostriatal reward circuitry in depression. Am J Psychiatry 177(8):660–662. https://doi.org/10.1176/appi.ajp.2020.20060848
Furman DJ, Hamilton JH, Gotlib IH (2011) Frontostriatal functional connectivity in major depressive disorder. Biol Mood Anxiety Disord 1(1):1–1. https://doi.org/10.1186/2045-5380-1-11
Gale CR, Batty GD, Cooper SA, Deary IJ, Der G, McEwen BS, Cavanagh J (2015) Reaction Time in adolescence, cumulative allostatic load, and symptoms of anxiety and depression in adulthood. Psychosom Med 77(5):493–505. https://doi.org/10.1097/psy.0000000000000189
Goodman R (1997) The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry 38(5):581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
Halari R, Simic M, Pariante CM, Papadopoulos A, Cleare AJ, Brammer M, Rubia K (2009) Reduced activation in lateral prefrontal cortex and anterior cingulate during attention and cognitive control functions in medication-naïve adolescents with depression compared to controls. J Child Psychol Psychiatry 50(3):307–316. https://doi.org/10.1111/j.1469-7610.2008.01972.x
Hale JB, Fiorello CA. (2004). School Neuropsychology: A Practitioner’s Handbook (1st ed.). The Guilford Press.
Hampton Wray A, Stevens C, Pakulak E, Isbell E, Bell T, Neville H (2017) Development of selective attention in preschool-age children from lower socioeconomic status backgrounds. Dev Cogn Neurosci 26:101–111. https://doi.org/10.1016/j.dcn.2017.06.006
Hariz N, Bawab S, Atwi M, Tavitian L, Zeinoun P, Khani M, Maalouf FT (2013) Reliability and validity of the Arabic Screen for Child Anxiety Related Emotional Disorders (SCARED) in a clinical sample. Psychiatry Res 209(2):222–228. https://doi.org/10.1016/j.psychres.2012.12.00
Kalyanshetti SB, Vastrad BC (2012) Effect of age and gender on visual, auditory and tactile reaction time in normal subjects. Biomediicine (India) 32:217–221
Kertz SJ, Belden AC, Tillman R, Luby J (2015) Cognitive control deficits in shifting and inhibition in preschool age children are associated with increased depression and anxiety over 7.5 years of development. J Abnormal Child Psychol 44(6):1185–1196. https://doi.org/10.1007/s10802-015-0101-0
Kokštejn J, Musálek M, Tufano JJ (2017) Are sex differences in fundamental motor skills uniform throughout the entire preschool period? PLoS ONE 12(4):e0176556. https://doi.org/10.1371/journal.pone.0176556
Last BS, Lawson GM, Breiner K, Steinberg L, Farah MJ (2018) Childhood socioeconomic status and executive function in childhood and beyond. PLoS ONE 13(8):e0202964. https://doi.org/10.1371/journal.pone.0202964
Lee RS, Hermens DF, Redoblado-Hodge MA, Naismith SL, Porter MA, Kaur M, Hickie IB (2013) neuropsychological and socio-occupational functioning in young psychiatric outpatients: a longitudinal investigation. PLOS ONE 8(3):e58176. https://doi.org/10.1371/journal.pone.0058176
Maalouf F, Bakhti R, Tamim H, Shehab S, Brent D (2018) Neurocognitive predictors of clinical improvement in selective serotonin reuptake inhibitor-treated adolescents with major depressive disorder. J Child Adolesc Psychopharmacol 28(6):387–394. https://doi.org/10.1089/cap.2017.0105
Maalouf FT, Alrojolah L, Akoury-Dirani L, Barakat M, Brent DA, Elbejjani M, Ghandour LA (2022) Psychopathology in Children and Adolescents in Lebanon Study (PALS): a national household survey. Soc Psychiatry Psychiatric Epidemiol 57(4):761–774. https://doi.org/10.1007/s00127-021-02208-4
Maalouf FT, Brent D, Clark L, Tavitian L, McHugh RM, Sahakian BJ, Phillips ML (2011) Neurocognitive impairment in adolescent major depressive disorder: State vs. trait illness markers. J Affect Dis 133(3):625–632. https://doi.org/10.1016/j.jad.2011.04.041
Maalouf FT, Klein C, Clark L, Sahakian BJ, LaBarbara EJ, Versace A, Phillips ML (2010) Impaired sustained attention and executive dysfunction: BIPOLAR disorder versus depression-specific markers of affective disorders. Neuropsychologia 48(6):1862–1868. https://doi.org/10.1016/j.neuropsychologia.2010.02.015
Mokobane M, Pillay BJ, Meyer AM. (2019). Fine motor deficits and attention deficit hyperactivity disorder in primary school children. South African Journal of Psychiatry, 25. https://doi.org/10.4102/sajpsychiatry.v25i0.1232
Motzkin JC, Philippi CL, Wolf RC, Baskaya MK, Koenigs M (2015) Ventromedial prefrontal cortex is critical for the regulation of amygdala activity in humans. Biol Psychiat 77(3):276–284. https://doi.org/10.1016/j.biopsych.2014.02.014
Norvilitis, J. M. (2015). ADHD - New Directions in Diagnosis and Treatment.
Pessoa L (2009) How do emotion and motivation direct executive control? Trends Cogn Sci 13(4):160–166. https://doi.org/10.1016/j.tics.2009.01.006
Piek JP, Barrett NC, Smith LM, Rigoli D, Gasson N (2010) Do motor skills in infancy and early childhood predict anxious and depressive symptomatology at school age? Hum Mov Sci 29(5):777–786. https://doi.org/10.1016/j.humov.2010.03.006
Riley E, Okabe H, Germine L, Wilmer J, Esterman M, DeGutis J (2016) Gender differences in sustained attentional control relate to gender inequality across countries. PLoS ONE 11(11):e0165100. https://doi.org/10.1371/journal.pone.0165100
Robbins TW, James M, Owen A, Sahakian BJ, McInnes L, Rabbitt P (1994) Cambridge Neuropsychological Test Automated Battery (CANTAB): a factor analytic study of a large sample of normal elderly volunteers. Dement Geriatr Cogn Disord 5(5):266–281. https://doi.org/10.1159/000106735
Rodríguez-Negro J, Huertas-Delgado FJ, Yanci J (2019) Motor skills differences by gender in early elementary education students. Early Child Dev Care 191(2):281–291. https://doi.org/10.1080/03004430.2019.1617284
Sikora-Wachowicz B, Lewandowska K, Keresztes A, Werkle-Bergner M, Marek T, Fafrowicz M (2019) False recognition in short-term memory – age-differences in confidence. Front Psychol 10(10):2785. https://doi.org/10.3389/fpsyg.2019.02785
Smits-Engelsman BCM, Hill EL (2012) The relationship between motor coordination and intelligence across the IQ range. Pediatrics 130(4):e950–e956. https://doi.org/10.1542/peds.2011-3712
Sommerfeldt SL, Cullen KR, Han G, Fryza BJ, Houri AK, Klimes-Dougan B (2015) Executive attention impairment in adolescents with major depressive disorder. J Clin Child Adolesc Psychol 45(1):69–83. https://doi.org/10.1080/15374416.2015.1072823
Tao T, Wang L, Fan C, Gao W, Shi J. (2017). Latent Factors in Attention Emerge from 9 Years of Age among Elementary School Children. Front Psychol, 8. https://doi.org/10.3389/fpsyg.2017.01725
Tavitian L, Atwi M, Bawab S, Hariz N, Zeinoun P, Khani M, Maalouf FT (2013) The arabic mood and feelings questionnaire: psychometrics and validity in a clinical sample. Child Psychiatr Human Devel 45(3):361–368. https://doi.org/10.1007/s10578-013-0406-6
The Relationship Between Motor Coordination and Intelligence Across the IQ Range. (2012). Pediatrics, 130(4), e950–e956. https://doi.org/10.1542/peds.2011-3712d
Treadway MT, Pizzagalli DA (2014) Imaging the pathophysiology of major depressive disorder - from localist models to circuit-based analysis. Biol Mood Anxiety Dis 4(1):5. https://doi.org/10.1186/2045-5380-4-5
Turkheimer E, Haley AP, Waldron M, D’Onofrio BM, Gottesman II (2003) Socioeconomic status modifies heritability of IQ in young children. Psychol Sci 14(6):623–628. https://doi.org/10.1046/j.0956-7976.2003.psci_1475.x
Tyng CM, Amin HU, Saad MNM, Malik AS. (2017). The Influences of Emotion on Learning and Memory. Front Psychol, 8. https://doi.org/10.3389/fpsyg.2017.01454
Voyer D, Voyer SD, Saint-Aubin J (2016) Sex differences in visual-spatial working memory: a meta-analysis. Psychonomic Bull Rev 24(2):307–334. https://doi.org/10.3758/s13423-016-1085-7
Wray AH, Stevens C, Pakulak E, Isbell E, Bell TS, Neville HJ (2017) Development of selective attention in preschool-age children from lower socioeconomic status backgrounds. Dev Cogn Neurosci 26:101–111. https://doi.org/10.1016/j.dcn.2017.06.006
Zeinoun P, Bawab S, Atwi M, Hariz N, Tavitian L, Khani M, Maalouf FT (2013) Validation of an Arabic multi-informant psychiatric diagnostic interview for children and adolescents: development and Well Being Assessment-Arabic (DAWBA-Arabic). Comprehensive Psychiatry 54(7):1034–1041. https://doi.org/10.1016/j.comppsych.2013.04.012
Acknowledgements
Not applicable.
Funding
This study was funded by the American University of Beirut Faculty of Medicine – Medical Practice Plan.
Author information
Authors and Affiliations
Contributions
MB, WS and GP analyzed the data, MB, WS and FM interpreted the data and drafted the manuscript, all authors reviewed and revised the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the American University of Beirut-Institutional Review Board
Consent for publication
Not applicable.
Competing interests
Dr. Brent reports the following: Royalties from Guilford Press, UpToDate, and eRT; consultant, Healthwise, on Scientifics Board of Klingenstein Third Generation Foundation and the American Foundation for Suicide Prevention, Funding from NIMH, AFSP, and the Once Upon A Time Foundation.
Dr. Maalouf reports consultancy work with UNICEF.
All other authors disclose no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Barakat, M., Shamseddeen, W., Hanna, E. et al. Neurocognitive profiles in a community sample of children & adolescents: sociodemographic, behavioral and emotional correlates. Middle East Curr Psychiatry 31, 22 (2024). https://doi.org/10.1186/s43045-024-00413-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-024-00413-w