
Abstract
Background
The autism spectrum disorder (ASD) has no identified biomarker for early detection or for its severity. As for the brain-derived neurotrophic factor (BDNF), it is a crucial neurotropic factor that regulates the plasticity and maturing of neuronal synapses. Accordingly, it might influence how children with autism develop.
Method
To evaluate the BDNF serum levels in autistic children and their relationship with the illness severity as well as with the common drugs received by autistic patients, 60 patients with autism along with another 60 normally developing children were involved in the study. Using the Childhood Autism Rating Scale (CARS), the severity of autism was then evaluated. The ELISA method was used to measure the BDNF level.
Results
It was seen that the BDNF concentrations were higher in autism patients (P < 0.001). There was also a highly strong positive association between the CARS score and the BDNF (P < 0.001). Using the cut-off value of > 2.8 of BDNF helped to distinguish between well-developing and autistic children, with the aspects of “sensitivity” and “specificity” being 88.3% and 80%, respectively. Moreover, children with autism who received omega-3 had statistically lower levels of BDNF than those who did not take any (P = 0.040).
Conclusion
The serum BDNF concentration is higher in autism; this proposes that the BDNF may contribute to the onset or progress of autism. Therefore, it may be used as a noninvasive biomarker for the illness severity because of its greater occurrence in autistic children who have severe social impairment.
Similar content being viewed by others


Introduction
Autism spectrum disorder (ASD) is a series of complicated neurodevelopmental diseases that lead to difficulties in communication, language, and stereotyped behaviours [1]. In the last decades, there has been a substantial rise in ASD that cannot be solely attributed to improved diagnosis and more awareness of new cases [2]. As a result, it is crucial to continue searching the etiological reasons that could explain this increase [3].
There are numerous causes that may lead to the development of the autism phenotype, but the exact cause of autism is still yet unknown [4]. In other words, the causes of the clinical signs of ASD may be genetic, environmental, or a combination of both [5].
Synaptic disruption has been hypothesized as a potential mechanism for the development of neurodevelopmental diseases [6]. The likelihood that the autistic disorder behaviour traits result from synaptic dysfunction is supported by the observation that ASD traits are frequently observed in children with genetic disorders (like fragile X syndrome) which have been shown to disrupt the synaptic function [7].
A crucial neurotrophin for controlling synaptic plasticity, lifespan, and neuronal differentiation is the BDNF. Since the BDNF protein was purified, clear proof of its crucial function in the physiology, pathophysiology, and development of mammalian brains has been revealed [8].
BDNF expression levels have a significant impact on neutron activity, which is closely related to learning and memory. The BDNF also affects an individual’s physical growth and development [9, 10].
As for the BDNF depletion, it has been linked to the severity of neurological dysfunction and has been found in both neurodegenerative and mental illnesses. The significance of the BDNF’s role as a biomarker for ASD is becoming more noticed these days. However, inconsistent data from preclinical studies have related BDNF reduction to autism and intellectual disability.
A mean of 39.1% of people with autism, with or without epilepsy, and 8–80% of children with ASD who are not epileptics had abnormal EEGs [11]. Numerous investigations raised issues about EEG changes and their possible relations to BDNF [12, 13].
Although numerous studies in rats have shown a strong relationship between BDNF concentrations in serum and in the nervous system [14], proof of this correlation in humans is still missing. However, it is believed that peripheral BDNF concentrations inadvertently mirror brain BDNF concentrations [15].
Accordingly, the current research has sought to evaluate the serum level of BDNF and its correlation to the severity of social affection in autistic children, electrophysiological activity, and the relationship between the synaptic disruption assessed by the BDNF and the oral omega-3 supplementation.
Subjects and methods
Participants
The current controlled cross-sectional study comprised 120 children. Sixty of them had the ASD, aka the case group, and were treated at the Child Psychiatry Clinic, at Ain Shams University, while the other 60 were healthy children who were sex and age matched, aka the control group. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) was used to confirm the diagnosis of ASD [16]. Children with neurodevelopmental disorders as Down syndrome or Rett syndrome were excluded from this research. Moreover, age, gender, BMI, and dietary habits were taken into consideration when pairing the two groups. In order to facilitate further comparison and analysis, patients with autism who received an omega-3 supplement for 3 months (0.700 g daily syrup dose) as well as patients who received antipsychotics (risperidone 0.5–1 mg/day or aripiprazole 5 mg/day) at the last 3 months were further subcategorized.
After comparing the level of BDNF between the control and ASD cases, Barbosa et al. (2020) reported a large effect size. Generally, a sample size of 40 control and 40 cases would achieve a power of 80 to detect a medium-to-large effect size (0.65), using t-test, with the significance level being 0.05.
Regardless of the age of the child, all parents and guardians agreed and approved the consent. The study complied with the Declaration of Helsinki’s guidelines and was granted approval by the University Hospitals ethics committee.
Methods
Childhood Autism Rating Scale (CARS)
The severity of symptoms of autism was assessed by the Childhood Autism Rating Scale (CARS) [17]. The threshold for the diagnosis is a CARS score value of 30, which ranges from 15 to 60.
Wechsler Intelligence Scale for Children
Both groups’ IQs were measured using the Wechsler Intelligence Scale for Children [18].
Electroencephalogram (EEG)
It was done for both groups to assess the electrical activity of the brain in both groups.
Serum level of BDNF
To prevent potential changes in BNDF levels, between 8:00 and 10:00 a.m., blood samples were taken, and throughout the first 30 min, the resultant sera were then stored for the next four hours at − 80 °C [19].
A commercial ELISA kit Cat. No: E1302Hu (Biosensis Mature BDNF ELISA Kit, Thebarton, Australia) was used to check the BDNF level in the serum samples. Samples, equipments, reagents, and standards dilutions were prepared according to the manufacturer’s guidelines. The procedure of the assay included two wells, one with no material and the other labelled with biotin or streptavidin-HRP for the anti-BDNF antibody. The standard wells then included the following: a 50 μl of a ready standard solution containing the labelled anti BDNF antibody with 50 μl of streptavidin-HRP was applied to each well. Moreover, sample wells to be tested included the following: a 40-μl sample, a 10-μl BDNF antibodies, and a 50-μl streptavidin-HRP. The prepared plate was covered and sealed, shacked for proper mixing, and then incubated at 37 °C for 60 min. Proper washing was done, and then each well was filled with 50 μl of solution A (chromogen solution) and then another 50 μl of solution B (chromogen solution). The plate was then gently shook and kept the mixture dark and at 37 °C for 10 min. In order to halt the reaction, the stop solution was finally added to each well. Subsequently, within 10 min, the OD values were read, and concentrations were calculated. Each sample was tested twice for BDNF levels, and the resulted mean of two values was used for statistical analysis. The assay’s sensitivity was 0.01 ng/ml, while the intra-assay and inter-assay coefficients of variance were at 4.31% and 6.6%, respectively.
Statistical analysis
Version 23 of the statistical programme for social sciences was used to analyse the statistics that was obtained (SPSS Inc., Chicago, IL, USA). The Shapiro–Wilk and Kolmogorov–Smirnov tests were used to determine whether the data was normal. The following tests were carried out: first of all, when comparing two means of independent samples, the t-test of significance was applied. Secondly, the Mann–Whitney U-test was used in nonparametric data for two-group comparisons. Moreover, to compare the proportions between qualitative factors, the chi-square (χ2) test of significance was also applied. If one or both of the variables were skewed, Spearman’s rank correlation coefficient (rs) was employed to measure the degree of relationship between them. A receiver operating characteristic (ROC) curve research was conducted to assess the overall predictability of the parameter and determine the optimal cut-off value at which both sensitivity and specificity could be detected.
Results
Regarding the demographic data of both groups, out of the 60 ASD children, 80% were boys with a mean age of 6.80 ± 2.78 years old. Moreover, their mothers mean age was 28.03 ± 5.28 years old, whereas the father mean age was 33.48 ± 5.6414 years old. This is in comparison to the control groups’ 60 healthy controls; 66.7% of them were boys, with a mean age of 7.33 ± 2.91 years old. Their mothers mean age was 27.22 ± 4.37 years old, whereas the father mean age was 32.70 ± 4.87 years old, the age of the child, gender, mother, or father age did not differ statistically significantly between the two groups with the P-value (P > 0.05) (Table 1).
Regarding the clinical data of both groups, as for the IQ, the mean of the ASD group was 63.20 ± 8.79 SD, whereas the mean of the control group was 93.42 ± 10.5 SD, with a statistically significant difference, with the P-value (P < 0.001). EEG changes were positive in 16.7% of the ASD group versus in 8.3% in the control group, with no statistically significant difference between the groups, with the p-value (P > 0.05). The mean CARS score among the ASD group was 33.77 ± 4.41 SD. Among the ASD group, 80% of them were on omega-3 preparations; 66.7% of them were on antipsychotic medications, while 51.7% of them were on behavioural therapy.
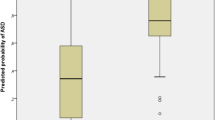
Regarding the BDNF level, the ASD group had a significantly higher mean level of BDNF than the normally developed control group 5.50 ± 2.05 ng/ml versus 1.61 ± 1.75 ng/ml, respectively, with the P-value (P < 0.001) (Fig. 1).

The box plot between patients group and control group according to BDNF showing patients had significant higher levels of BDNF with P-value < 0.001
The mean BDNF level in cases with severe ASD was 6.34 ± 2.82 SD, whereas the level in mild to moderate ASD cases was 5.08 ± 1.39 SD. The different cases and control groups using a cut-off value of P > 2.8 ng/ml of BDNF showed a strong discriminating chance between patients with ASD and typically developing children, with the aspects of sensitivity and specificity being 88.3% and 80%, respectively (Fig. 2).

ROC curve analysis exhibits effective discriminating power of the BDNF between control and patients autistic children at a cut-off value of > 2.8, with sensitivity and specificity being 88.3% and 80%, respectively
Regarding the correlates with the BDNF level, there was a highly statistically significant positive association between the CARS score and the BDNF level (P < 0.001) (Fig. 3).

The scatter plot showing a strong significant association between BDNF and CAR scale with P-value < 0.001
There was a statistically lower BDNF that was found in ASD children who received omega-3 than in others without omega-3 supplementation (P = 0.040) (Table 2). However, there was no correlation between the use of antipsychotics, brain non-stimulants, or behavioural therapy with BDNF level.
Discussion
Although there are many researches and studies that were done to find out a biomarker for the diagnosis or severity of autism, autism still remains one of the most difficult disorders to be biochemically diagnosed [20]. The BDNF is emerging as a promising chemical that could aid in the understanding of a variety of neurodevelopmental illnesses.
In the study, 60 autistic Egyptian children were compared to 60 age- and sex-matched normally developing controls for their serum BDNF levels in order to assess the serum BDNF’s suitability for the diagnosis of ASD patients. Overall, the current study found a substantial difference in blood BDNF concentrations in autistic children with a high discriminating capacity when compared to controls. This was supported by other studies, like in the ones done by Barbosa et al., Meng et al., and Miyazaki et al. [3, 21, 22], which revealed that the BDNF concentrations were higher in children with autism than in the controls (34.38 ± 2.81 and 31.24 ± 3.75 ng/ml) with (P < 0.000).
The enhanced BDNF response in some autism patients is thought to represent an immune cell response that is dysregulated in autism. Different BDNF responses were identified within the autistic group depending on the time of onset. That is because the early onset as well as severe forms of ASD show a higher level of BDNF [23].
Another hypothesis for higher BDNF levels in autism is that BDNF and its receptor, TrkB, cause synaptic transmission activation. Other receptors, like FMRP and PTEN, as well as TSC1/2, inhibit these excitations under normal settings. Without this negative regulation, excitatory activity would be uncontrollable in pathological situations [24]. As a result, it is reasonable to speculate that synaptic disruption may be implicated in the formation and progression of autistic symptoms. Elevated BDNF levels may therefore contribute to neuronal synaptic dysfunction.
This study found a statistically significant positive association between the CARS score and the BDNF (P < 0.001) which was consistent with Meng et al., [21], whereas there was a substantial correlation between blood BDNF levels and CARS scores, with the mean CARS score being 43.5 points (SD 4.7), r [Spearman] = 0.328, P < 0.0001). On the other hand, the study of Barbosa et al., [3] showed a correlation between CARS and BDNF levels, but it was not statistically significant (P = 0.632).
It has been proposed that the brain volume expansion of early ASD children’s is mostly caused by enhanced proliferation of neural precursor cells. Neurotrophic factors boost the growth of embryonic progenitor cells that produce neurons. The appropriate growth and the function of the nervous system depend on the temporally controlled amounts of BDNF that are present during development [25]. Consequently, in the early stages of autism, aberrant BDNF regulation results in future long-term abnormalities in brain function and structure. Additionally, it has been noted that disruption in brain development in autistic children occurred before the majority of clinical characteristics of the condition, increasing the likelihood of the BDNF abnormalities seen in ASD children contributing to the overgrowth in the brains of early ASD children. For these reasons, using BDNF blood levels as a diagnostic tool for ASD is recommended [26].
In this research, the mean IQ for the cases was 63.20 ± 8.79 SD compared with 93.42 ± 10.55 SD for the controls with a significant difference with the p-value < 0.001, yet there was no significant correlation with the BDNF level among the patients group. This did not match the findings of Bryn et al. [27] and Meng et al. [21] as there was a statistically significant negative relation between the BDNF levels in serum and in IQ (P < 0.0001). This discrepancy in the results can be explained as all ASD patients enrolled in these studies had good cognitive functions, i.e., an IQ level of more than 70 at least.
The structural elements of cell membranes, particularly in the central nervous system, include omega-3 long-chain polyunsaturated fatty acids, especially docosahexaenoic acid. These acids promote the development and differentiation of nervous system, synapses, visual acuity, and even the control of gene expression. Moreover, they also control systems that combat inflammation and oxidative stress [28].
The current research examined the relationship between omega-3 supplementation and the synaptic dysfunction marker (BDNF) level in autistic patients because synaptic dysfunction, impaired fatty acid metabolism, and decreased omega-3 fatty acids have been related to the underlying etiology of neurodevelopmental disorders [29]. While studies like Avraham et al. [30] and Doaei et al. [31] and Weiser et al. [32] reported that oral supplementation with docosahexaenoic acid improved autism spectrum behaviours in kids with ASD, they did not however assess its impacts on the neural biochemical markers. Other studies, like Mankad et al. [33] and Voigt et al. [34], discovered a negative role of this supplementation.
Consequently, in the current study, by comparing the serum BDNF levels in children with ASD who received omega-3 to the ones in others without omega-3 supplementation, those who received the supplement orally on a regular basis for 3 months had significantly lower BDNF levels. This suggests that omega-3 may indeed play a protective role against synaptic dysfunction.
This positive effect of omega-3 fatty acids supplementation on serum BDNF levels may also suggest that people with ASD have a weak endogenous intrinsic antioxidant system which may be the cause behind the patients’ synaptic dysfunction, opening the door to using biochemical markers to ascertain the kinds of antioxidants given to ASD patients in order to assess any potential therapeutic effects. Further research is still required though.
Implication and limitations
There are ongoing disputes over autism’s fundamental mechanisms despite extensive research into the disease. The results of this study add to the body of data about the precursor-product molecule unbalance, and the contribution of BDNF in the etiology of autism can help with targeted interventions to restore the balance of metabolites and reduce symptoms of social impairment.
The study does, however, have significant drawbacks. First, the number of participants was relatively too small to declare that this serum parameter may be a predictor of the severity and progression of ASD. As the marker was only obtained peripherally, its validity for issues with the brain is questionable. Moreover, possibility that antipsychotics could affect the BDNF levels has to be more investigated in further studies. The current study has another limitation which is the lack of measurement of omega-3 levels, so further researches and trials studies are required to pinpoint the precise effects of exogenous antioxidant on the clinical features and neurobiochemical markers of autism. However, this study can be considered as a nucleus for further researches to study pathogenesis of increased BDNF in autism.
Conclusion
This study findings enhance the role of BDNF in autism and its use as a diagnostic as well as a characterization marker of severity in autism spectrum disorders. Its affection by omega-3 fatty acid supplementation may make researchers wonder whether oxidative stress plays a part in synaptic dysfunction and subsequently in the onset and progression of disease.
Availability of data and materials
Data is offered on demand due to privacy of patients.
Abbreviations
- ASD:
-
Autism spectrum disorder
- BDNF:
-
Brain-derived neurotrophic factor
- CARS:
-
Childhood Autism Rating Scale
- ELISA:
-
Enzyme-linked immunosorbent assay
- DSM V:
-
Diagnostic and Statistical Manual of Mental Disorders
References
Kasarpalkar NJ, Kothari ST, Dave UP (2014) Brain-derived neurotrophic factor in children with autism spectrum disorder. Ann Neurosci 21(4):129–133. https://doi.org/10.5214/ans.0972.7531.210403
Hansen SN, Schendel DE, Parner ET (2015) Explaining the increase in the prevalence of autism spectrum disorders: the proportion attributable to changes in reporting practices. JAMA Pediatr 169(1):56–62. https://doi.org/10.1001/jamapediatrics.2014.1893
Barbosa AG, Pratesi R, Paz GSC, Dos Santos MAAL, Uenishi RH, Nakano EY, Gandolfi L, Pratesi CB (2020) Assessment of BDNF serum levels as a diagnostic marker in children with autism spectrum disorder. Sci Rep 10(1):17348. https://doi.org/10.1038/s41598-020-74239-x
Van Naarden Braun K, Pettygrove S, Daniels J, Miller L, Nicholas J, Baio J, Schieve L, Kirby RS, Washington A, Brocksen S, Rahbar H, Rice C, Centers for Disease Control and Prevention (2007) Evaluation of a methodology for a collaborative multiple source surveillance network for autism spectrum disorders–Autism and Developmental Disabilities Monitoring Network, 14 sites, United States. MMWR Surveill Summ 56(1):29–40
Balasubramanian B, Bhatt V, C., & A Goyel, N. (2009) Genetic studies in children with intellectual disability and autistic spectrum of disorders. Indian J Hum Genet 15(3):103–107. https://doi.org/10.4103/0971-6866.60185
Zoghbi HY (2003) Postnatal neurodevelopmental disorders: meeting at the synapse? Science (New York, NY) 302(5646):826–830. https://doi.org/10.1126/science.1089071
Hatton DD, Sideris J, Skinner M, Mankowski J, Bailey DB Jr, Roberts J, Mirrett P (2006) Autistic behavior in children with fragile X syndrome: prevalence, stability, and the impact of FMRP. Am J Med Genet A 140A(17):1804–1813. https://doi.org/10.1002/ajmg.a.31286
Balaratnasingam S, Janca A (2012) Brain derived neurotrophic factor: a novel neurotrophin involved in psychiatric and neurological disorders. Pharmacol Ther 134(1):116–124. https://doi.org/10.1016/j.pharmthera.2012.01.006
Foltran RB, Diaz SL (2016) BDNF isoforms: a round trip ticket between neurogenesis and serotonin? J Neurochem 138(2):204–221. https://doi.org/10.1111/jnc.13658
Kowiański P, Lietzau G, Czuba E, Waśkow M, Steliga A, Moryś J (2018) BDNF: a key factor with multipotent impact on brain signaling and synaptic plasticity. Cell Mol Neurobiol 38(3):579–593. https://doi.org/10.1007/s10571-017-0510-4
Santarone ME, Zambrano S, Zanotta N, Mani E, Minghetti S, Pozzi M, Villa L, Molteni M, Zucca C (2023) EEG features in autism spectrum disorder: a retrospective analysis in a cohort of preschool children. Brain Sci 13(2):345. https://doi.org/10.3390/brainsci13020345
Roy N, Barry RJ, Fernandez FE, Lim CK, Al-Dabbas MA, Karamacoska D, Broyd SJ, Solowij N, Chiu CL, Steiner GZ (2020) Electrophysiological correlates of the brain-derived neurotrophic factor (BDNF) Val66Met polymorphism. Sci Rep 10(1):17915. https://doi.org/10.1038/s41598-020-74780-9
Li G, Lu C, Li S, Kang L, Li Q, Bai M, Xiong P (2023) Correlation study of brain-derived neurotrophic factor, EEG γ activity and cognitive function in first-episode schizophrenia. Brain Res 1820:148561. https://doi.org/10.1016/j.brainres.2023.148561
Karege F, Schwald M, Cisse M (2002) Postnatal developmental profile of brain-derived neurotrophic factor in rat brain and platelets. Neurosci Lett 328(3):261–264. https://doi.org/10.1016/s0304-3940(02)00529-3
Fernandes BS, Steiner J, Berk M, Molendijk ML, Gonzalez-Pinto A, Turck CW, Nardin P, Gonçalves CA (2015) Peripheral brain-derived neurotrophic factor in schizophrenia and the role of antipsychotics: meta-analysis and implications. Mol Psychiatry 20(9):1108–1119. https://doi.org/10.1038/mp.2014.117
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders: DSM-5 5th edn, 947. American Psychiatric Association, Washington, DC
Schopler E, Reichler RJ, DeVellis RF, Daly K (1980) Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J Autism Dev Disord 10(1):91–103. https://doi.org/10.1007/BF02408436
Kort W, Compaan EL, Bleichrodt N, Resing WCM, Schittekatte M, Bosman M, Vermeir G, Verhaeghe P (2002) Nederlandse bewerking van de Wechsler Intelligence Scale for Children III (WISC-III). Test en handleiding. Design, NIP Dienstencentrum
Katoh-Semba R, Wakako R, Komori T, Shigemi H, Miyazaki N, Ito H, Kumagai T, Tsuzuki M, Shigemi K, Yoshida F, Nakayama A (2007) Age-related changes in BDNF protein levels in human serum: differences between autism cases and normal controls. Int J Dev Neurosci 25(6):367–372. https://doi.org/10.1016/j.ijdevneu.2007.07.002
Autism Genome Project Consortium, Szatmari P, Paterson AD, Zwaigenbaum L, Roberts W, Brian J, Liu XQ, Vincent JB, Skaug JL, Thompson AP, Senman L, Feuk L, Qian C, Bryson SE, Jones MB, Marshall CR, Scherer SW, Vieland VJ, Bartlett C, Mangin LV, … Meyer KJ (2007) Mapping autism risk loci using genetic linkage and chromosomal rearrangements. Nat Genet 39(3);319–328. https://doi.org/10.1038/ng1985
Meng WD, Sun SJ, Yang J, Chu RX, Tu W, Liu Q (2017) Elevated serum brain-derived neurotrophic factor (BDNF) but not BDNF gene Val66Met polymorphism is associated with autism spectrum disorders. Mol Neurobiol 54(2):1167–1172. https://doi.org/10.1007/s12035-016-9721-9
Miyazaki K, Narita N, Sakuta R, Miyahara T, Naruse H, Okado N, Narita M (2004) Serum neurotrophin concentrations in autism and mental retardation: a pilot study. Brain Develop 26(5):292–295. https://doi.org/10.1016/S0387-7604(03)00168-2
Sun JJ, Chen B, Yu T (2022) Construction of an immune-related ceRNA network to screen for potential diagnostic markers for autism spectrum disorder. Front Genet 13:1025813. https://doi.org/10.3389/fgene.2022.1025813
Gandhi T, Lee CC (2021) Neural mechanisms underlying repetitive behaviors in rodent models of autism spectrum disorders. Front Cell Neurosci 14:592710. https://doi.org/10.3389/fncel.2020.592710
Qin XY, Feng JC, Cao C, Wu HT, Loh YP, Cheng Y (2016) Association of peripheral blood levels of brain-derived neurotrophic factor with autism spectrum disorder in children: a systematic review and meta-analysis. JAMA Pediatr 170(11):1079–1086. https://doi.org/10.1001/jamapediatrics.2016.1626
Saghazadeh A, Rezaei N (2017) Brain-derived neurotrophic factor levels in autism: a systematic review and meta-analysis. J Autism Dev Disord 47(4):1018–1029. https://doi.org/10.1007/s10803-016-3024-x
Bryn V, Halvorsen B, Ueland T, Isaksen J, Kolkova K, Ravn K, Skjeldal OH (2015) Brain derived neurotrophic factor (BDNF) and autism spectrum disorders (ASD) in childhood. Eur J Paediatr Neurol 19(4):411–414. https://doi.org/10.1016/j.ejpn.2015.03.005
Agostoni C, Nobile M, Ciappolino V, Delvecchio G, Tesei A, Turolo S, Crippa A, Mazzocchi A, Altamura CA, Brambilla P (2017) The role of omega-3 fatty acids in developmental psychopathology: a systematic review on early psychosis, autism, and ADHD. Int J Mol Sci 18(12):2608. https://doi.org/10.3390/ijms18122608
Cecerska-Hery´c E, Polikowska A, Serwin N, Roszak M, Grygorcewicz B, Hery´c R, Michalczyk A, Dołęgowska B (2022) Importance of oxidative stress in the pathogenesis, diagnosis, and monitoring of patients with neuropsychiatric disorders, a review. Neurochem Int 153, Article 105269. https://doi.org/10.1016/j.neuint.2021.105269
Avraham Y, Berry EM, Donskoy M, Ahmad WA, Vorobiev L, Albeck A, Mankuta D (2019) Beta-carotene as a novel therapy for the treatment of “autistic like behavior” in animal models of autism. Behav Brain Res 364:469–479. https://doi.org/10.1016/j.bbr.2017.09.041
Doaei S, Bourbour F, Teymoori Z, Jafari F, Kalantari N, Abbas Torki S, Ashoori N, NematGorgani S, Gholamalizadeh M (2021) The effect of omega-3 fatty acids supplementation on social and behavioral disorders of children with autism: a randomized clinical trial. Wpływ suplementacji kwas´ow tłuszczowych omega-3 na zaburzenia społeczne i behawioralne u dzieci z autyzmem: badanie kliniczne z randomizacją. Pediatr Endocrinol Diab Metabol 27(1):12–18. https://doi.org/10.5114/pedm.2020.101806
Weiser MJ, Mucha B, Denheyer H, Atkinson D, Schanz N, Vassiliou E, Benno RH (2016) Dietary docosahexaenoic acid alleviates autistic-like behaviors resulting from maternal immune activation in mice. Prostaglandins Leukotrienes Essent Fatty Aci 106:27–37. https://doi.org/10.1016/j.plefa.2015.10.005
Mankad D, Dupuis A, Smile S, Roberts W, Brian J, Lui T, Genore L, Zaghloul D, Iaboni A, Marcon PM, Anagnostou E (2015) A randomized, placebo-controlled trial of omega-3 fatty acids in the treatment of young children with autism. Molecular Autism 6:18. https://doi.org/10.1186/s13229-015-0010-7
Voigt RG, Mellon MW, Katusic SK, Weaver AL, Matern D, Mellon B, Jensen CL, Barbaresi WJ (2014) Dietary docosahexaenoic acid supplementation in children with autism. J Pediatr Gastroenterol Nutr 58(6):715–722. https://doi.org/10.1097/MPG.0000000000000260
Acknowledgements
Not applicable
Funding
This study did not receive any fund from funding organizations.
Author information
Authors and Affiliations
Contributions
Conceptualization, REK and SAA. Funding acquisition, SAA and MMA. Collection of samples and patient data, SAA, MMA, and REK. Supervision, SAA, MMA, and REK. Original draft writing, SAA, MMA, and REK. Review and editing, SAA and MMA.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The 1964 Helsinki Declaration, its later amendments, and similar ethical standards, as well as the institution’s or ethics committee’s ethical standards, were all followed in all procedures carried out in research involving human subjects. The ethical commission of Ain Shams University gave its approval (FMASU R283). Every individual taking part in the study gave their informed consent. Participants provided clear, fully informed consent for the use of their anonymized data in publications and research. Children and teenagers who took part in the intervention provided written, fully informed consent for the use of anonymized data for publishing and research as well as for the purpose of service evaluation.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elhamid, S.A.A., Alkherkhisy, M.M. & Kasem, R.E. Assessment of brain-derived neurotrophic factor levels in serum of children with autism spectrum disorders. Middle East Curr Psychiatry 31, 18 (2024). https://doi.org/10.1186/s43045-024-00403-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-024-00403-y