
Abstract
Background
With the rise of fragility, conflict, and violence (FCV), understanding the prevalence and risk factors associated with common mental disorders (CMD) is beneficial to estimate the disease burden, redirect of available resources and design evidence-based interventions to mitigate the rising issue among war affected population. Mental disorders are most likely to be elevated in Libyan population, possibly triggered by the triple challenges of long-standing civil conflict, economic shocks, and the coronavirus disease 2019 (COVID-19) pandemic. Although many other mental health variables are salient, this review focused only on posttraumatic stress disorder (PTSD), depression and anxiety, because these are the outcome indices that have been studied sufficiently in Libya. The purpose of this review is to investigate the prevalence of PTSD, depression and anxiety and associated risk factors within the Libyan context, and to assess and identify the resources needed to address this continually rising alarming health issue.
Methods
A search was completed in the academic databases: PubMed, Web of Science, BMJ, Science Direct, Springer Link, Mandumah, ALMANHAL (Arabic Database) from the start of Libyan war February 2011 till January 2023. In addition, hand search was conducted to source additional data. Only studies that investigated prevalence and associated risk factors of PTSD, depression and anxiety in Libya were included. A total of 506 studies were identified of which 33 met the inclusion criteria for this review. There were ten studies investigated the prevalence of post-traumatic stress disorder, twenty studies were focused on depression, while eighteen studies evaluated anxiety. The sample size for all the included studies ranged from 19 to 31,557.
Results
The aggregate prevalence of PTSD, depression, and anxiety was 25.23%, 23.68%, and 14.93%, respectively, which is alarming high comparing to the global prevalence, and it requires immediate intervention. The studies further concluded that several demographic variables such as young age, female, single, educated, loss of employment, with financial difficulties, and victims of domestic violence were significantly associated with PTSD, depression, and anxiety.
Conclusion
In conclusion, the results from this systematic review will help in informing healthcare practitioners, planners, and policymakers on the burden of common mental disorders in Libya and enable them to develop evidence-based policy initiatives, health awareness campaign and intervention programs for mental health disorders in Libya.
Similar content being viewed by others


Introduction
Ten years after the Arab Spring and the collapse of the regime of Muammar Gaddafi in Libya, the destabilizing and deadly conflict between warring factions has not ended despite mediation efforts from the international community. Four periods of instability have characterized Libya's crisis. First, in 2011, having been influenced by revolts in other Arab countries, a popular uprising in Libya triggered a city-based revolt and the overthrow of the four decades of longstanding dictatorship Qaddafi regime. From 2012 through early 2014, the transitional political process was driven by opposing armed factions, including the emergence of Islamist militants. The ‘Second Libyan Civil War’ started in 2014 when General Khalifah Haftar launched an insurgency against Islamist factions in Benghazi. In 2017, violence occurrences decreased considerably compared to 2016, owing mostly to the defeat of Islamic State (IS) terrorists. However, the advance of the Haftar Libyan National Army towards Tripoli in 2019 provoked more conflicts until the Haftar forces were driven by the United Nation-backed Government of National Accord in mid-2020 [1]. Rival governments in the country’s East and West, factionalism, militia warfare and foreign interference have all contributed to a complex conflict that still has no resolution in sight [2].
The lengthy conflict is taking a heavy toll on the Libyan economy and the well-being of the population, causing a significant loss of economic potential in Libya, estimated at 783.4 billion Libyan dinars from 2011 till September 2021 [3], affecting all aspects of economic life in the country. Moreover, the country’s production of oil has also been obstructed by the conflict, the main source of income in Libya, which has been steadily declining over the years to reach around 0.38 million barrel per day (bpd) in 2016, which is less than one fourth of pre-revolution levels. As a result, the Libyan economy shrank by an estimated 2.5% in 2016 [4], Gross domestic product (GDP) per capita estimates in 2021 stood at about half of its value in 2010 before the start of the conflict. The war in Ukraine and multiple waves of the COVID-19 pandemic has further fueled inflationary pressures, further deteriorating household welfare. The cost of the Minimum Expenditure Basket and its food portion rose respectively by 37 and 41 percent year-on-year in April 2022 [5].
COVID-19 has been proposed as a serious event that has had a significant impact on the mental well-being of the population worldwide [6]. The plunge in the Libyan economy and COVID-19 Pandemic lockdowns exacerbated the impact of the conflict on the welfare and poverty outcome of the people. The reduction in oil revenue led to a sharp decrease in government spending and a rise in unemployment. Many health facilities were forced to close due to the violence or lack of medicines, supplies, and medical personnel. Many schools were closed, and there were increased commodity prices, disruption of salary payments, and hindered access to food and essential services.
Mental disorders contribute significantly to the global burden of disease, with common mental disorders (CMDs) such as depression, anxiety and post-traumatic stress disorders (PTSD) accounting for 41.9% of the burden [7], evidence indicates that exposure to conflict-related potentially traumatic events (PTE) will lead to an elevation in the prevalence of mental disorders among exposed sections of the Libyan population [8, 9], although many other mental health variables are salient, this review focused only on PTSD, depression and anxiety, because these are the outcome indices that have been studied sufficiently in Libya., WHO in 2019 estimated that approximately one in five people in post-conflict settings has depression, anxiety disorder, post-traumatic stress disorder [10], it was estimated that about 40% of the most conflict-affected populations could be suffering from PTSD, with 30% of these cases considered to be severe. More than a third could have depression, with around half of these experiencing the most severe form of the illness. Additionally, they found a high degree of co-morbidity between the two disorders with half of those experiencing PTSD estimated to be also suffering from depression, and more than 60% who suffers from anxiety will also have symptoms of depression and vice versa [11]. In this particular study, it is estimates show that more than 120,000 Libyans are predicted to have the most severe form of PTSD while more than 220,000 are predicted to have severe depression [12].
Though it’s important to note, a useful finding from a study for field researchers who use self-report or symptom-based measures to ascertain mental disorder prevalence estimates is that these instruments were shown to significantly overestimate the prevalence of depression, PTSD, and anxiety by 1·5 to 2 times. Most of these instruments do not assess clinical significance or function, and hence can overestimate prevalence of disorders compared with diagnostic instruments [10].
Its estimated that 14.3% of deaths worldwide, or approximately 8 million deaths each year, are attributable indirectly to mental disorders, and efforts are needed to quantify and address the global burden of illness to better consider the role of mental disorders in preventable mortality, reduction of this burden will require a focus on less prevalent but more severe diagnoses and more common mental disorders [13] systematic review of research plays an important role in the process of translating scientific evidence into patient care decisions, allowing the clinical practice to be organized based on scientific evidence from multiple studies and identifying new research topics, thus contributing to the development of science [14]. This study is a cornerstone toward finding possible solutions, and highlighting key problems during a time where mental health issues are easily overlooked. In my opinion, it carries important practical implications, as it assists in identifying groups that are vulnerable to mental health risks during and after the war, making it possible to target psychiatric care to people of the studied groups. This knowledge is essential for planning appropriate forms of help.
The purpose of this study is to investigate the prevalence of posttraumatic stress disorder (PTSD), depression and anxiety and associated risk factors within the Libyan context, and to assess and identify the resources needed to address this continually rising alarming health issue.
Methods
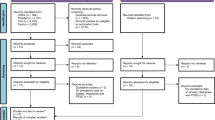
The systematic review was reported according to the Preferred Reporting Items of Systematic Review and Meta-Analyses (PRISMA) guidelines. A flow diagram of the literature search based on the PRISMA is presented in (Fig. 1). The search was conducted in the following English academic databases: PubMed, Web of Science, BMJ, Science Direct, Springer Link, and Arabic databases: Mandumah, ALMANHAL from February 2011 the start of Libyan war till January 2023, hand search was also conducted to source additional data, which included reference lists of relevant review papers which were manually searched for articles that may not have been identified in the literature search and also we searched through search engines (Google Scholar, Research gate); however, it was limited to the first 50 pages and included only the most relevant articles. The following search terms were used relating to five categories: (1) PTSD (post-traumatic stress disorder or posttraumatic stress disorder or posttraumatic stress or posttraumatic syndrome or PTSD; (2) depression (depression or major depression or depress); (3) anxiety (anxious, generalized anxiety disorder, anxiety); (4) mental health (mental Illness or mental health or mental disorder); (5) Libya. The search was conducted that at least one term in the categories Depression, PTSD, Anxiety or Mental Health had to be reported in titles, abstracts, or key concepts in the respective database, along with the term Libya.

Flow diagram of the literature search based on the PRISMA
Inclusion and exclusion criteria
Studies that measured the prevalence rates of at least one common mental disorder (PTSD, depression, and generalized anxiety disorder) in Libyan population who lived in Libya during or after the civil war (2011). Only those studies that utilized validated quantitative screening tools or formal diagnoses of a common mental disorders, in line with either the criteria set by the International Classification of Diseases (ICD), Diagnostic and Statistical Manual of Mental Disorders (DSM), Fourth or Fifth Edition were included. We considered all study designs for this review with no language restrictions except for case reports, poster publication, systematic reviews, meta-analyses, editorials, and articles with qualitative-only methods. Primary inclusion and exclusion criteria for this review are represented in Table 1.
Data extraction
Data was extracted from the 33 studies included within this review, the extracted data included study design, location, prevalence rates, sampling, and data collection methods, as well as the adopted measurement tool. We also extracted information on a few demographic data which have been previously reported in the literature as potential variables that may influence the prevalence rates of common mental disorders such as age, sex, and study population characteristics as shown in Table 2
Quality assessment and risk of bias
Methodological quality and risk of bias was assessed using the (Damian Hoy et al.) Quality assessment checklist for prevalence studies. It consists of nine questions that assesses the representativeness of the sample, the sampling technique, the response rate, the data collection method, the measurement tools, the case definitions, and the statistical reporting. Each checked question was scored either as “1” or “0” corresponding respectively to “low risk of bias” and “high risk of bias”. The total. score ranged from 0 to 9 with the overall score categorized as follows: 0 to 3: “low risk of bias”, 4 to 6: “moderate risk”, and 7 to 9: “high risk”. In all, 33 studies were categorized as having a low risk of bias while one study had a moderate risk of bias as shown in Table 3
Results
PTSD
Prevalence of PTSD
Ten studies out of 33 measured the prevalence of PTSD in Libyan population, which presented with a significant heterogeneity, it ranged between 19.8 and 100%). This is a common problem in the epidemiology of mental health disorders where prevalence often varies widely across studies. Variation in prevalence can be due to factors such as differences in sampling, measurement, geographic area, population group, and other factors. For instance, regarding sampling high-risk clinical samples is likely to account for some of the variation; high-risk samples in the included studies (veterans, militias, war injured, and IDP’s) were more likely to report PTSD compared to community samples (teachers, undergraduate students). The most common tool used to assess PTSD was PTSD PCL (n = 5), IES-R (n = 2), CAPS (n = 1), Davidson Trauma Scale (n = 1), andCRIES-8 (n = 1).
Most research has assessed PTSD according to DSM-IV criteria where symptoms of PTSD are grouped into three clusters: (1) re-experiencing the traumatic event through nightmares, intrusive thoughts, or flashbacks; (2) persistent avoidance of reminders of the event and numbing of general responsiveness; and (3) increased arousal such as hypervigilance, irritability, difficulty concentrating, and other emotional dysregulation. To be diagnosed with PTSD, a person must have at least one re-experiencing symptom, three avoidance symptoms, and two symptoms of arousal. Symptoms must cause the person significant distress and impairment in occupational or social functioning [48]
Differences in measurement are also important whether studies measure full diagnostic criteria or only symptoms. Measures with ICD-11 PTSD criteria yield higher prevalence estimates than the DSM-5 criteria [49], self-report measures that do not measure full diagnostic criteria for PTSD might inflate prevalence estimates. For example, studies have found that the prevalence of participants meeting the criteria for PTSD measured by a symptom scale decreased from 20 to 3% when criterion E and F (duration and subjective impairment, respectively) were added [50] and doubled when the criterion A2 (intense emotional response) was removed [51]. Similarly, self-report questionnaires may result in higher prevalence rates than clinical diagnostic interviews [52].
The aggregate prevalence of PTSD across all the 10 studies (25.23%) of total sample size 34,344 of which 12,490 were males and 21,854 were females, consisting mainly of adolescents and adults (above the age of 18), with the exception of one study that measured its prevalence in children between the age 9 and 15 years [44], they were are all prospective studies, except two were retrospective [17, 19], in which their prevalence was based on hospital records. The study design was all cross-sectional except two [20, 40], they all obtained their data mainly from surveys with self-administrated questionnaires apart from two studies, one was through neuropsychiatric examination [17], while the other was structured clinical administrated scale [19]. The samples covered large area across Libya, most of the studies were conducted among one of the three largest cities in Libya (n = 2), Tripoli (n = 3), Benghazi (n = 2), Misrata, and its suburbs, while one of the studies had samples from almost all over Libya (30 cities).
Risk factors of PTSD
Four studies focused on identifying PTSD correlated risk factors, a study consisting of 31,577 participants conducted across 30 cities in Libya focused on demographic variables, for example it identified that females were 1.07 times more likely to have PTSD than males, unmarried people had a 1.39 times higher likelihood of having PTSD than married subjects, PTSD was significantly associated with higher education levels and younger age. Moreover, it identified its association with the war and COVID-19 stressors, for instance, being internally displaced due to civil war was significantly associated with 1.26 times higher odds of exhibiting PTSD, work status changes during the pandemic is statistically associated with increased likelihood of PTSD, Notably, those who were infected with COVID-19 without hospitalization or those who had recent contact with infected patients were statistically associated with higher odds of having PTSD. Participants who reported having suffered from financial issues during the pandemic, exposure to domestic violence or abuse, or suicidal ideation were more likely to have PTSD [21]. Another study endorsed the previous studies in regard to females were more likely to have PTSD than males, and its association with war stressors, indicating the persons who lost loved ones and their homes were statistically associated with increased likelihood of PTSD [43]. In addition, another study stated that living in neighborhood closer to the bombing and shooting increased the chances of developing PTSD [41]; one further study conducted among internally displaced persons further confirmed that females, younger age, and who lived closer to the war zone were more prevalent to develop PTSD [47]. Furthermore, an interesting study investigated successful strategies to mediate PTSD symptoms, it articulated that lower problem-solving strategies were significantly associated with PTSD and other mental health problems amongst children, while their parents’ mental health was more affected by a lack of support-seeking strategies [44].
Depression
Prevalence of depression
Depression is the common cold of mental disorders; most people will be affected by depression in their lives either directly or indirectly, through a friend or a family member. Depression is characterized by a number of common symptoms. These symptoms include persistent sadness, anxiety and feelings of guilt, worthlessness, and hopelessness. They no longer take interest or pleasure in hobbies and activities they were once enjoyed [35].
Twenty studies measured the prevalence of depression among Libyan citizens, ranging between 4.3 and 85.2%, and there is considerable heterogeneity in the datasets and their reported estimates, which created large uncertainty around the predicted estimates. This heterogeneity stemmed partly from differences across sample background such as high-risk group would naturally have higher prevalence, as an example war injured had prevalence of (85.9%), IDP’s had a prevalence of (61.8%), it could also be partly accounted for the presence of over 280 rating scales to assess depressive symptoms, and common scales only overlap moderately in symptom content. Clinical diagnoses and self-report measures have been used to determine depression cases but rely on different criteria and identify sets of cases that do not fully overlap. Among the 20 studies, the scaled used were PHQ-9 (n = 5), HADS (n = 3), DASS (N = 3), BDI (n = 2), PHQ-3, KADS, GHQ, GSHS, ACHA, ICD-10, EPDS, and it worth noting that among the five studies that used PHQ-9, four had a cutoff score of 15, while one had cutoff score of 10, which could also attribute to the heterogeneity.
Ten of the included studies addressed the association of depression with the adverse effects of war (n = 10) and five was associated with COVID-19 stressors (n = 5); two studies paid special attention to pregnancy (n = 2), in which the first investigated the correlation between anemic pregnant women and depression; however, it identified that there was no significant association between hemoglobin level and depression during pregnancy [15], and the second study measured the prevalence of postpartum depression and its correlation with sleeping disturbance, state of neonate after birth, excess consumption of stimulants, less weight acceptance by mothers during pregnancy and infant illness [25], it is important to highlight the prevalence among them was terrifying (43.3–60%, respectively); furthermore, a study administered among 104 mothers of autistic children had prevalence of (32.7%) [34]. Five studies identified the alarming prevalence of depression within medical health workers (n = 5) ranging from 10.5 to 73.4% which was conducted among doctors, emergency physician, frontlines physician, surgical staff, nurses, technicians, and pharmacists. Furthermore, four studies focused on its prevalence among undergraduate students (n = 4), two of them were among medical students (n = 2), its prevalence among them is petrifying, one of them was conducted in Tripoli university with sample size of 170, in which 45.8% were diagnosed with depression based on KADS score [36], however it is important to note that the researcher also used (PHQ-9) to measure the degree of depression, resulting in 44.7% mild, 25.8% moderate, 8.8% moderately severe, 1.17% severe; therefore, the depression rate for the same study should be 9.97% based on PHQ-9 with cutoff score was ≥ 15 as other studies included within the systematic review, while the second study was conducted among 2430 medical undergraduates from 15 medical schools across Libya, which had a prevalence rate of 21.6% using the same measuring scale (PHQ-9) [29]; furthermore, the two other studies on undergraduate students used the same study sample, and it was conducted among 1300 undergraduate students at nine higher education institutes across seven cities in Libya; however, they used two different scales to assess the prevalence, the first identified prevalence of 57.6% using GSHS [18], the second study reported only 4.3%; this could be attributed to the fact that used scale ACHA relied on participants admitting they were previously diagnosed with depression, which could not be a valid creditable measure since many are undiagnosed, and Libyan citizen out of fear of mental illness stigma, would not usually admit they are depressed [31].
The aggregate prevalence of depression across all the 20 studies (23.68%) of total sample size 50,551 of which 15,872 were males and 34,679 females, consisting mainly of adolescents and adults (ranging between 14 and 80), and they are all prospective studies, except one was retrospective, in which their prevalence was based on hospital records [19]. The study design was all cross-sectional, except one was case series study [34], and they all obtained their data mainly from surveys with questionnaires apart from two studies was conducted through structured clinical interview (n = 2) [15, 34]. There was widespread area coverage of study samples from Tripoli in the west to Benghazi in the east, and from Misrata in the north to Sabha in the south.
Risk factors of depression
Across the included studies several of social demographic characteristics haven been associated with depression, for example, finding of study among 31,557 person across Libya indicated that younger age was associated with a higher likelihood of depressive symptoms. Females had 1.22 times higher odds of exhibiting depressive symptoms than males. Additionally, unmarried people had 1.63 times higher odds of being depressed than married people. Higher education level was significantly associated with higher odds of being depressed, and those with secondary or university-level education had the highest likelihood of being depressed, while regarding COVID-19 stressors, Individuals whose work was suspended owing to the COVID-19 pandemic or those who turned to teleworking had a higher likelihood of being depressed. Individuals with a previous history of infection with COVID-19 without hospitalization had 1.67 times higher odds of being depressed than those who were not infected, having a relative or loved one infected with COVID-19 was significantly associated with depressive symptoms. Individuals who had financial issues during the pandemic, internal displaced due to civil war, who were exposed to domestic abuse or violence, or had suicidal ideation were more likely to have depressive symptoms [21]. Other studies also endorsed the finding of this study.
Anxiety
Prevalence of anxiety
A total of 18 studies were included in the analysis of anxiety, with a total number of 58,038 participants from different cities across Libya. 5 studies reported the prevalence of anxiety among health care providers, whereas 3 studies reported on the prevalence of anxiety among undergraduate students, 4 studies were among the public, however the remaining other studies each focused on specific group ranging from diabetic patients [33], pregnant women [15], IDP’s [22], mother of autistic child [34], teachers [27], and war injured [19]. In the included studies, the prevalence of anxiety ranged by 8.8–91.4%. The most common tool used to assess depression was the GAD-7 (n = 7), DASS-21 (n = 3), HADS (n = 3), BAI (n = 1), GHQ-28 (n = 1), ACHA (n = 1), MDHS (n = 1), FLSAS (n = 1).
All of the studies assessed General Anxiety with the exception of two studies, one focused on dental anxiety [45], which was highly prevalent (91.4%), as expected since dental fear/anxiety is very common worldwide [53], though the prevalence within this study is still considerably higher than other countries, and another study measured the prevalence of speaking anxiety among EFL students (English as a Foreign Language) to be 84.33% [46], which is also highly prevalent in several of countries [54], including these two specialized type of anxiety caused the high fluctuation in prevalence rate of anxiety among all of the eighteen included studies. It is also imperative to highlight the puzzling variance in the prevalence among medical undergraduate students (64.5%) [29] and other undergraduate students (8.8%) [31], though it could be argued that medical student are subjects to more stressors due to the nature of their studies and it could also be explained by the measuring tool that was used among regular undergraduates (ACHA), which could be delusive, as it’s not an assessment tool, it depends on truthful answering of the students if they have been previously diagnosed with Anxiety, and the fear of mental illness stigma in Libya will make it a misleading tool to measure anxiety within Libyan population. It could be noticed that there is a higher prevalence of anxiety among groups that are highly susceptible to stressors such as IDP (internally displaced persons) due to the unstable living conditions and sudden changes in their lives and loss of their homes (58.6%) [22], and also war injured persons (82.7%) [19] as they have almost faced death, or witness the death of loved ones and have been subjected to heavy bombing and gunshots, which has highly adverse effect on one’s mental health.
The aggregate prevalence of anxiety across all the 18 studies (14.93%) of total sample size 58,038 of which 8670 were anxious, consisting mainly of adolescents and adults, and they are all prospective studies, except one was retrospective [19], in which their prevalence was based on hospital records. The study design was all cross-sectional, except one study was case series study [34], and they all obtained their data mainly from surveys with questionnaires apart from three studies was conducted through structured clinical interview (n = 3). In which 10 of the studies collected their samples from heath care centers, while four of them were gathered from educational facilities.
Risk factors of anxiety
Several of the included studies examined the association of prevalence of anxiety with sociodemographic characteristics, furthermore ten of the studies also examined the association with civil war stressors and COVID-19. In this particular study [21] which explored the association of anxiety with several of factors and found that females were 1.17 times more likely to exhibit anxiety symptoms than males. In addition, unmarried individuals had a 1.31 times higher likelihood of having anxiety symptoms than married participants. Similar, to depressive symptoms, anxiety symptoms were higher in younger ages and those with higher levels of education. Work status during the pandemic was independently associated with anxiety symptoms, especially in those whose workload increased or whose work was suspended during the pandemic. Individuals who suffered from financial issues during the pandemic, internal displacement due to civil war, were exposed to domestic abuse or violence, or had suicidal ideation were more likely to have anxiety symptoms [21]. Another study also supported the previous study finding with respect to age and sex; however, it differed in reference to marital status illustrating that being married was significantly associated with higher likelihood of anxiety symptoms, compared to not being married, furthermore it exhibited that being infected with COVID-19 was associated with 9.59 times higher risk of exhibiting clinically significant anxiety symptoms [23]. Moreover, another study among health care workers endorsed the effect of internal displacement and living in a conflict zone were statistically associated with anxiety symptoms [30].
Discussion
The systematic review was preformed to better understand the prevalence of PTSD, depression, and anxiety and associated risk factors in Libya, creating robust knowledge on this alarming health issue will gain policy-makers attention to fund intervention programs, allocate resources, and help in early identification and treatment of these mental illness, which if detected late it could a heavy burden on the society. Therefore, a study of this manner may warrant inclusion of the findings gathered in this study.
The disability and burden associated with these mental disorders have been well-documented [55], as has their socio-economic impact. The Global Burden of Disease study attributes nearly 15% of years of life lost to mental disorders, making mental illnesses one of the largest causes of disability worldwide; in 2019, it was estimated 418 million disability-adjusted life years (DALYs) could be attributable to mental disorders (16% of global DALYs) [56]. Most epidemiological studies on mental disorders in war survivors have focused on posttraumatic stress disorder (PTSD) and depression. If untreated, both depression and PTSD can become chronic, and contribute significantly to the global burden of disease. Furthermore, comorbid depression and PTSD is characterized by significantly higher levels of psychopathological distress, including suicide risk, than either condition alone [57].
A recent systematic review, which estimated the prevalence of mental disorders in countries of the Eastern Mediterranean Region (EMR) of the World Health Organization (including but not limited to Libya, Egypt, Tunis, Syria, and Yamen), Depressive disorders showed the highest pooled prevalence of current, period, and lifetime prevalence (14.8), followed by generalized anxiety disorder (GAD) (10.4%), post-traumatic stress disorder (7.2%), and it is alarmingly high, though explainable since almost 85% of the EMR population have experienced a humanitarian crisis within the past two decades [58]. Arab spring commenced in Tunisia, followed by Egypt then Libya, all neighboring Arab north African countries, even though the uprising in Egypt and Tunis lasted for less than a month and did not involve weapons and civil war unlike Libya which lasted for 8 months and over a decade of civil unrest; however, they still both faced aggressive military oppressions, political instability, economic crisis, and COVID-19 stressors. It expected to witness rise in the prevalence of common mental disorder among their population. In Tunis, the prevalence of PTSD 27% [59], depression 13.4% [60], and anxiety 5.51% [61]. However, Egypt PTSD was 16.31% [62], depression 33.33% [62], and anxiety 4.75% [63] (though these figures are not nationality representative due to lack of research in this sector). Further studies are needed to understand the different circumstances among these neighboring countries, to exchange resources, organize working group to discuss and share finding and design strategies for early identification, intervention, and treatment of these mental burdens.
Mental health services in Libya were woefully inadequate before and after the civil war following the Arab Spring of 2011 [64]. Some areas lack mental health services altogether. A study reported that per 100,000 population, the country had approximately 0.2 psychiatrists, 5 psychologists, 0.05 psychiatric nurses, and 1.5 social workers. The number of psychologists is relatively high because it includes therapists, nurses, and social workers interested in psychosocial interventions [65].
The mental healthcare that does exist in Libya is mainly in the form of highly centralized institutional in-patient services. There are two hospital services for the entire population, located in two large cities; they have a total of nearly 2000 beds [64], there are no facilities or services for adolescent or child psychiatry, forensic psychiatry, or older-adult psychiatry. Patients usually present at a very late stage of illness, and most admissions are involuntary. Patients’ family members or other carers normally try to manage the situation without seeking any help, due to stigma. It is more acceptable for spiritual healers to be considered as the first option. The next step is usually the patient’s general practitioner (GP), because it is seen as less stigmatizing. Psychiatrists are generally the last resort for patients and family [66].
There is no formal psychiatric training scheme for clinicians. Qualified doctors usually work as GPs and specialists at the same time, without having to go through a formal training program such as for the Member of the Royal College of Psychiatrists (MRCPsych). Children with behavioral or mental health problems will usually be seen by a pediatrician rather than a psychiatrist [67]. A survey of young children in Benghazi found that mental health problems such as depression and anxiety affected significantly more girls than boys [67]. Unfortunately, there is no system in place for the early detection and management of children with emotional or mental health disorders.
Research and development have been grossly neglected, there being no specific center for research equivalent to the UK’s National Institute for Health Research [66]. This gap in research output constrains improvements in public health and mental health policy and practice.
Limitations of the review
There are multiple limitations that should be considered when interpreting the results of this systematic review. Firstly, this study had a high level of heterogeneity. However, it should also be considered that high heterogeneity is expected when analyzing a large number of studies. Furthermore, there are great differences in the evaluation of depression, anxiety, and post-traumatic stress due to the different tools and questionnaires that are used, differences in assessment tools may also affect the corresponding reported prevalence. Thirdly, due to limitations of time and resources, not all databases such as Scopus, Psycinfo, and Embase, trustable databases, were included in the analysis, which may have left out important studies in the analysis, though given the number of studies included in our analysis, it is unlikely that the results would be substantially affected.
Recommendation for future studies
The majority of research in mental health has been conducted in the west. Therefore, robust methods of culturally validating instruments for the Libyan population are needed, also there is an urgent need for longitudinal studies, since most of the studies included were cross sectional, even though they provide sufficient information on prevalence and risk factors, but they cannot tell us anything about the cause or what the best treatment might be. Additionally, it is evident that there is lack of studies on prevalence of common mental disorder in children, which is of high importance to detect and address, ensuring it would be managed early before it would have long term negative effect on the growth and development of healthy future generation. In addition, it is essential to study impact of these mental illness across generations, and it is imperative to consider that a substantial number of adults in Libya who developed this mental illness are parents with dependent children, which most probably would impair their parenting capabilities negatively, which subsequently would cause psychological, social, and emotional difficulties in children. Furthermore, studies on development of intervention and political advocacy campaigns aiming to reduce mental disease burden in Libya is warranted.
Conclusion
The results of this review may assist policy makers and international organizations by providing the necessary population-based analysis of psychological well-being during the COVID-19 pandemic and the ongoing civil war crisis in Libya. In addition, it may assist during planning awareness or intervention campaigns through targeting the persons who are more likely to develop these common mental based on the findings of the included study.
Availability of data and materials
Not applicable.
Abbreviations
- ACHA:
-
American College Health Association Survey
- BAI:
-
Beck Anxiety Inventory
- BDI:
-
Beck Depression Inventory
- CAPS:
-
Clinician-Administered PTSD Scale
- CMD:
-
Common mental disorders
- COVID-19:
-
Coronavirus disease of 2019
- CRIES:
-
Children's Revised Impact of Event Scale
- DSM:
-
Diagnostic and Statistical Manual of Mental Disorders
- DAS:
-
Depression anxiety stress
- DASS:
-
Depression Anxiety Stress Scales
- DALYs:
-
Disability-adjusted life years
- EMR:
-
Eastern Mediterranean Region
- EPDS:
-
Edinburg postnatal Depression Scale
- FCV:
-
Fragility, conflict and violence
- FLSAS:
-
Foreign Language Speaking Anxiety Scale
- GAD:
-
Generalized anxiety disorder
- GHQ:
-
General Health Questionnaire
- GP:
-
General practitioner
- GSHS:
-
General Student Health Survey
- HADS:
-
Hospital Anxiety and Depression Scale
- ICD:
-
International Classification of Diseases
- IDPs:
-
Internally Displaced Persons
- IES-R:
-
Impact of Event Scale-Revised
- KADS:
-
Kutcher Adolescent Depression Scale
- MDAS:
-
Modified Dental Anxiety Scale
- MRCPsych:
-
Member of the Royal College of Psychiatrists
- PTSD:
-
Post-traumatic stress disorder
- PTE:
-
Potentially traumatic events
- WHO:
-
World Health Organization
- PCL-C:
-
PTSD Checklist–Civilian Version
- PHQ:
-
Patient Health Questionnaire
References
World Bank. Vulnerability, Shocks, and Coping Mechanisms in Libya (English). Washington, D.C. : World Bank Group. http://documents.worldbank.org/curated/en/099050406292237714/P1776930a7bdb309092400c964928e24b6
Hill TM. What’s next for Libya’s protracted conflict? [Analysis and commentary]. The United States Institute of peace; 2022 [Available from: https://www.usip.org/publications/2022/06/whats-next-libyas-protracted-conflict
Asia UNEaSCfW (2021) The economic cost of the Libyan conflict. (United Nation) United Nations Economic and Social Commission for Western Asia (ESCWA). https://www.unescwa.org/publications/economic-cost-libyan-conflict
World Bank. Libya’s Economic Outlook- April 2017 (English). The World Bank Group. https://www.worldbank.org/en/country/libya/publication/economic-outlook-april-2017
Bank TW. Libya's Economic Update — October 2022: The World Bank; 2022 [Available from: https://www.worldbank.org/en/country/libya/overview
Rauch SAM, Simon NM, Rothbaum BO (2020) Rising tide: Responding to the mental health impact of the COVID-19 pandemic. Depress Anxiety 37(6):505–509
Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE et al (2013) Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. The lancet 382(9904):1575–1586
Summerfield D (2000) War and mental health: a brief overview. BMJ 321(7255):232–235
Attanayake V, McKay R, Joffres M, Singh S, Burkle F Jr, Mills E (2009) Prevalence of mental disorders among children exposed to war: a systematic review of 7,920 children. Med Confl Surviv 25(1):4–19
Charlson F, Van Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S (2019) New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. The Lancet 394(10194):240–248
Kaufman J, Charney D (2000) Comorbidity of mood and anxiety disorders. Depress Anxiety 12(Suppl 1):69–76
Charlson FJ, Steel Z, Degenhardt L, Chey T, Silove D, Marnane C et al (2012) Predicting the impact of the 2011 conflict in Libya on population mental health: PTSD and depression prevalence and mental health service requirements. PLoS ONE 7(7):e40593
Walker ER, McGee RE, Druss BG (2015) Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiat 72(4):334–341
Feldstein DA (2005) Clinician’s guide to systematic reviews and meta-analyses. WMJ 104(3):25–29
Jiji D, Rajagopal K (2014) Assessment of depression anxiety and stress among the anaemia in pregnant women attending selected health care facilities in Sebha, Libya. Asian Pac J Health Sci 1:438–42
Peeran SW, Kumar NP, Azaruk FA, Alsaid FM, Abdalla KA, Mugrabi MH et al (2014) Association between mental well-being, depression, and periodontal attachment level among young adults of the postwar Sebha city, Libya: A pilot study. J Nat Sci Biol Med 5(2):308–312
Dootz F, Von Stackelberg O-M, Abaya J, Jacobi C, Mohs C, Craemer EM et al (2021) Better be prepared: the spectrum of neuropsychiatric impairment among Libyan war victims transferred to Germany for trauma rehabilitation. Neurol Res Pract 3(1):36
El Ansari W, Khalil K, Stock C (2014) Symptoms and health complaints and their association with perceived stressors among students at nine Libyan universities. Int J Environ Res Public Health 11(12):12088–12107
Biçen Ç, Akdemir M, Gülveren D, Dirin D, Ekin A (2021) Depression, anxiety, and post-traumatic stress disorder following orthopedic war injuries. Cureus 13(3):e13792
Mughairbi FA, AbdulazizAlnajjar A, Hamid A (2020) Effects of psychoeducation and stress coping techniques on posttraumatic stress disorder symptoms. Psychol Rep 123(3):710–724
Elhadi M, Msherghi A, Khaled A, Alsoufi A, Alhadi A, Kareem A et al (2022) Impact of lockdown due to the COVID-19 pandemic on mental health among the Libyan population. PLoS ONE 17(4):e0267426
Sryh M, Ozcebe H (2020) Mental health and quality of life assessment among adult internally displaced persons, Tripoli Libya. Eur J Public Health 30:ckaa165
Msherghi A, Alsuyihili A, Alsoufi A, Ashini A, Alkshik Z, Alshareea E et al (2021) Mental health consequences of lockdown during the COVID-19 pandemic: a cross-sectional study. Front Psychol 12:605279
Elhadi M, Msherghi A (2021) Mental health of surgeons during the COVID-19 pandemic: an urgent need for intervention. Surgery 169(2):477–478
Saeed N, Elrayani A, Sherif R, Sherif FM (2022) Postpartum depression and associated risk factors in Libya. 2:79–89
Elhadi M, Khaled A, Malek AB, El-Azhari AE, Gwea AZ, Zaid A et al (2020) Prevalence of anxiety and depressive symptoms among emergency physicians in Libya after civil war: a cross-sectional study. BMJ Open 10(8):e039382
Taher YA, Samud AM, Hashemi MM, Kabuoli NF (2016) Prevalence of depression, anxiety and stress among Libyan primary and secondary schoolteachers: a cross-sectional study= دراسة مستعرضة لمعرفة مدى انتشار الشعور بالاكتئاب والقلق والتوتر بين معلمي المدارس الليبية في المرحلتين الابتدائية والثانوية. Jordan J Pharma Sci 403(3972):1–12
Elhadi M, Alsoufi A, Msherghi A, Alshareea E, Ashini A, Nagib T et al (2021) Psychological health, sleep quality, behavior, and internet use among people during the COVID-19 pandemic: a cross-sectional study. Front Psychiatry 12:632496
Elhadi M, Buzreg A, Bouhuwaish A, Khaled A, Alhadi A, Msherghi A et al (2020) Psychological impact of the civil war and COVID-19 on Libyan medical students: a cross-sectional study. Front Psychol 11:570435
Elhadi M, Msherghi A, Elgzairi M, Alhashimi A, Bouhuwaish A, Biala M et al (2020) Psychological status of healthcare workers during the civil war and COVID-19 pandemic: a cross-sectional study. J Psychosom Res 137:110221
Khalil KA. Rates of anxiety and depression among higher education students In Libya-2015.
Elhadi M, Msherghi A, Elgzairi M, Alhashimi A, Bouhuwaish A, Biala M et al (2021) The mental well-being of frontline physicians working in civil wars under coronavirus disease 2019 pandemic conditions. Front Psych 11:598720
Khrwat A, Saadawi A (2021) Generalized anxiety disorder among diabetic patients visiting gharyan-polyclinic in Libya during COVID-19 pandemic. BJPsych Open 7(S1):S265-S
Benrween A, Alazabi T, Abukash H, Alnajjar N, Ejdeah N, Shileebik M, et al (2022) Psychological distress among Libyan mothers of autistic male children in Tripoli, Libya. AlQalam J Med Appl Sci 5(1):267–73. https://journal.utripoli.edu.ly/index.php/Alqalam/article/view/147
Hnish M (2017) The prevalence of clinical depression among Libyan females of ages 14 to 18 years. J Depress Anxiety 06:278. https://doi.org/10.4172/2167-1044.1000278
Sherif R, Saeed N, Sherif G, Rabab K, Sherif FM, Artículo I (2021) Prevalence of depression among Libyan medical students. Iberoamerican Journal of Medicine 3:196
Abuhajar AM. Cultural values, social support and self-esteem as predictors of depression in a Libyan context (Doctoral dissertation, School of Social Sciences Theses). http://bura.brunel.ac.uk/handle/2438/8286
Lagaa A, Alhoot M, Baobaid M (2022). Knowledge, attitude, perception and psychological status of healthcare workers during COVID-19 outbreak in Libya: a cross sectional study. J Pure Appl Microbiol. 16(2):1370–83. https://microbiologyjournal.org/abstract-16-2-65/
Tresh M (2021) Amid armed conflict: perceptions and the psychological impact of Covid-19 in Western Libya
Stanford MS, Rogers EB, Elverson TM, Padilla JI (2014) Feasibility and efficacy of a peer-led recovery group program for war-related trauma in Libya. South African Journal of Psychology 44(1):97–105
تليب س, Talib S. مدى شيوع اضطراب ضغوط مابعد الصدمة لدى المحاربين الليبيين وفقاً لمتغير السکن - The prevalence of post-traumatic stress disorder among Libyan fighters, according to the housing variable. مجلة البحث العلمي في الآداب - Scientific Research Journal of Arts. 2017;18(2):1–35
Joud دأأ-DAA, Fakeri أما-MA, Musmari دإا-DIA. اضطراب الضغوط التالية للصدمة لدى المعلمين المتضررين من أحداث الحرب في مدينة بنغازي - Post-traumatic stress disorder among teachers affected by war events in Benghazi. المجلة الليبية العالمية - The Libyan International Journal. 2019(44)
Sultan سعم-A. اضطراب ضغوط التالية للصدمة بعد حرب 2011 وعلاقته ببعض المتغيرات لدى عينة من طلاب جامعة مصراتة - Post-traumatic stress disorder after the 2011 war and its relationship to some variables among a sample of Misurata University students: الجامعة الأسمرية الإسلامية - كلية التربية زليتن - Al Asmariya Islamic University - Faculty of Education Zliten; 2017
Farag AAH (2020) The Role Of Social Supports And Copying Strategies In Mediating The Impact Of Civil War On Libyan Children's Mental Health. University of Leicester. Thesis. https://doi.org/10.25392/leicester.data.12652325.v1
Elmasuri GM, Rashidah E (2010) Dental anxiety among adult patients attending the Libyan national health services: Jabatan Pergigian Masyarakat. Universiti Malaya, Fakulti Pergigian
Toubot AM, Seng GH (2018) Examining levels and factors of speaking anxiety among EFL Libyan English undergraduate students. Int Journal of Applied Linguistics and English Literature 7(5):47–56
Madani خماKA. اضطراب ضغوط ما بعد الصدمة لدى عينة من النازحين بمدينة مصراتة - PTSD amomg Internally displaced person living in Misrata. الرعاية النفسية والاجتماعية لضحايا الثورات والحروب والعنف السياسي- Psychological and social care for victims of revolutions, wars and political violence; بنغازي Benghazi: المنظمة العربية للعمل الاجتماعي والثقافي والتنمية; 2013
Association AP. What is posttraumatic stress disorder (PTSD)? 2000 [Available from: https://www.psychiatry.org/patients-families/ptsd/what-is-ptsd
Cao C, Wang L, Wu J, Bi Y, Yang H, Fang R et al (2020) A comparison of ICD-11 and DSM-5 criteria for PTSD among a representative sample of Chinese earthquake survivors. Eur J Psychotraumatol 11(1):1760481
Boals A, Valentine L (2009) The importance of the DSM-IV E and F criteria in self-report assessments of PTSD. J Anxiety Disord 24:161–166
Boorman RJ, Devilly GJ, Gamble J, Creedy DK, Fenwick J (2014) Childbirth and criteria for traumatic events. Midwifery 30(2):255–261
Stevens A, Fabra M, Thies E (2013) Self-report vs clinical interview for posttraumatic stress disorder in medicolegal assessment. German J Psychiatry 16:87–94
Silveira ER, Cademartori MG, Schuch HS, Armfield JA, Demarco FF (2021) Estimated prevalence of dental fear in adults: a systematic review and meta-analysis. J Dent 108:103632
Melouah A (2013) Foreign language anxiety in EFL speaking classrooms: a case study of first-year LMD students of English at Saad Dahlab University of Blida, Algeria. Arab World Eng J 4(1):64–76. https://awej.org/foreign-language-anxiety-in-efl-speaking-classrooms-a-case-study-of-first-year-lmd-students-of-english-at-saad-dahlab-university-of-blida-algeria/
Organization WH (1998) The global burden of disease: 2004 update: World Health Organization
Arias D, Saxena S, Verguet S (2022) Quantifying the global burden of mental disorders and their economic value. eClinicalMedicine 54:101675
Morina N, Stam K, Pollet TV, Priebe S (2018) Prevalence of depression and posttraumatic stress disorder in adult civilian survivors of war who stay in war-afflicted regions. A systematic review and meta-analysis of epidemiological studies. J Affect Disord 239:328–38
Zuberi A, Waqas A, Naveed S, Hossain MM, Rahman A, Saeed K et al (2021) Prevalence of mental disorders in the WHO Eastern Mediterranean Region: a systematic review and meta-analysis. Front Psych 12:665019
Ouanes S, Bouasker A, Ghachem R (2014) Psychiatric disorders following the Tunisian revolution. J Ment Health 23(6):303–306
Belhadj H, Jomli R (2017) Prevalence of depression in Tunisian general population. Eur Psychiatry 41(S1):S523-S
Jabeur M, Gassab L, Ayadi A, Ben Mohamed B, Zaafrane F, Gaha L (2022) Prevalence and clinical features of anxiety disorders: Tunisian study about 436 subjects. Eur Psychiatry 65(S1):392-S
Rabie M, Sheikh M, ElSayed M, Fekry M, Saad M (2015) Post-traumatic stress disorder and psychiatric comorbidity in a sample of Egyptian adolescents after the revolution: a cross-sectional study. Middle East Curr Psychiatry 22:91–96
Ghanem M, Gadallah M, Meky F, Mourad S, El-Kholy G (2009) National survey of prevalence of mental disorders in Egypt-preliminary survey. East Mediterranean Health J= La revue de santé de la Méditerranée orientale = al-Majallah al-ṣiḥḥīyah li-sharq al-mutawassiṭ 15:65–75
Abuazza A (2013) The Arab spring movement: a catalyst for reform at the psychiatric hospital in Tripoli Libya. Int Psychiatry 10(3):56–58
Okasha A (1999) Mental health services in the Arab world. EMHJ-Eastern Mediterr Health J 5(2):223–230. https://apps.who.int/iris/bitstream/handle/10665/118699/EMHJ_1999_5_2_223_230.pdf?sequence=1
Rhouma AH, Husain N, Gire N, Chaudhry IB (2016) Mental health services in Libya. BJPsych International 13(3):70–71
Salam AA, Alshekteria AA, Mohammed HA, Al Abar NM, Al Jhany MM, Al FF (2012) Physical, mental, emotional and social health status of adolescents and youths in Benghazi Libya. East Mediterr Health J 18(6):586–597
Acknowledgements
I would like to thank my parents and family for their constant support and encouragement throughout my study, special thanks to my supervisor and associate for their review and valuable insight and lastly, I would like to thank JICA for their tremendous support.
Funding
No funding was provided for this study.
Author information
Authors and Affiliations
Contributions
B.D.A was responsible of conceptualization, data curation, formal analysis, investigation, methodology, resources, visualization, writing—original draft preparation. S.D and T.F were responsible for supervision, guidance, writing—review and editing, and final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abuhadra, B.D., Doi, S. & Fujiwara, T. The prevalence of post-traumatic stress disorder, depression, and anxiety in Libya: a systematic review. Middle East Curr Psychiatry 30, 49 (2023). https://doi.org/10.1186/s43045-023-00322-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-023-00322-4