
Abstract
Background
Child maltreatment is a global risk factor for mental health. The burden of child maltreatment is heaviest in low- and lower-middle-income countries, where most of the world’s children live. This study sheds light on the occurrence of child maltreatment within Egypt’s upper social class stratum, countering a long-held belief that violence against children only occurs within low-income households. In addition, the study examines the association between exposure to child maltreatment and psychopathology, life satisfaction and resilience among emerging adults in Egypt, and whether emotion dysregulation mediates these relationships. Participants were 171 college students who were selected based on a series of questionnaires about exposure to child abuse and neglect, psychopathology, satisfaction with life, and resilience, as well as difficulties in emotion regulation.
Results
A rate of 48% of exposure to at least one type of child maltreatment before the age of 18 was found. Experiencing antipathy and/or sexual abuse was most strongly associated with PTSD and depression, while exposure only to antipathy contributed to lower life satisfaction and resilience. Emotion dysregulation mediated the associations between antipathy and PTSD, depression, life satisfaction, and resilience, as well as the associations between sexual abuse and PTSD and depression.
Conclusions
The present study hints at a comparably high rate of exposure to child maltreatment among the higher social class stratum, producing data that highlights the association between child maltreatment and mental health in emerging adults in Egypt. These findings emphasize that child maltreatment transcends social class, and that attempting to address the issue requires changing social and cultural belief systems that bolster violent behavior.
Similar content being viewed by others


“The true character of a society is revealed in how it treats its children.” — Nelson Mandela at the launch of the Blue Train, Worcester Station, Worcester, South Africa, 27 September 1997 [1]
Background
In February 2019, a five-minute video of a mother forcing her 13-year-old son to climb the wall of their building in order to reach the balcony went viral on social media. The boy had misplaced the key to their apartment. While he screamed in fear, his mother continued to beat and push him, pulling him back only when he was near falling (Daily News Egypt). In October of the same year, a 4-year-old girl died in hospital after being tortured by her grandmother and raped by her uncle (Ahram Online). These incidents, among many others, shed light on the social problem of violence against children in Egypt, a lower-middle income (LMIC) Middle Eastern country that sits in the north of the African continent.
In this article, I first shed light on the cultural context that increases the prevalence of child maltreatment (CM) in Egypt. Second, I summarize the existing research on CM and its consequences in adulthood. I then justify the importance of studying emerging adulthood and choice of college students as a sample. Finally, I offer an overview of the present study, along with its findings, limitations and implications.
Shedding light on the Egyptian culture
The Arab culture is characterized by its collectivist nature, which gives precedence to the welfare of the group (i.e., family) over the welfare of the individual [2]. The family is the basic unit of social structure in traditional and contemporary Arab society [3]. The family structure is subject to a set of traditional norms, including protecting the family’s privacy and protecting its reputation amongst the community, which may prevent family members from contacting welfare and health authorities for assistance [4]. Children are consequently raised to be obedient to certain authority figures, particularly those in the family unit. Furthermore, disciplining one’s child by resorting to physical abuse is generally accepted in Egyptian society and because the reputation of the family is prioritized over individual good, children are expected to make sacrifices for the benefit of the family [3]. I argue that collectivism contributes to how individuals and communities justify forms of violence, especially that shame is fueled by the urge to avoid exposure.
Contextualizing child maltreatment
The WHO’s 2014 global status report on violence prevention shows that 36% of Egyptian children were emotionally abused, 23% have been physically abused, 18% of girls and 8% of boys have been sexually abused, and 16% have experienced neglect. Although Egyptian law prohibits the emotional, physical, and sexual exploitation of children [5], exploitation remains prevalent. According to Elghossain et al. [6], Egypt had the highest rate of CM in the Arab region (91%). The deep-rooted cultural model of parental discipline, which includes physically chastising and yelling, legitimizes the use of violence against children [7]. According to the latest nationally representative population survey in Egypt, 93% of children between ages 1 and 14 were exposed to violent disciplinary practices at some point during their childhood. Among the sample (N = 19.474; age range = 15–49), 63% reported “calling the child dumb, lazy or a similar term” at least once during the month before the interview. As for physical punishment, 41.2% reported using severe physical punishment against their children, specifically “hitting or slapping the child on the face, head or ears,” and 11.1% reported “hitting the child over and over and as hard as one can” at least once during the month preceding the interview (Ministry of Health and Population, [8]).
Repercussions of child maltreatment in adulthood
The WHO defines CM as the abuse and neglect of individuals under the age of 18. This includes all forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligence, and exploitation—commercially or otherwise—in the context of a relationship of responsibility, trust, or power that results in actual or potential harm to the child’s health, survival, development, or dignity. Four types of CM are generally recognized: emotional abuse, physical abuse, sexual abuse, and neglect. CM disrupts the caregiver-child bond that is necessary for children’s emotional development [9]. As maltreated children grow up, forming and maintaining bonds could become challenging; they are likely to deal with future emotional connections in a manner that mimics the style of attachment they grew up to learn through their relationship with those who maltreated them, increasing their chance of developing symptoms of psychopathology. Among the deleterious effects in adulthood, a history of antipathy (i.e., emotional abuse), physical and sexual abuse, and/or neglect is linked to risks of posttraumatic stress disorder (PTSD) [10], depression [11], lower satisfaction with life [12], and lower resilience [13]. One possible link between CM, PTSD, depression, life satisfaction, and resilience is difficulty in emotion regulation [14].
CM leaves children feeling terrorized [10], which potentially impairs the integration of the CM experience into memory, resulting in PTSD [15]. Although all forms of CM are associated with PTSD, effects are stronger for antipathy and sexual abuse [10]. The link between sexual abuse and PTSD has long been documented, having been demonstrated in a 30-year longitudinal study by Fergusson et al. [16]. Relating to negative evaluation by an attachment figure, antipathy is potent in causing emotion dysregulation and negative emotions, including shame, which can explain the link between antipathy and PTSD [17]. Antipathy negatively affects children’s attachment style, which shapes individuals’ internal working models [9]. Such negative working models, in turn, anticipate depression [11]. Sexual abuse disrupts children’s sense of trust, which is also associated with depression [18] as well as their world view [19]. The current investigation suggests that sexual abuse is the strongest correlate to depression when compared to other forms of CM [10]. To summarize, both antipathy and sexual abuse, in comparison to physical abuse and neglect, are more strongly associated with PTSD and depression.
CM also affects adult individuals’ subjective life satisfaction [20]. A 19-year longitudinal study by Mosley-Johnson et al. [12] found a negative association between CM and life satisfaction. Fortunately, some who are maltreated as children overcome the adverse consequences and grow up to be resilient [13]. In this context, resilience is the potential to thrive despite having experienced severe stressors. It is therefore best studied longitudinally (e.g., [20]). Individuals with a history of CM tend to be less resilient to stressors later in life. Some traits and skills that contribute to resilience, such as psychological hardiness, ego resilience, and coping efficacy have been measured by self-reporting [21].
Furthermore, CM interferes with the development of the six strategies of emotion regulation abilities, namely acceptance, avoidance, problem solving, reappraisal, rumination, and suppression [22]. Emotion regulation is, in turn, associated with mental health [14]. On the one hand, emotion dysregulation predicts PTSD through thought suppression, avoidance and rumination, and it predicts depression through the inability to regulate affect [23]. Experiencing higher negative emotions due to low reappraisal and rumination [11], in turn, predicts lower life satisfaction [24]. On the other hand, resilient individuals use two emotion regulation strategies [25]: attentional control, to shift focus from negative experiences, and reappraisal, to focus on positive emotions. Since emotion regulation is instrumental for developing resilience—and because it is predicted by CM —[23] emotion regulation is shown to mediate the association between CM and resilience.
The right and duty to produce data about child maltreatment
The international community recognizes violence against children as a public health and human rights problem, both globally and within the 22 countries of the Arab League. Simultaneously, given the political events in the Middle East, Arabs have increasingly become the focus of media attention [26]. Thus, there is a growing need for accurate information regarding Arab culture in order to better aid assessment and treatment of CM in Arab countries. Egypt is currently undergoing political and economic turmoil due to the regime’s implementation of a number of policies which led to unprecedented inflation rates that have reached 23.2% in 2016 compared to 9% in 2011 [27]—that directly impacts social and familial dynamics—which might lead to increased levels of violence, including community violence, and possibly CM. It has been established in the existing literature that economic hardships are associated with adverse changes in the parenting of children, including maternal child abuse and neglect [28]. In this regard, Le Minh et al. [29] argue that high rates of CM in LMICs exist in tandem with high rates of community violence. Evidence that violence increases the chances of developing short- and long-term negative mental health issues has led to calls for greater attention to violence as a determinant of mental health, especially among young people [6].
Most research on CM in Egypt focuses on risk factors [30], external symptoms [31], and socioeconomic predictors [32]. Other studies that investigate the problem of CM focus on data from emergency or clinical departments, criminal records or autopsy reports (e.g., [33]). To the best of our knowledge, only three studies examined CM among Egyptian college students (N = 450; 52% females [34];; N = 1270; 100% females [35];; N = 963; 64% females [36];). While one of the three studies only reported prevalence of sexual abuse [34], Mansour et al. [36] and Mahrous et al. [35] found that CM correlated with negative outcomes using instruments that were only designed for these studies. The lack of use of existing and validated instruments hinders the comparison of findings with other studies. In addition, none of the three studies investigated the relations of interest here, namely the correlation of CM with PTSD, depression, life satisfaction, and resilience, nor did they examine the mediating role of emotion dysregulation. Thus, the existing literature leaves important questions regarding CM unanswered. Most importantly, most research done on CM in Egypt is based on samples from lower socioeconomic statuses (SES) (Mohammad & Samak, 2017), including the three aforementioned studies. While findings refer to low parental education as a positive predictor of CM [37], our research shows that CM transcends social class [38]. Therefore, this study contributes to the body of limited information on CM in emerging adults from middle and higher SES in Egypt. Emerging adulthood is a developmental stage marked by greater independence, exploration, and uncertainty [39]. It is understandably a period of vulnerability for psychopathology. There is a large body of research establishing CM as a risk factor for multiple negative outcomes in both adolescence and adulthood. Yet studies have relatively neglected emerging adulthood [38].
The present study
The present study aimed to replicate findings about associations between CM and PTSD, depression, life satisfaction, and resilience, as well as investigate the mediating role of emotion regulation in a sociocultural context not yet well studied: well-educated emerging adults in Egypt. This study was motivated by two objectives: (1) contributing to the literature on CM in Arab countries and (2) advancing the study of CM in higher SES in Egypt. I hypothesized a positive association between CM and psychopathology (H1) and a negative association between CM, life satisfaction and resilience (H3). Specifically, I hypothesized that antipathy and sexual abuse contributed most to both associations (H2, H4). Second, I aimed at elucidating the mechanisms by which the forms of CM exerted their relative influence on psychopathology and life satisfaction. Specifically, I hypothesized that emotion dysregulation mediates the relationship between each CM form and psychopathology (H5), as well as life satisfaction and resilience (H6).
Methods
Participants
Students from various disciplines were recruited at a private English-speaking university in Cairo, using two strategies: (1) presenting the study inside classrooms (81.3%) and (2) advertising on Facebook groups used by students (18.7%). Recruitment materials explained that the study investigates how individuals’ experiences with their families affected them. Using Cochran’s formula, the sample size was set to 150 participants. Out of 505 students approached in 35 classes, 45.9% (N = 232) expressed interest in the study, of whom 79.3% (N = 184) participated, a rate that is consistent with similar studies [40]. Thirteen students were excluded because they fulfilled at least one of the three exclusion criteria: (1) risk for psychosis, (2) substance abuse, and (3) suicidality. The final sample included 171 emerging adults (M = 20.46 years, SD = 1.87; 74.9% females).
Procedures
Data was collected between April and November 2019. Participants were informed that if they expressed suicidal ideations, they would be referred to the student counseling center. Written informed consent was obtained. In a single 2-h session in an office on campus, self-report instruments were administered. The study was divided into three sections: (1) screening for CM and assessment of PTSD and resilience, (2) narrative interviews reported elsewhere [41], and (3) assessment of depression and emotion regulation. In compensation for their time, participants received vouchers for on-campus outlets worth 100 Egyptian pounds. A referral booklet that included contact information for mental health professionals in different geographical areas in Cairo was offered to all participants. Exclusion criteria were pre-determined in order to avoid causing further distress to participants.
Measures
Exclusion criteria
The Prodromal Questionnaire-16 (PQ-16 [42];) includes 16 yes/no items about psychotic symptoms (cut-off = 9). The Drug Abuse Screening Test (DAST-10 [43];) and the Alcohol Use Disorders Identification Test (AUDIT [44];) each includes 10 items (cut-off = 6 and 16, respectively). The Columbia-Suicide Severity Rating Scale (C-SSRS [45];) includes six yes/no items (cut-off = 2).
Child maltreatment
The Childhood Experience of Care and Abuse Questionnaire (CECA.Q [46];) is a retrospective assessment of antipathy, physical and sexual abuse, and neglect. Test-retest reliability over 2 years was reported for antipathy (r =.71), physical abuse (r = .51), sexual abuse (r = .61), and neglect (r = .53–.84). The cut-off scores recommended by the authors were used to categorize participants who were exposed to maltreatment [46]. Antipathy and neglect were each assessed using eight items, filled in separately for each parental figure. Physical abuse was probed with one question. If answered affirmatively, participants answered four additional questions (frequency of hitting, the type of implement used, resulting injuries, and whether the perpetrator was out of control). Sexual abuse was probed with three questions, e.g., “When you were a child or teenager, did you ever have any unwanted sexual experiences?” If at least one of them was answered affirmatively, seven more questions were asked (e.g., frequency of sexual abuse, relationship with the perpetrator, characteristics of experience).
Symptoms of PTSD and depression, life satisfaction, resilience, and emotion dysregulation
PTSD
The Posttraumatic Stress Disorder Checklist for DSM–5 (PCL-5 [47];) includes 20 items assessing symptoms on a five-point scale. The questions are asked on a Likert scale from 0 (not at all) to 4 (extremely). There was a high internal consistency with Cronbach’s α = .96. Participants were asked to answer the scale in reference to the most stressful event in their family before age 18.
Depression
The revised version of the Center for Epidemiological Studies Depression Scale (CESD-R [48];) includes 20 items assessing symptoms on a five-point scale. The questions are asked on a Likert scale from 1 (rarely or none of the time) to 4 (most or all of the time). The CES-D has been found to have adequate internal consistency (current study α =.74) and test-retest reliability [49].
Life satisfaction
The Satisfaction with Life Scale (SWLS [50];) includes five items assessing the overall quality of life on a seven-point scale. All items are scored by a seven-point Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree). According to Diener and co-workers, the SWLS has been demonstrated to have strong internal consistency and moderate temporal stability with Cronbach's alpha of 0.87 and 2-month test-retest reliability of 0.82.
Resilience
The Connor-Davidson Resilience Scale (CD-RISC-10 [51];) includes 10 items assessing tolerance of negative affect, ability to focus under pressure, and an action-oriented approach to problem solving on a four-point scale. Respondents rate items on a scale from 0 (not true at all) to 4 (true nearly all the time). A preliminary study of the psychometric properties of the CD-RISC in general population and patient samples supported its internal consistency, test–retest reliability, and convergent and divergent validity [21].
Emotion dysregulation
The short version of the Difficulties in Emotion Regulation Scale (DERS-SF [52];) includes 18 items assessing emotion regulation strategies on a five-point scale from 0 (almost never) to 4 (almost always). The DERS demonstrated adequate factorial validity as well as internal consistency (.76–.87 and .85 to .94, respectively) [14].
Data analysis plan
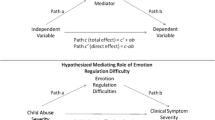
All data met assumptions of linearity, multicollinearity, homoscedasticity, and normally distributed errors. Two outliers were winsorized. Sociodemographic variables that correlated with the dependent variables were controlled in all tests of hypotheses: age, SES, and prior therapy experience. The hypotheses that CM is positively associated to psychopathology (H1) and negatively to life satisfaction and resilience (H3), and that antipathy and sexual abuse are the strongest correlates to the dependent variables (H2, H4) were tested in four multiple regressions, one for each dependent variable: PTSD, depression, and satisfaction with life and resilience. The control variables—age, SES, and therapy experience—were entered in step 1 and the continuous variables for the four CM (antipathy, physical abuse, sexual abuse, and neglect) forms were entered in step 2. The hypotheses that emotion dysregulation mediated the association between CM and psychopathology (H5) and life satisfaction and resilience (H6) were tested separately for each of the four dependent variables by using PROCESS Macro V3.5 [53] to determine whether emotion dysregulation predicted the dependent variables, and whether it reduced or eliminated the predictive value of CM forms. Control variables were included in the mediation analysis.
Results
Descriptive statistics
Sample characteristics and correlations between variables are reported for descriptive purposes (see Tables 1 and 2). With regard to social class, 18.1% (n = 31) of the participants classified themselves socially as being middle class as middle social class, 59.6% (n = 102) upper middle class, or upper class (n = 38; 22.2%). Almost half of the sample (48%; n = 89) had experienced some form of CM before the age of 18. Of these 89 participants, 30.4% (n = 52) experienced physical abuse, 21.1% (n = 36) experienced sexual abuse, 14.6% (n = 25) experienced antipathy, and 9.4% (n = 15) experienced neglect during childhood. It is important to note that these types of CM are not mutually exclusive; 54.9% (n = 45) of those who have been exposed to CM experienced only one type of abuse or neglect, while 34.1% (n = 28) experienced two types, and 11% (n = 9) experienced three types of CM. With regard to perpetrators of CM, 48% (n = 12) of those exposed to antipathy indicated that it was by their father, 36% (n = 9) by their mother, and 16% (n = 4) by both parents. Moreover, 40.4% (n = 21) reported being physically abused by their father, 36.5% (n = 19) by their mother, and 23% (n = 12) by both. Of those having experienced neglect, it was reported that 75% (n = 12) experienced it from the father, 12.5% (n = 2) from the mother, and 12.5% (n = 2) from both parents. Finally, sexual abuse was reported to have been experienced by someone known to the person among 55.6% (n = 20) of participants, by a household member or a relative by 41.7% (n = 15), and by a stranger among 2.8% (n = 1). It is important to note, however, that none of those who experienced sexual abuse reported that either parent was the perpetrator.
CM correlates with psychopathology in emerging adulthood
H1, that CM correlates with psychopathology, was confirmed for both PTSD (F(4, 163) = 10.18, p < .001, R2 = .24) and depression (F(4, 163) = 8.87, p < .001, R2 = .24), as was hypothesis 2, that CM correlates with both satisfaction with life (F(4, 163) = 5.61, p < .001, R2 = .16) and resilience (F(4, 163) = 4.40, p < .001, R2 = .17).
Antipathy and sexual abuse correlate the strongest with psychopathology, life satisfaction and resilience in emerging adulthood
Hypotheses 3 and 4—which predicted that amongst the four forms of CM, antipathy and sexual abuse have the strongest correlation to the outcome variables—were partially supported. Only antipathy, and not sexual abuse nor any other CM form, correlated with life satisfaction and resilience (see Table 3).
Emotion dysregulation
Hypotheses 5 and 6—which expected emotion dysregulation to mediate the association between CM and the outcome variables. Both the prediction of the mediator by antipathy and sexual abuse was significant, as were the correlations between emotion regulation and the four dependent variables (see Table 2). Antipathy correlated with all four variables, while sexual abuse only correlated with two (see Table 3). Therefore, six mediation models were run, four with antipathy as predictors and two with sexual abuse (see Table 4). For antipathy, emotion dysregulation reduced the predictive value of antipathy for PTSD and satisfaction with life (partial mediations), while eliminating those for depression and resilience (full mediations). For sexual abuse, emotion dysregulation reduced the predictive value of sexual abuse for PTSD (partial mediation) and eliminated it for depression (full mediation).
Discussion
The overarching goal of this study was to examine the association between CM and psychopathology, life satisfaction and resilience among well-educated emerging adults. I hypothesized that antipathy and sexual abuse are the strongest correlates to psychopathology, life satisfaction, and resilience and that emotion dysregulation mediates these associations. The results partially supported the hypotheses. Antipathy and sexual abuse were associated with both PTSD and depression. However, only antipathy correlated negatively with resilience and life satisfaction. Emotion dysregulation mediated all these associations.
The present study reveals that 48% of the sample (N = 82) was exposed to at least one type of CM. Our findings are consistent with the literature on the effects of CM in adulthood. What the present study adds to this body of knowledge is an illustration of the impact of CM in emerging adults in Egypt, and that violence, and specifically parental violence against children, cuts through social and economic lines.
In earlier studies on Egypt, Mansour et al. [36] reported rates of 2.1% for antipathy, 3% for physical abuse, 5% for sexual abuse, and 7% for neglect among college students (N = 963; 63.9% females) using an Arabic version of the Childhood Trauma Questionnaire (CTQ [54];). Using a different translated version of the CTQ, Mahrous et al. [35] reported rates of 40.26% for antipathy, 40.28% for physical abuse, 33.05% for sexual abuse, and 49.73% for neglect among a sample of female college students (N = 1270). Aboul-Hagag and Hamed [34] reported a rate of 29.8% for sexual abuse among a sample of college students (N = 450; 51.8% females) using the Finkelhor’s [55] questionnaire.
Among survivors of CM, our results showed increased PTSD and depression in emerging adulthood, lower life satisfaction and lower resilience. The present study confirms evidence that CM increases the risk for psychopathology. Consistent with other studies (e.g., [10]), antipathy and sexual abuse had the strongest association to PTSD, in comparison to physical abuse and neglect. As hypothesized, antipathy was strongly associated with lower life satisfaction, paralleling recent findings in China, a similarly collectivistic culture [24], as well as those in western countries [12]. These findings confirm that CM is an important environmental factor that leads to lower life satisfaction in adulthood in middle to high socioeconomic classes in Egypt. Moreover, it corroborates findings that CM, especially parental antipathy, reduces resilience in adulthood [24].
Sexual abuse did not correlate with resilience or satisfaction with life, contradicting earlier findings, which could be understood through examining two main factors. First, in the current sample, sexual abuse was not found to be perpetrated by any of the parents, but rather by other persons of trust (55.6% by someone known to the family, 41.7% by a household member or a relative, and 2.9% by a stranger). While these findings call for an exploration as to why no sexual abuse by a parent was reported, survivors might have benefited from individual and environmental protective factors that moderated their experience, possibly lessening its long-term effect. In a meta-analysis by Ventus et al. [56], intrafamilial sexual abuse was associated with an earlier age of onset, which results in more serious sequelae due to an expectedly longer duration of abuse. When sexual abuse is inflicted by a trusted adult, it may be hard for children to view the perpetrator in a negative light, thus pushing them to blame themselves for the event [57]. Second, 65.7% of those who were sexually abused (n = 23) experienced it more than once. The remaining 34.3% were abused only once. Prolonged maltreatment has been studied in comparison to singular events in childhood [13]. Conversely, cumulative trauma over the course of a lifetime correlated with higher levels of psychological distress [58].
Therefore, the finding of a significantly negative association between antipathy and life satisfaction and/or resilience concurs with the literature. As for sexual abuse, the results reflect the fact that many of those exposed to this form of CM only experienced it once, which might have not affected their satisfaction with life and resilience as much as cumulative stress during childhood would (i.e., antipathy). Prolonged stress has been shown to be the strongest contributor to symptom complexity, which is often marked by difficulties with emotion regulation [58]. Longitudinal studies show that emotion dysregulation is a connecting factor between CM, PTSD, and depression [10, 59]. The study highlights this correlation, confirming earlier results [23].
This study has two main limitations. First, the design of the study does not exclude a retrospective bias in its assessment of CM. In addition, it does not allow us to draw conclusions about causal relations between CM and the outcomes. Second, the findings have limited generalizability as the selected sample is nonrepresentative of the Egyptian population. Further research can help us to better understand cultural norms regarding discipline, especially physical punishment and abuse. Conducting research among a more representative sample of the general population would allow for a better understanding of the repercussions of CM in emerging adulthood across Egypt as a whole. A potential inquiry for future research is to examine people’s knowledge, attitudes and reporting behavior of CM in order to address deep-rooted cultural beliefs that contribute to the prevalence of violence against children.
Conclusions
The findings of this study are useful for stakeholders in Egypt, specifically families as well as policymakers working in the field of childcare, particularly as it challenges the assumption that CM is only comorbid among families in lower SES. A comprehensive understanding of the negative impacts of CM on individuals throughout their lifespan can provide support for awareness and advocacy initiatives on the indelible effects of violence against children across all social strata. While the findings are consistent with evidence from Western countries with regard to the particularly detrimental effect of antipathy and sexual abuse, this study has important implications for practitioners as it shows that CM has diverse and complex sequelae that extend over time in the Egyptian culture. Without undermining the negative consequences of physical abuse in adulthood, this data highlights the importance of examining the characteristics of childhood physical abuse, its perception among youngsters, as well as the potential ramifications it has, whether on the individual (e.g., other forms of psychopathology) or family (e.g., domestic violence) or on society (e.g., social violence) as a whole. These findings are essential to parents, health planners, and policy makers in proposing strategies to help prevent mental health problems that can persist into adulthood. Finally, the study’s findings call for a stronger enforcement of the existing children’s rights and protection laws in place.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CM:
-
Child maltreatment
- LMIC:
-
Lower-middle income country
- PTSD:
-
Posttraumatic stress disorder
- WHO:
-
World Health Organization
References
Lynch, Vivian Valvano. “The country of the young: interpretations of youth and childhood in Irish culture Ed. by John Countryman and Kelly Matthews (review).” New Hibernia Review, vol. 18, no. 1, Center for Irish Studies at the University of St. Thomas, 2014, pp. 157–159. https://doi.org/10.1353/nhr.2014.0016,
Erickson CD, Al-Timimi NR (2001) Providing mental health services to Arab Americans: recommendations and considerations. Cultur Divers Ethnic Minor Psychol 7(4):308–327. https://doi.org/10.1037/1099-9809.7.4.308
Dwairy M (2004) Parenting styles and mental health of Palestinian–Arab adolescents in Israel. Transcult Psychiatry 41(2):233–252. https://doi.org/10.1177/1363461504043566
Haj-Yahia MM (2001) The incidence of witnessing interparental violence and some of its psychological consequences among Arab adolescents. Child Abuse Negl 25(7):885–907. https://doi.org/10.1016/S0145-2134(01)00245-9
Egypt (2008) Law No. 12 of 1996 Promulgating the Child Law Amended by Law No. 126 of. Al-Jarida Al-Rasmiya 39(13):2–47
Elghossain T, Bott S, Akik C, Ghattas H, Obermeyer CM (2019) Prevalence of key forms of violence against adolescents in the Arab Region: a systematic review. J Adolesc Health 64(1):8–19. https://doi.org/10.1016/j.jadohealth.2018.08.016
Mohammed NY, Samak YAA (2017) Spoil the rod and save the child: Socioeconomic predictors of harsh discipline by parents, Egyptian case study. J Interpers Violence 32(11):1730–1752. https://doi.org/10.1177/0886260517698703
Ministry of Health and Population, El-Zanaty and Associates, and ICF International. (2015). Egypt demographic health survey. Ministry of Health and Population and ICF International.
Bowlby J (1969) Attachment: attachment and loss. Basic, New York
Messman-Moore TL, Bhuptani PH (2017) A review of the long-term impact of child maltreatment on posttraumatic stress disorder and its comorbidities: an emotion dysregulation perspective. Clin Psychol Sci Pract 24(2):154–169. https://doi.org/10.1111/cpsp.12193
Infurna MR, Reichl C, Parzer P, Schimmenti A, Bifulco A, Kaess M (2016) Associations between depression and specific childhood experiences of abuse and neglect: a meta-analysis. J Affect Disord 190:47–55. https://doi.org/10.1016/j.jad.2015.09.006
Mosley-Johnson E, Garacci E, Wagner N, Mendez C, Williams JS, Egede LE (2019) Assessing the relationship between adverse childhood experiences and life satisfaction, psychological well-being, and social well-being: United States Longitudinal Cohort 1995–2014. Qual Life Res 28(4):907–914. https://doi.org/10.1007/s11136-018-2054-6
Ben-David V, Jonson-Reid M (2017) Resilience among adult survivors of childhood neglect: a missing piece in the resilience literature. Child Youth Serv Rev 78:93–103. https://doi.org/10.1016/j.childyouth.2017.05.014
Jennissen S, Holl J, Mai H, Wolff S, Barnow S (2016) Emotion dysregulation mediates the relationship between child maltreatment and psychopathology: a structural equation model. Child Abuse Negl 62:51–62. https://doi.org/10.1016/j.chiabu.2016.10.015
Horowitz MJ (1997) Stress response syndromes: PTSD, grief, and adjustment disorders (3rd ed.). Jason Aronson, Northvale
Fergusson DM, McLeod GF, Horwood LJ (2013) Childhood sexual abuse and adult developmental outcomes: findings from a 30-year longitudinal study in New Zealand. Child Abuse Negl 37(9):664–674. https://doi.org/10.1016/j.chiabu.2013.03.013
Spinazzola J, Van der Kolk B, Ford JD (2018) When nowhere is safe: interpersonal trauma and attachment adversity as antecedents of posttraumatic stress disorder and developmental trauma disorder. J Trauma Stress 31(5):631–642. https://doi.org/10.1002/jts.22320
Cutajar MC, Mullen PE, Ogloff JR, Thomas SD, Wells DL, Spataro J (2010) Psychopathology in a large cohort of sexually abused children followed up to 43 years. Child Abuse Negl 34(11):813–822. https://doi.org/10.1016/j.chiabu.2010.04.004f
Ferrajão PC, Elklit A (2020) World assumptions and posttraumatic stress in a treatment-seeking sample of survivors of childhood sexual abuse: a longitudinal study. Psychol Violence 10(5):501–508. https://doi.org/10.1037/vio0000280
Klika JB, Herrenkohl TI (2013) A review of developmental research on resilience in maltreated children. Trauma, Violence, & Abuse 14(3):222–234. https://doi.org/10.1177/1524838013487808
Connor KM, Davidson JRT (2003) Development of a new resilience scale: the Connor–Davidson Resilience Scale (CD-RISC). Depress Anxiety 18(2):76–82. https://doi.org/10.1002/da.10113
Gratz KL, Roemer L (2004) Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess 26(1):41–54. https://doi.org/10.1023/B:JOBA.0000007455.08539.94
Villalta L, Smith P, Hickin N, Stringaris A (2018) Emotion regulation difficulties in traumatized youth: a meta-analysis and conceptual review. Eur Child Adolesc Psychiatry 27(4):527–544. https://doi.org/10.1007/s00787-018-1105-4
Xiang Y, Yuan R, Zhao J (2020) Childhood maltreatment and life satisfaction in adulthood: the mediating effect of emotional intelligence, positive affect and negative affect. J Health Psychol. 26(13):2460–2469. https://doi.org/10.1177/1359105320914381
Troy AS, Mauss IB (2011) Resilience in the face of stress: emotion regulation as a protective factor. Resilience and mental health: challenges across the lifespan 1(2):30–44. https://doi.org/10.1017/CBO9780511994791.004
Comunello F, Anzera G (2012) Will the revolution be tweeted? A conceptual framework for understanding the social media and the Arab Spring. Islam and Christian–Muslim Relations 23(4):453–470. https://doi.org/10.1080/09596410.2012.712435
Central Bank of Egypt. (2018). Central Bank of Egypt Database [Database]. Retrieved from http://www.cbe.org.eg/en/EconomicResearch/Statistics/Pages/Inflationhistorical.aspx
Schneider W, Waldfogel J, Brooks-Gunn J (2017) The Great Recession and risk for child abuse and neglect. Child Youth Serv Rev 72:71–81. https://doi.org/10.1016/j.childyouth.2016.10.016
Le Minh TH, Holton S, Romero L, Fisher J (2018) Polyvictimization among children and adolescents in low- and lower-middle-income countries: a systematic review and meta-analysis. Trauma Violence Abuse 19(3):323–342. https://doi.org/10.1177/1524838016659489
Afifi ZEM, El Lawindi MI, Ahmed SA, Basily WW (2003) Adolescent abuse in a community sample in Beni Suef, Egypt: Prevalence and risk factors. East Mediterr Health J 9(5-6):1003–1018. https://doi.org/10.26719/2003.9.5-6.1003
El-Baz RH, Abo-El-Ezz WF, El-Hadidy MA, El-Boraie HA (2016) Child abuse experiences in adolescents with externalizing disorders. Egypt J Psychiatry 37(2):46. https://doi.org/10.4103/1110-1105.193021
Khalifa HA (2017) Physical punishment of children: dimensions and predictors in Egypt. Int J Psychol Behav Sci 7(1):32–40. https://doi.org/10.5923/j.ijpbs.20170701.06
El-Elemi AH, Moustafa SM (2013) Review of 89 autopsies of child deaths from violence and neglect in the Suez Canal area, Egypt. Egypt J Forensic Sci 3(4):116–122. https://doi.org/10.1016/j.ejfs.2013.07.002
Aboul-Hagag KES, Hamed AF (2012) Prevalence and pattern of child sexual abuse reported by cross sectional study among the university students, Sohag University, Egypt. Egypt J Forensic Sci 2(3):89–96. https://doi.org/10.1016/j.ejfs.2012.05.001
Mahrous E, Abd Elazem S, Hassan Z (2016) Prevalence of child abuse and its long-term psychological consequences among female students of medical faculties. Int J Sci Res 5(10). https://doi.org/10.21275/ART20162127
Mansour K, Roshdy E, Daoud O (2010) Child abuse and its long-term consequences: an exploratory study on Egyptian university students. Arab J Psychiatry 44(2299):1–54
Antai D, Braithwaite P, Clerk G (2016) Social determinants of child abuse: evidence of factors associated with maternal abuse from the Egypt demographic and health survey. J Inj Violence Res 8(1):25–34. https://doi.org/10.5249/jivr.v8i1.630
Toth SL, Cicchetti D (2013) A developmental psychopathology perspective on child maltreatment. Child Maltreat 18(3):135–139. https://doi.org/10.1097/00004583-199505000-00008
Arnett JJ (2000) Emerging adulthood: a theory of development from the late teens through the twenties. American Psychologist 55(5):469–480. https://doi.org/10.1037/0003-066X.55.5.469
Fincham JE (2008) Response rates and responsiveness for surveys, standards, and the journal. Am J Pharm Educ 72(2):43. https://doi.org/10.5688/aj720243
Fishere M., & Habermas, T. (2021). Evaluation and immersion in child maltreatment narratives by emerging adults [unpublished manuscript]. Department of Psychology, Goethe University Frankfurt.
Ising HK, Veling W, Loewy RL, Rietveld MW, Rietdijk J, Dragt S, Van Der Gaag M (2012) The validity of the 16-item version of the Prodromal Questionnaire (PQ-16) to screen for ultra-high risk of developing psychosis in the general help-seeking population. Schizophr Bull 38(6):1288–1296. https://doi.org/10.1093/schbul/sbs068
Skinner HA (1982) Guide for using the drug abuse screening test (DAST). Addict Behav 7(4):363–371. https://doi.org/10.1016/0306-4603(82)90005-3
Babor TF, de la Fuente JR, Saunders J, Grant M (1992) AUDIT: the alcohol use disorders identification test: guidelines for use in primary health care. In: AUDIT: the alcohol use disorders identification test: guidelines for use in primary health care. World Health Organization
Posner K, Brent D, Lucas C, Gould M, Stanley B, Brown G et al (2008) Columbia-suicide severity rating scale (C-SSRS). Columbia University Medical Center, New York, NY
Bifulco A, Bernazzani O, Moran PM, Jacobs C (2005) The childhood experience of care and abuse questionnaire (CECA. Q): validation in a community series. Br J Clin Psychol 44(4):563–581. https://doi.org/10.1348/014466505X35344
Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP, Schnurr PP (2013) The PTSD checklist for DSM-5 (PCL-5). Scale available from the National Center for PTSD
Eaton W, Muntaner C, Smith C, Tien A, Ybarra M (2004) Center for Epidemiologic Studies Depression Scale: review and revision (CESD and CESD-R). In: Maruish M (ed) The use of psychological testing for treatment planning and outcomes assessment, 3rd edn. Lawrence Erlbaum, Mahwah, NJ, pp 363–377
Devins GM, Orme CM, Costello CG, Binik YM (1988) Measuring depressive symptoms in illness populations: psychometric properties of the Center for Epidemiologic Studies Depression (CESD) scale. Psychol Health 2(2):139–156. https://doi.org/10.1080/08870448808400349
Diener ED, Emmons RA, Larsen RJ, Griffin S (1985) The satisfaction with life scale. J Pers Assess 49(1):71–75. https://doi.org/10.1207/s15327752jpa4901_13
Campbell-Sills L, Stein MB (2007) Psychometric analysis and refinement of the Connor–Davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress 20(6):1019–1028. https://doi.org/10.1002/jts.20271
Kaufman EA, Xia M, Fosco G, Yaptangco M, Skidmore CR, Crowell SE (2016) The difficulties in emotion regulation scale short form (DERS-SF): validation and replication in adolescent and adult samples. J Psychopathol Behav Assess 38(3):443–455. https://doi.org/10.1007/s10862-015-9529-3
Hayes AF (2017) Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. Guilford publications, New York
Bernstein DP, Fink L (1998) Childhood Trauma Questionnaire: a retrospective self-report manual. The Psychological Corporation, San Antonio, TX
Finkelhor D (1979) Sexually victimized children. Free Press, New York, NY
Ventus D, Antfolk J, Salo B (2017) The associations between abuse characteristics in child sexual abuse: a meta-analysis. J Sex Aggression 23(2):167–180. https://doi.org/10.1080/13552600.2017.1318963
Hall, M., & Hall, J. (2011). The long-term effects of childhood sexual abuse: counseling implications. http://counselingoutfitters.com/vistas/vistas11/Article_19.pdf.
Cloitre M, Stolbach BC, Herman JL, Kolk BVD, Pynoos R, Wang J, Petkova E (2009) A developmental approach to complex PTSD: childhood and adult cumulative trauma as predictors of symptom complexity. J Trauma Stress 22(5):399–408. https://doi.org/10.1002/jts.20444
Kim J, Cicchetti D (2010) Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. J Child Psychol Psychiatry 51(6):706–716. https://doi.org/10.1111/j.1469-7610.2009.02202.x
Acknowledgements
I thank Prof. Dr. Tilmann Habermas (Goethe University Frankfurt, Germany) for his continuous supervision of my work, extensive feedback concerning this draft, and all his valuable support. I thank Dr. Yasmine Saleh, Mariam Arafa, Sarah Ismail, Safeya Abouzeid (American University in Cairo, Egypt), and Raghda El-Qabbage (Cairo University, Egypt) for providing me with support during the data collection period.
Funding
This work was partially funded by the German Business Foundation (Stiftung der deutschen Wirtschaft).
Author information
Authors and Affiliations
Contributions
MF is the sole author of this work. The author read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the American University in Cairo’s Institutional Review Board (#2018-2019-109).
Consent for publication
The study has received consent for publication from the Institutional Review Board as well as from all participants who signed the consent form stating this purpose.
Competing interests
The author declares that she has no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fishere, M. The ripple effect: a cross-sectional study on the repercussions of child maltreatment among Egyptian college students. Middle East Curr Psychiatry 28, 69 (2021). https://doi.org/10.1186/s43045-021-00147-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-021-00147-z